INTRODUCTION
Arthrodesis has been recognized and has gained general acceptance as the golden standard in surgical treatments of chronic discogenic back pain in degenerative disc diseases (DDD)83). However, various fusion-related complications such as incorrect placement of screws, breakage of metallic implants, nonunion, have been observed during follow-up for a long time40). Besides, adjacent segment disease and dissociation between fusion rate and clinical success rate have received more serious attention from surgeons over time30). These shortcomings of arthrodesis motivated spine surgeons to take account of a substitute for arthrodesis.
Theoretically, it was anticipated that lumbar total disc replacement (LTDR) would replace arthrodesis in the management of chronic discogenic back pain because it was expected to reduce various intra- and post-operative complications particularly related with fusion and adjacent segment disease (ASD). LTDR is indicated in chronic back pain arising from the disc per se, so called discogenic back pain in patients with DDD. However, clinical relevancy of LTDR in general practice of spine surgery is undetermined yet. Most of the investigators studying clinical relevancy of LTDR by following up LTDR patients and reviewing LTDR articles insisted that indications for LTDR are not extensive but limited. Some investigators insisted that LTDR could only be used for investigational use42,7983). In addition, mid- and long-term follow-up results brought about new modes of clinical failure, quite different from complications of arthrodesis such as wear-debris induced osteolysis80). Recently in more than 5-year follow-up outcome results of some randomized comparison studies between arthrodesis and LTDR, LTDR has appeared to be non-inferior compared to arthrodesis, while rather surpassing in the result of certain minor follow-up parameters35,86).
Arthrodesis is known to be the counterpart and an inevitable comparator of LTDR. Practically, the main difference that sets LTDR and arthrodesis apart is motion preservation or motion sacrificed. In LTDR, a mobile is implanted to replace the disc that is totally removed in order to treat discogenic back pain during surgical procedures. The devices and technologies in the motion preservation surgery in the lumbar spine can be divided into four groups : 1) Total disc replacement (TDR), 2) Nucleus replacement, 3) Intra-disc biologic treatments, 4) Posterior dynamic stabilization including total facet replacement43). These implants and technologies have not been widely practiced and have very limited literatures relatively in the lower grade of evidence except for LTDR55). Therefore the present article is limited only to LTDR. This implant was generally introduced to medical community and widely applied to their clinical practice between late 1990s and early 2000s. More than 10 years have passed since then. Now, it seems to be the right time to sum up clinical results, and these results obviously present desirable information related with LTDR's clinical relevancy.
In the present study, the Author has reviewed the articles, which dealt with relevancy and efficacy of LTDR in the treatment of DDD, and draws a conclusion from these review results. At the beginning of this article, the clinical characteristics of DDD are briefly reviewed for readers to better understand the role of LTDR in the management of DDD.
PATHOGENESIS, DIAGNOSIS AND MANAGEMENTS OF DDD
Degenerative disc disease (DDD) is a complex degenerative cascade due to age-related changes in molecular composition of the disc65,74), which often occurs at a faster rate in patients of working age and gives rise to clinical sequel of substantial impairment in the patients. However, the question of what the most proper approach is in the management of a patient with symptomatic DDD is still on debate63), though intractable discogenic back pain is known as the most common type of chronic LBP and the most common cause of axial back pain22). Practically, there have been various kinds of interventional and surgical managements for a patient with intractable discogenic back pain. Therefore, clinicians need to understand pathogenesis and clinical relevance of DDD, with which they could select a proper means for diagnosis and managements of symptomatic DDD.
Pathogenesis of discogenic back pain
The existence, nature and mechanism of discogenic back pain may be the subject of the most controversy. Opponents of discogenic pain hypothesis have insisted that because there are no pain receptors within the intervertebral discs, discogenic pain cannot occur2). However, Groen et al.34) identified the sinu-vertebral nerve using a new staining technique, which ends in the posterior longitudinal ligament and the outer lamina of the annulus fibrosis11). Interestingly, discogenic back pain has relevance to a unique sensory pathway, unusual in the musculoskeletal system31,3252), which has a dual pattern of sensory pathway26). One route enters the adjacent dorsal root in segmentalized way, whereas the other supply is non-segmental ascending through the paravertebral sympathetic chain with re-entry through the thoracolumbar white rami communicants54,5676). In accordance with all these results, the presence of discogenic back pain is supported by both observed clinical data and neuroanatomical research.
The mechanism of discogenic pain is also explained by 'peripheral sensitization'32,75) and possibly 'central sensitization'32,58) as a potential cause of chronic back pain. In addition, the disc affected by DDD may also acquire innervation. Neovascularity and unmyelinated nerve endings proliferate along the degenerative annular fissures, and penetrate deep into the annulus, the outer nucleus, and the end plate cartilage18,2962). The intrinsic inflammatory mediators must sensitize these nerves, and the sensitized nerves may mediate lumbar discogenic back pain. In the light of the pathogenesis, LTDR must be an ideal surgical management, the pathologic disc totally replaced but its mobile function conserved.
Diagnosis
The clinical features of DDD are nonspecific and variable. Back pain is principal, mainly in midline and immediate paraspinous in the lumbar area. Sitting intolerance caused by backache is a major feature of this disease51). Pain usually is worsened with flexion and lessened with extension. Not a few patients suffer from difficulty recovering from standing flexion. Even if discogenic pain is predominantly axial, somatic referred pain to the lower extremities is common too, which appears widespread, ill defined, and described as an intolerable ache deep in the limb. This is different from radicular pain associated with disc herniation. Neurologic findings are usually normal. DDD is also associated with psychological distress7,61). Practically, discogenic back pain remains primarily a diagnosis of exclusion77).
Radiographic evaluation should be the initial study of choice but actually doesn't denote any specific images but the common findings of degenerative changes.
MR imaging must be the ideal modality for the evaluation of lower back pain (LBP). Characteristics of DDD on MRI are decrease in disc height, presence or absence of annular tears, signs of disc degeneration (e.g., decreased signal on T2WI : dark disc), and end-plate changes13). The high-intensity zone (HIZ) used to be recognized as a sign of annular tear and a specific indicator of a painful internal disc disruption51). However, recently its clinical significance has been questioned because of the continued low sensitivity with regard to pain reproduction48). Disc degeneration can occur in the absence of related symptoms including back pain. It has been reported10) that almost 30% of asymptomatic individuals with no history of LBP had disc abnormalities in MR imaging. And being followed up for seven-year, these patients demonstrated that MRI abnormalities were not predictive of the development or duration of LBP12). There is no pathoanatomic gold standard for discogenic pain, even tissue pathology of disc either51).
Given the concept of imaging that correlates with discogenic pain for recognition of a pathological dark disc, the current reference standard test for discogenic pain is provocation discography, although its effectiveness and reliability have come into question15). The main limitation of discography is that it relies only upon patient's subjective pain responses. Therefore, it is inevitable to carry out the same procedure of discography in a contiguous asymptomatic normal disc as a control during provocation discography. In asymptomatic discs, usually the pain is mild and requires high-pressure injection to elicit51). The addition of post-discography CT allows further characterization of the anatomic basis of DDD70,85). If the most reliable conditions for a successful provocation discography are summarized16), four findings can be considered : 1) low-pressure injection, 2) degenerative disc morphology including dye extravasation through the annulus, 3) subjective reproduction of the patient's pain at the injected (index) level, 4) no or minimal subjective pain at the adjacent (normal control) levels injected. There was a clinical try to apply the concept of dual sensory pathway to provocation discography for confirmative diagnosis in the author's institute, but this try had not borne a fruit.
Taking the knowledge and experience we have so far into consideration in concert, the provocation discography along with clinical features appears to be information most dependable for spine surgeons to consult for the diagnosis of DDD, even though there is no fully reliable diagnostic tool available.
Managements of DDD
There are a multitude of treatments used in clinical practice to treat chronic LBP, with little consensus amongst clinicians as to which the best approach is63). Treatments of symptomatic DDD can be largely divided into two major categories : non-surgical and surgical treatments. Non-surgical treatments include activity modification, physical therapy such as exercise to strengthen muscles, spinal manipulation and use of braces, and medication treatments. And they also include intradiscal electro-thermal therapy68) and various kinds of epidural procedures. Surgical treatments include fusion and motion-sparing surgeries.
The understanding of natural history of discogenic back pain can offer a clue for decision-making of treatments and predicting clinical outcome. Epidemiologically1) about 90% of persons with LBP improved to normal state within 3 months with or without proper treatment. Meantime, other investigators61) recently presented different results of their clinical study that the natural history of discogenic LBP was continuous and chronic. This result indicates that most patients are expected to experience LBP after a longer time interval, and their pain severity is expected to remain nearly the same. Based on these two study results, the initial treatment of all patients with LBP but patients with a neurologic emergency should be nonsurgical, however surgical treatments can be considered if back pain remains nearly the same or gets worse even following 3-month conservative treatments.
THE PAST AND PRESENT OF LTDR INCLUDING LONG-TERM OUTCOME
History
In 1960, Fernstr├Čm28) implanted an artificial disc for the first time, which was in the form of a steel ball using an anterior approach, the results of which appeared initially encouraging, but became disappointing in the long-term follow-up. The ball ended up subsiding into the subchondral bone. About 20 years later in 1984, Schellnack and Buttner-Janz in Germany implanted the SB Charite prosthesis using anterior approach83). The implant was a semi-constrained type of lumbar artificial disc (LAD) and comprised two metallic upper and lower plates and a sliding polyethylene core. Thereafter, three successive models of this implant have been launched and regularly used by David and Lemaire in France8,4971). In 1990, Marnay implanted ProDisc-L in France, which was a semi-constrained type and comprised two metallic plates and non-mobile polyethylene core6). An upgraded successive model, ProDisc-II was launched in 1999 and has been widely used in the market21,78). Since then, many different designs and composition of LAD have been launched, and multitudes of implants are available these days.
Designs and composition
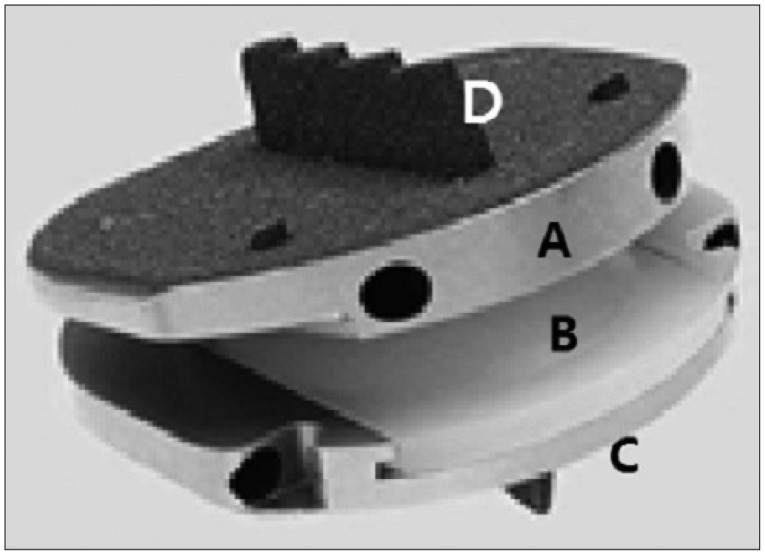
According to the direction of back motion limitation in mobility of LAD, it can be classified into 3 types5) : non-constrained, semi-constrained with translation and semi-constrained without translation. Non-constrained design has no specific limitation in its mobility [ex. Elastic Spine Pad (ESP)], semi-constrained design has two types, the one has no specific limitation including partial translation (ex. SB Charite, Mobidisc) (Fig. 1), the other no specific limitation but translation (ex. ProDisc-L, Maverick) (Fig. 2). More strong and perfect anchorage and stability are required in more constrained design of LTDR83), while in non-constrained designs the plates are highly mobile to protect them against the risks of mechanical stress but this design of LAD imposes greater stress on the posterior joints5).
LADs are made up with metal and alloys such as stainless steel, titanium and cobalt alloys, and high molecular weight polyethylene such as ultra-high molecular weight polyethylene (UHMWPE) for nucleus (core) (Fig. 2), and ceramics5). In LAD, bearing surfaces are designed to accommodate load without breaking, to reduce friction and wear and to conserve range of motion.
In addition, LADs can also be classified by anchorage, surface and friction couple, design, location of center of movement, and compatibility with MRI.
Selection criteria for LTDR
Since LTDR was applied in the management of degenerative lumbar spine diseases in early 1980s, many efforts have been made to set up criteria to avoid complications and to maximize surgical outcome by selecting right patients for LTDR. In respect that DDD is not seriously malignant but benign, LTDR appears to be rather aggressive means in the spectrum of management options, because back pain kills nobody but aggressive surgery can kill somebody. Therefore, in the selection of patients for LTDR, an absolute adherence to accepted indications and contraindications is a must. In the first USA Food and Drug Administration (FDA) Investigational Device Exemption (IDE) trial using Charite, the indications for LTDR were 18 to 60-year-old patients with single-level symptomatic DDD at L4-5 or L5-S1 without radiculopathy with visual analog scale score Ōēź40 and an Oswestry disability index (ODI) Ōēź30 in spite of more-than-6-month of participation in an active rehabilitation program, reproduction of concordant pain in provocative discography without relevant pain at one or more control levels9). Bertagnoli and Kumar3) have correlated the outcome of surgery in 108 patients with the indications, and then categorized the indications into 4 levels. Among them the indication, which correlated with the best outcome, was named "prime". The prime candidate for LTDR was presented as a patient with single level DDD, more than 4 mm of remaining disc height, no osteoarthritis in the facet joints, no degeneration at the adjacent level, and intact posterior elements3).
The contraindications for LTDR include conditions that may compromise the safety and integrity of the implants9). The patient should not have vertebral fractures, a spinal instability at the index level, particularly spondylolisthesis for any reason or of any grade, and any other spinal conditions, which necessitate a fusion surgery either. Patients with osteoporosis should not undergo LTDR, because the weakened bone can lead to the subsidence of the implant and fracture or splitting of vertebral body especially in keel type LADs. Another contraindication is lumbar spondylosis such as significant facet joint changes, too much narrow disc space (<5 mm), degenerative arthrodesis and stenosis. Among them, facet joint changes may be the most serious because this may compromise not only function of the motion segment including the implant but also surgical outcome due to postoperative persistence of the facet pain. Preoperative facet joint injection can be considered to rule out facet-origin pain in a questionable case. And the patient with a history of prior lumbar surgery that was extensive laminectomy more than simple laminotomy is also considered contraindicated. Finally, the contraindications also include history of severe foreign body reaction to implant, history of major intraperitoneal surgeries, and a case of pregnancy, or severe abdominal obesity. The contraindication must be considered more seriously for good surgical outcome of LTDR than the indications.
Surgical techniques
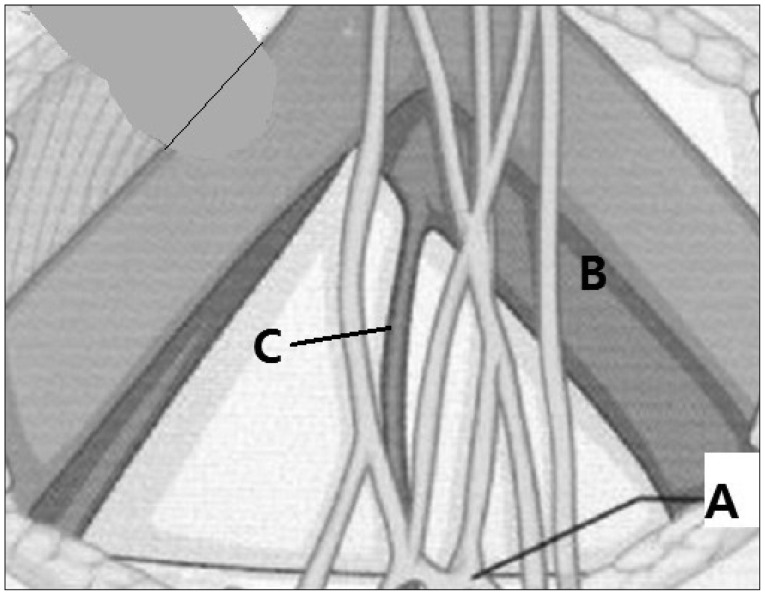
LTDR is usually done through anterior approach (Fig. 3). In anterior approach for LTDR, the left retroperitoneal approach is preferred in all levels but in L5-S1. The reason for the left side preference is to avoid an injury of the large vessels, especially the vena cava, which is located mostly at the right side of the lumbar spine. And the dissection and traction of this vessel are not easy. However, in a patient with L5-S1 lesion, especially in male, the right side approach is usually recommended because hypogastric plexus is usually located in the left anterior part of the promontory (Fig. 4), which may bring about retrograde ejaculation in male. So, a surgeon can push the plexus away of the main operation field to the contralateral side in order to avoid the damage of the plexus while exposing the anterior part of L5-S1 disc by the right side approach. Another benefit, when the patient with a history of L5-S1 LTDR undergoes second LTDR surgery at a level above, a surgeon can take the conventional approach, anterior and left retroperitoneal approach and dissect the vena cava without significant difficulty because the surgical wound in the left abdomen and retroperitoneal space remains still virgin.
Once exposure of the anterior part of intervertebral disc at the index level is obtained, the next important step is a correct placement of implant. The prosthesis must be placed into the middle of disc space on coronary plane, as far posterior as possible on sagittal plane, and as large foot-print as possible.
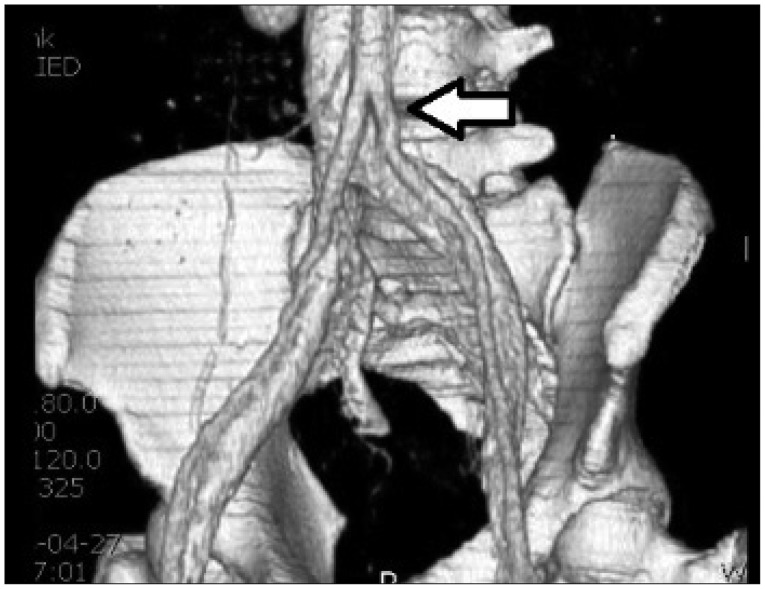
Lately, LTDR designed suitable for lateral or anterolateral approach to lumbar discs is introduced. LTDR for anterolateral approach, through an access between the psoas muscle and large vessels (Fig. 5) has a merit that it does not need to manipulate the abdominal major vessels (ex. Maverick-O), while it has been reported a practical difficulty in placing LAD correctly in a proper position, particularly at the midline in coronal plane and frequent postoperative subsidence of the implant50). Consequently, the merit of this newly designed implant appears to be offset by these shortcomings. LTDR for lateral approach (ex. Nuvasive's XL) has merits of no need for manipulating the abdominal major vessels, preservation of anterior longitudinal ligament, easy accessibility and various salvage options, while it has demerits such as high-risk of lumbosacral plexus injury and inaccessibility in a case of lumbosacral spine lesion especially with high iliac crest64).
Extended application of LTDR
LTDR technology has been applied in various ways and pathologies by some investigators. For instance, it have been reported that cases of multilevel DDD (>1 level) were treated with multilevel LTDR or hybrid LTDR, patients older than 60 years of age were treated with LTDR4) and cases with both DDD and severe facet arthropathy were treated only with a replacement technology, anteriorly LTDR and posteriorly facet replacement57). Most of the extended applications of LTDR are still in investigational stage. Among them, hybrid LTDR in multi-level DDD has been tried clinically and experimentally by many surgeons. Daftari et al.20) reported the results of a kinematic study that both one-level and a two-level LTDR and hybrid constructs did not significantly change adjacent kinematics compared to the intact level, while the two-level fusion construct presented an increase in flexibility at the adjacent level and two-level LTDR construct tended to decrease motion with a stability concern. These results were interpreted that hybrid constructs may be applied to two-level lumbar DDD as a replacement for two-level fusion surgery. Erkan et al.27) reported similar results that in an in vitro human cadaveric biomechanical study, the motion at L4-5 of a hybrid model, LTDR at L4-5 and fusion at L5-S1 is similar to that of a two-level LTDR. Meanwhile, a two-level fusion at L4-5, L5-S1 reduced intact motion. In conclusion, they suggested clinical studies to validate the efficacy of the hybrid model. Hybrid TDR appeared to be biomechanically feasible for a surgical alternative of two-level fusion. Recently, a prospective randomized clinical trial demonstrated that hybrid group had significantly lower mean visual analog scale (VAS) pain scores and better biomechanical outcome at mean follow-up of postoperative 37 months compared to 2-level circumferential fusion group39). Based on the results of these studies, hybrid LTDR, especially such a composition as LTDR at L4-5 and fusion at L5-S1 appears to be feasible biomechanically as well as clinically for the surgical management of multi-level DDD.
A cadaveric biomechanical study of multi-level LTDR has revealed that two-level LTDR maintained more favorable biomechanical environment at the adjacent segments compared with fusion surgery24). And a prospective longitudinal single group cohort study demonstrated that multi-segmental LTDR seemed to be safe and efficacious treatment method at 2-year follow-up for patients with deliberating lumbar spondylosis without significant facet arthropathy5). We need a prospective well-controlled randomized study to confirm therapeutic role of multi-segmental LTDR.
Outcome
Lemaire et al.46) reported the 51-month follow-up clinical result of SB Charite in 105 patients. Among them, 79% responded as very satisfied and 87% was able to perform normal labor works. Tropiano et al.78) assessed the outcome of 55 patients treated with ProDisc-L and followed up for average 8.7 year. In this study, 40 of them presented notable symptomatic improvement, 74% of success rate was achieved and no implant-related complication but approach-related complications such as injury of vein, retrograde ejaculation and hernia were observed78).
The author has reported follow-up clinical results of LTDR, ProDisc-L sequentially two times : Once more than 2-year and secondly more than 5-year59,60). In more than 2-year follow-up of 30 patients consecutively operated with ProDisc-L59), VAS and ODI reduced from 7.2 to 1.2 and from 18.3 to 4.1 respectively, and the mean motion range at the levels operated was 4.78┬░, while the one at L5-S1 was 2.9┬░. This finding indicated that the motion preservation rate at L5-S1 by LTDR appears to be low and not significant compared to the one at L4-5. In more than 5-year follow-up of the same cohort60), outcome scores such as VAS and ODI maintained in improved state at the last follow-up. 71.4% of them achieved overall success. However, the results of radiological follow-up to monitor maintenance of the implant appeared to be below expectations, because the mean global lumbar motion range has reduced from 37.94┬░ at 1-year, to 29.03┬░ at 2-year and then 17.01┬░ at more-than-5-year follow-up, much less than preoperative value, 24.3┬░. And the mean height of the disc space increased immediately after LTDR, since then it reduced progressively and constantly from 17.2 mm immediately after LTDR to 13.8 mm at the last follow-up. Posterior facet degeneration at the last follow-up was observed in 30.3% at the index and 14.1% at the adjacent level, meanwhile in the earlier study of the same cohort, more-than 2-year follow-up, observed in 29.3% at the index and 6.4% at adjacent. Consequently, facet degeneration did not appear to progress at the index level, while progressed two times at the adjacent levels, compared to the one in 2-year follow-up.
Gornet et al.33) reported several variables proved effective at optimizing LTDR outcome in patients treated with Maverick. These variables include a preoperative disc height <8 mm, Modic type 2 changes adjacent to the target disc, a low amount of lordosis at the treatment level, low levels of fatty replacement of the paraspinal musculature, a prominent amount of facet joint or disc degeneration, and the presence of flat or convex vertebral endplates. They also reported that post-operative findings associated with better patient outcomes included a larger per cent of the endplate covered with the implant, greater increases in disc space heights, larger implant heights, and a larger increase in index level lumbar lordosis.
Currently, relatively long-term follow up results of prospective random controlled multicenter comparison studies between LTDR and fusion groups have been reported. These studies had been carried out in the USA as US FDA IDE studies since 1980s. Guyer et al.36) published the results of 5-year follow-up prospective, randomized, multicenter study on the Charite disc in 2009, which should be the first published study up to that time among the similar kinds of studies on the Charite and other types of LADs. In this randomized study on Charite as the treatment group and anterior lumbar interbody fusion (ALIF) with BAK cage as the control group for the treatment of single-level DDD, the clinical outcomes were similar across groups, although overall success rate (Charite vs. BAK group : 57.8% vs. 51.2%, p<0.05), patient full-time employed rate (65.6% vs. 46.5%, p<0.05) and long-term disability (8.0% vs. 20.9%, p<0.05) presented significant difference. In this five-year follow-up study, they concluded the consistency of Charite's non-inferiority formerly presented in the two-year reports compared to ALIF with BAK. In 2012, Zigler and Delamarter86) published the results of 5-year follow-up prospective, randomized, multicenter study on the ProDisc-L in patients with single-level DDD. In this study, patients in both, LTDR and circumferential lumbar fusion groups maintained significant improvement during the 5-year follow-up and did not have any significant difference in the clinical outcomes between the groups. The results of these two studies herald that therapeutic effects of LTDR in patients with DDD are not superior but equivalent to those of fusion. Accordingly, LTDR could be considered as one of surgical options in a selected patient group. However, these studies were criticized for the limitations of industry-sponsor clinical researches. Especially the Charite study was bitterly depreciated due to its inappropriate control group of the BAK device, which did not represent the best of modern spinal fusion techniques but was known largely abandoned. And also due to loss of many participating centers to follow-up after 2-year study closed, which is known to be jeopardizing validity and generalizability, there is a clear risk of having a poorer experience with one study arm at those centers35).
In the meantime, some single group cohort studies including those of the author have demonstrated that in more than 5-year long-term follow-up, for carefully selected patients, clinical results of LTDR are compatible with those of fusion, which have previously been published for a variety of different fusion techniques and maintaining the improved state throughout59,7278). In these articles, the authors concluded LTDR can be a viable treatment alternative to have benefit of LTDR in some relevant patients such as a single level lumbar discopathy in young age72,78).
However, in most of review articles dealing with LTDR, limitations of industry-sponsored research are pointed out in US IDE clinical trials of prospective multicenter randomized controlled study, and lack of high quality of evidence sufficient enough to justify the wide-spread use of LTDR is also generally pointed out19,4279,83). Consequently, higher quality of prospective controlled and longer-term follow-up studies with relevant control groups are still required to establish efficiency and longevity of the devices, LADs and to support an assumption that a fusion surgery can be replaced with LTDR in the surgical treatment of DDD.
THE STRENGTH AND SHORTCOMING OF LTDR
Strength
Merits of LTDR can be divided into three groups according to the evidence of certainty. The first group is the inherent advantages which can be obtained simply because LTDR is a non-fusion surgery and can naturally avoid fusion-related complications including side-effects during harvesting donor bone, in donor site such as dislodgement, subsidence and mal- or non-union, and also slow virus infection by allograft fusion. No one questions about these substantial merits of non-fusion surgery. Eventually, this group does not need to prove evidence.
Second group is the advantages, which can be expected because the device was designed in a motion preservation technology. A representative example of this advantage is preservation of motion at index level, which has been confirmed in long-term follow up studies6,3559,6079,8386). The primary design objective of LAD is to restore normal motion. However, when the newly formed motion obtained by LTDR is non-physiologic, grave doubt exists as to whether this motion at the index level is still beneficial to the spine, especially to the structures like facet joints at the index and adjacent levels67). This question is still left unaccounted for59,66).
The third group is what surgeons anticipate when a certain new and innovative technology is applied to clinical practice in surgical treatment of a specific pathology, and strongly requires evidence. The most typical example of the third group is application of LTDR in anticipation of minimizing the development of adjacent segment disease (ASD). However, the eligibility of LTDR for this advantage is still on debate38,69). According to recent review articles dealing with ASD, the etiology of ASD has been known multifactorial in nature : 1) natural history of the adjacent disc, 2) biomechanical stress on the adjacent level caused by the fusion, and 3) anatomical disruption at the adjacent level in the initial surgery38). Which factor the major contributor is in the development of ASD among them remains undetermined. Wai et al.84) assessed MRI for over 20 years in patients with normal preoperative discograms and operated with anterior lumbar interbody fusion (ALIF), in which only 6% of patients required surgery at the adjacent level although the incidence of degeneration was similar between adjacent and other nonadjacent levels (23.1% vs. 17.9%). They concluded that the natural history of the disc was likely related to ASD rather than the altered biomechanics at the adjacent level. The biomechanical changes at the adjacent level following fusion surgery have been well documented, which include an increased range of motion and increased intra-discal pressure23). However it is hard to demonstrate the causal relationship between biomechanical changes and degeneration25). If we can observe a case with postoperative sagittal imbalance after LTDR, this alteration of sagittal alignment can be an example because patients with postoperative loss of lordosis are known to have a significant increase in asymptomatic adjacent segment degeneration (ASDegen)47,7387). Disruption of the posterior elements during fusion procedure also aggravates the degenerative process at the adjacent level by changing the normal anatomy. Min et al.53) recently demonstrated the difference between anterior interbody fusion and posterior interbody fusion for lumbar spondylolisthesis in the incidence of ASDegen to be 44% with ALIF and 82.6% with PLIF. Surgeons should appreciate the importance of maintaining the facets intact at the adjacent level during fusion surgery in the lumbar spine.
The incidence of ASDegen in the lumbar spine ranges widely. Such a wide range may be ascribed to the various kinds of surgical procedures for the lumbar spine pathology41). Avoidance strategies can be considered on the basis of three etiological factors mentioned above. Altering the natural history is beyond current clinical technology. However, it can be expected to have an ability to alter the destiny of the adjacent level attributed to biomechanical and anatomical changes at the time of the index level procedures. Actually, several implants have been introduced on the market to avoid ASDegen. They include LTDR, dynamic fixation, and percutaneous fixation in the lumbar spine. LTDR and dynamic fixation were designed in the concept of motion preservation technology, and expected to reduce biomechanical stress caused by fusion surgery on the adjacent segments. Meanwhile, percutaneous fixation can preserve the adjacent level posterior elements during posterior fixation with transpediclular screws by avoiding anatomical disruption at a facet of the adjacent level.
Whether LTDR has an ability to avoid ASD or not remains undetermined38). Recently, Zigler et al.87) published the 5-year results for radiological ASDegen changes from a prospective multicenter study. In the study, patients were randomized to either LTDR or circumferential fusion for single-level lumbar DDD. In the results, new findings of ASDegen were observed in 6.7% of LTDR patients and 23.8% of fusion patients (p=0.008). Secondary surgery at the adjacent level was reported for 1.9% of LTDR patients and 4.0% of fusion patients (p>0.05). The author concluded that there was a significant sparing effect on radiological ASDegen in patients with LTDR compared with that in the control. These results can be analogized that LTDR does not have a significant avoiding effect on symptomatic degeneration at the adjacent level, but only has a sparing effect on radiological degeneration in 5-year follow-up. As a result, impact of LTDR on ASD cannot be conclusively stated and needs longer-term follow-up data.
Shortcoming
Most of shortcomings occur with various complications. The complication rates following LTDR ranged widely from 1% to 91.0%. The majority of the studies reported complication rates ranging from 10% to 40%79). In randomized controlled trials performed in USA, the overall complication and reoperation rates in LTDR group ranged from 7.3% to 29.1% and from 3.7% to 11.4%, respectively. But it was known that much higher rates were reported in FDA reports79).
Shortcoming can be divided into two groups according to either general complication or inherent complication. General complications consist of early and late. And they are related with non-specific common potential risks and complications encountered with during surgical approach and procedures regardless of the type of LTDR, which include wound problems, large vessels injuries, infection, retrograde ejaculation, nerve injury, and hematoma in the early stage and postsurgical incision hernia in the late stage.
Inherent weak point and complication are unique and LAD-originated, and also consist of early and late. Early one includes malposition and subluxation of implant, displacement of core or polyethylene inlay, same segment degeneration (SSD), ASDgen and unresolved preoperative back pain. Late one includes wear-debris induced osteolysis, osteophyte regrowth, ASD, and device failures such as implant migration, core or inlay migration, subsidence of the implant. Among them, disappointing one would be the occurrence of ASD following LTDR as a late complication, in respect that the primary justification for LTDR is to prevent or minimize the development of ASD. On the other hand, ASDegen, asymptomatic radiological degeneration appears to be negatively influenced by LTDR, apparently lower occurrence rate compared to fusion. Secondly SSD would occur under the condition of non-physiological motion of LAD67). In this regard, we need a biomechanical replica of human lumbar disc to develop a proper LAD.
LTDR is still supposed to be an unaccustomed technology, and it may potentially give rise to unfamiliar modes of failure, which spine surgeons have never experienced. Very late complications such as implant failure and wear-debris osteolysis are well known in large joint arthroplasty, which must be the most serious shortcoming. In fact, at the early period of LTDR use, release of wear debris would not be a clinically relevant issue to physicians. However, currently wear-debris induced osteolysis has been reported in patients treated with Charite45), which is practically the firstly commercialized LAD at the market and was followed eventually for the longest time among LADs available17,44). A similar nature of complication has been also reported in two patients implanted with ProDisc-L80), different design and composition from the former one, Charite. Veruva et al.82) investigated if the design and biomaterial factors affect clinical wear performance of TDR by reviewing relevant literatures. In this study, they found wear-associated complications could occur according to biomaterial selection for LTDR. For instance, 'metal-on-polyethylene' type LAD produced polymeric wear debris, while 'metal-on-metal' type has a tendency of generating small metallic wear debris and metal ion leading to adverse local tissue reaction5,37). LTDR designs incorporate polyethylene core, UHMWPE. Meantime, Veruva et al.81) also recently reported that ╬ō-inert-sterilized UHMWPE has notably improved the wear resistance of LTDRs compared with historical UHMWPE. And they presented that there was no significant influence of design factors (mobile- vs. fixed-bearing) on wear particle characteristics. Mobile-bearing type is identical with semi-constrain with translation (ex. Charite) and mobile-fixed type is semi-constrain without translation (ex. ProDisc-L). Therefore, an appropriate follow-up interval for LTDR may extend the time frame applied to patients treated with more traditional spine procedures. This is another reason for the necessity of long-term follow-up in LTDR.
Additionally, pitfalls related with anterior retroperitoneal approach for LTDR surgery can be considered including lack of salvage strategy and difficulty in access to anterior mid-part of the lumbar spine14). These pitfalls are mostly in conjunction with failed manipulation and inexperience of the large vessels, particularly the inferior vena cava during approaching the anterior part of the lumbar spines. And these approach-related shortcomings may be one of the serious reasons LTDR has been currently disregarded by many ordinary spine surgeons.
FUTURE PERSPECTIVES OF LTDR
If the most ideal LAD is installed, following conditions must be coincided : A removal of the offending lesion and bringing a recovery from intractable pain, while sparing the physiological motion, stabilizing the lumbar spine in good curvature and maintaining an ideal sagittal balance without fusion or sacrifice of not relevant structures. We need a detailed characterization of the range of motion of the lumbar spine, which must be indispensable in the development of a next-generation LAD because restoration of normal motion is the most important goal of LTDR19), and sparing the physiological motion may be the most desirable condition provided by LAD. The implant has continued advancement in materials and designs, which will consequently lead to a development of innovative design of LAD and/or improvement in device performance as well as surgical outcome.
CONCLUSION
In review of the literatures regarding the clinical significance of LTDR in the management of patients with DDD in the lumbar spine, it can be realized that the clinical value of LTDR still remains unsettled and the selection criteria for LTDR must be restrictive. LAD is a mechanical device that resides in patient's back and is generally safe, but does not come with lifetime guarantees. Consequently, longer follow-up should still be necessary to confirm the maintenance of improved surgical outcome and to observe any very late complications including wear-debris osteolysis and ASD, some of which spine surgeons may have never experienced. Fusion of the pathologic level must be still the mainstay of surgical management in DDD. Taking all information we have into consideration, as long as an evidence for LTDR's preventive effect against ASD in long-term follow up, and new versions of LAD designed to avoid various critical shortcomings can be provided, LTDR still may get a chance to establish itself as a substitute of fusion in the surgical treatment of DDD both nominally and virtually.