INTRODUCTION
Endovascular treatment of intracranial aneurysms using coils has become an accepted alternative to aneurysm neck clipping [3,4,8]. Technological advancements have led to increased coil stability, improved microwire stability and flexibility, and development of smaller microcatheters, which have rendered the process safer and simpler. However, incomplete occlusion or coil protrusion can occur during endovascular coiling, especially in patients with wide-neck or complex aneurysms. Stent-assisted coil embolization is being commonly used to counter such problems in the treatment of wide-neck aneurysms.
In the past 20 years, several newer laser-cut or braded stents have been introduced, such as the Solitaire, NeuroForm EZ, Enterprise, LEO and LEO Baby, LVIS and LVIS Jr. stent. Each stent has its own advantages and disadvantages. The open-cell type stents have the advantage of a better apposition of the vessel wall compared to that with the closed-cell type stents, but re-sheathing is impossible, and coil prolapse is more frequent in patients with open-cell stents [7]. Braded stents have increased metal coverage and can expect the flow diversion effects; however, considerable effort is required for the proper deployment [5]. NeuroForm Atlas (Stryker Neurovascular, Fremont, CA, USA) microstent is a next generation stent that has been improved to ensure lower profile delivery (via 0.0165 inch inner diameter microcatheter), better scaffolding due to small cell sizes, improved trackability, and higher conformability to the vessel wall compared to that with the previous stents. However, not many reports of this NeuroForm Atlas stent have aimed to evaluate the safety and efficacy of the NeuroForm Atlas during stent-assisted coil embolization of intracranial aneurysms.
MATERIALS AND METHODS
Patient population
We retrospectively analyzed electronic medical records and picture archiving and communication system data from 31 consecutive patients with intracranial aneurysms treated at our institution using the NeuroForm Atlas (Stryker Neurovascular) stent-assisted coil embolizaiton (SAC) between February 2018 and July 2018. Patients with both ruptured and unruptured aneurysms were included. This study was approved by Institutional Review Board of Pusan National University Yangsan Hospital (IRB No. 05-2019-090).
In addition to aneurysm-related information (location, size, prior treatment, and dome-neck ratio), we collected detailed procedural information regarding the techniques used (i.e., jailing or trans-strut technique), angiographic outcomes (Raymond-Roy occlusion classification, RROC), and periprocedural complications. Follow-up clinical and angiographic data were also obtained. In-stent stenosis was defined as narrowing of the vessel by more than 10%. Angiographic results were independently adjudicated by two neurovascular specialists.
Endovascular procedural information
Patients with unruptured aneurysms were pre-medicated using dual antiplatelet medication (acetylsalicylic acid 100 mg daily and clopidogrel 75 mg daily) for at least 7 days. P2Y12 reaction units were analyzed using the Verify Now assay prior to the procedure, and patients with values greater than 240 were regarded as clopidogrel non-responders. In such patients, cilostazol was administered immediately before the procedure, and clopidogrel was replaced with cilostazol after the procedure. During the procedure, 3000 IU of heparin was administered (depending on the patientŌĆÖs bodyweight, 50 IU/kg). If the procedural time exceeded 1 hour, additional 1000 IU of heparin were administered per hour.
The preoperative dual antiplatelet medication was not indicated in ruptured cases. Therefore, glycoprotein IIb/IIIa inhibitor tirofiban (Aggrastat, Merck &Co, Kenilworth, NJ, USA) was administered intravenously after stent deployment. All such patients received maintenance infusions of tirofiban (0.1 ┬Ąg/kg/min intravenously for 24 hours) [13].
All procedures were performed under general anesthesia and via femoral artery access with systemic heparinization. The flush system contained 5000 IU of heparin per liter.
Measurement of Clinical and angiographic outcome
Clinical outcomes were evaluated by the neurosurgeon using the modified Rankin scale (mRS). According to the mRS, favorable and unfavorable outcomes were 0-2 and 3-6, respectively. In patients with ruptured aneurysms, the HuntHess grades, FisherŌĆÖs grades, Glasgow coma scale scores, and the mRS scores were recorded at initial evaluation, while changes in mRS scores were recorded at discharge and during outpatient follow-up.
Digital subtraction angiography (DSA) was performed at the 6-month follow-up appointment. Occlusion of the aneurysm was evaluated based on the guidelines of the RROC (class I : complete obliteration, class II : residual neck, class III : residual sac). Recanalization was defined as a change from RROC class I/II to class III between the immediate postoperative period and the end of follow-up. All changes, including coil configuration, flow patency of the parent artery, and intimal hyperplasia, were recorded.
Safety and efficacy
Occurrence of major ipsilateral stroke or neurological death between the immediate postoperative period and 6 months following the procedure was considered as the primary endpoint. We compared our safety data with long-term morbidity and mortality data derived from previous studies evaluating stent-assisted coil embolization. All procedural events relating to the device, including coil loop protrusion, thromboembolic events, re-bleeding, or changes in technique, were recorded and evaluated. Angiographic results (RROC classes I and II) at the 6-month follow-up appointment and rate of aneurysm occlusion (complete occlusion) were regarded as the primary efficacy endpoints.
RESULTS
Characteristics of patients and aneurysms
Thirty-one consecutive patients with 35 aneurysms underwent 33 stent-assisted coil embolization procedures using NeuroForm Atlas between February 2018 and July 2018. In two patients, aneurysms were located close to one another, allowing simultaneous treatment using a single stent-assisted embolization. In one patient, two aneurysms were located far from one another, necessitating two separate stent-assisted embolization procedures. In one patient, two stents were used for one aneurysm. All patients were included in the analysis. Among the 31 treated patients, 11 (35.5%) were treated for ruptured aneurysms, while 21 were treated for unruptured aneurysms, including one patient who underwent retreatment. The mean patient age was 60.6┬▒13.3 years (range, 22- 83), and 24 patients (77.4%) were females. The baseline patient characteristics are presented in Table 1 and Table 2.
All 35 aneurysms were of the saccular type : six (17.1%) were located in the posterior circulation (basilar artery, five; superior cerebellar artery, one), while 29 (82.9%) were located in the anterior circulation (anterior cerebral artery, nine; middle cerebral artery, one; internal carotid artery, 19). The mean aneurysm size was 5.2┬▒2.6 mm (range, 2.0- 11.8). Of the 35 aneurysms, 34 (97.1%) were wide-neck aneurysms, defined as aneurysms showing dome-neck ratio (D/N ratio) Ōēż2 or neck size Ōēź4 mm. The mean neck size was 3.5┬▒1.0 mm (range, 1.5-5.2).
Procedural information and angiographic outcomes
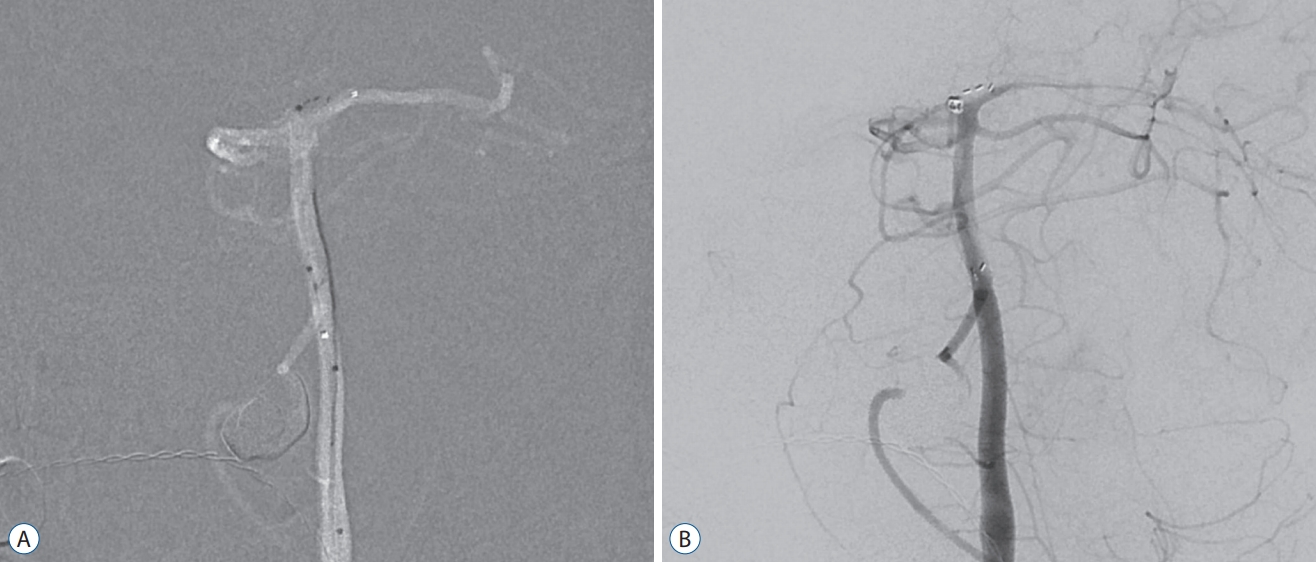
In all the patients and for all the aneurysms, the NeuroForm Atlas reached the target vessel and was successfully deployed at the neck of the aneurysm. All the stents were deployed as per preoperative planning in all the 22 unruptured cases. All coiling procedures were performed using a jailing technique; although, a trans-strut technique was used for additional coiling in three cases without complications. In 21/22 (95.4%) cases, the stent was deployed at the appropriate site. However, in one case, stent was deployed at an unexpected location because the microcatheter moved during opening for stent deployment (Fig. 1). Immediate, complete occlusion was evident in 16 of 24 aneurysms (66.7%), while neck remnants persisted in six patients (25%). Residual aneurysms were evident in two patients (8.3%).
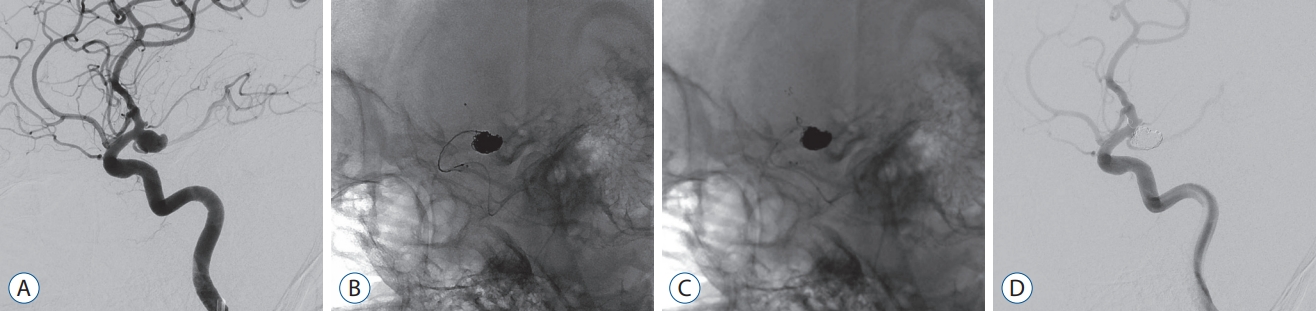
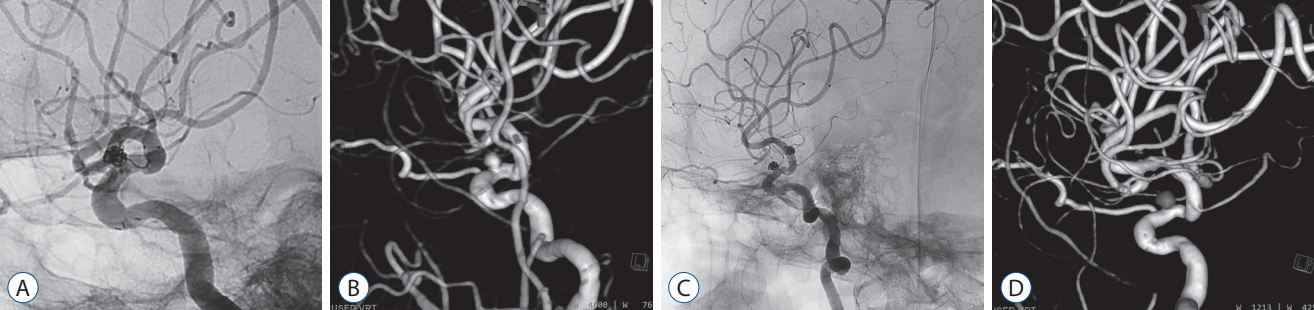
Among 11 patients with ruptured aneurysms, five underwent planned stent-assisted embolization. In six patients, stents were used to overcome unexpected events including thromboembolic complications (Fig. 2), final coil protrusion (Fig. 3) and coil instability (Fig. 4), and thromboembolic complications. Immediate angiographic revealed that complete occlusion occurred in eight patients (RROC I), while residual neck remnants were observed in the three patients (18.1%).
In one case (3.3%, case No. 30), intraarterial thrombolysis was required to address an immediate in-stent thrombus, which occurred during the procedure and was resolved without any associated complications.
Clinical outcomes
Patients with unruptured aneurysms showed no neurologic deficits prior to the procedure and were discharged without any clinical complications related to the procedure. Among the 11 patients with ruptured aneurysms, two died within a week after the procedure. One patient died due to hypoxic brain damage associated with re-bleeding just prior to the procedure, while the other died due to diabetic ketoacidosis caused by uncontrolled glucose levels. At discharge, four of nine patients exhibited unfavorable outcomes related to subarachnoid hemorrhage (SAH) (mRS=4 in three patients, mRS=3 in one patient). All four patients experienced acute hydrocephalus with intraventricular hemorrhage and underwent extra-ventricular drainage as initial treatment. Two of these patients underwent ventriculoperitoneal shunt surgery. Fortunately, there were no instances of vasospasm, ipsilateral stroke, late thromboembolic events, or late hydrocephalus in other patients with ruptured aneurysms. Overall mortality and morbidity rates in our study were 6.5% (2/31) and 12.9% (3/31), respectively.
Angiographic and clinical outcomes at 6 months
Follow-up DSA results were available for 21 patients with unruptured aneurysms. Follow-up DSA was not performed in one patient due to pregnancy. Among the 23 aneurysms analyzed, complete obliteration was observed in 16 cases (69.5%), while neck remnants were observed in six cases (26.1%). One patient (4.3%) had a residual aneurysm. Six patients with ruptured aneurysms underwent follow-up DSA at 6 months, excluding two patients that had died and three with unfavorable outcomes. Complete aneurysm obliteration was observed in three patients (50%), while two patients (33.3%) showed neck remnants. A residual aneurysm and growth of the aneurysmal sac were observed in one patient (16.7%). Therefore, among the 29 aneurysms for which follow-up data were obtained, complete aneurysm obliteration was achieved in 65.5% (19/29), while 27.6% (8/29) showed neck remnants, and 6.9% (2/29) revealed residual aneurysms.
Patients with unruptured aneurysms exhibited no neurological symptoms at follow-up. Five of nine patients with ruptured aneurysms recovered without neurologic symptoms. Three patients with mRS scores of 4 were admitted to the hospital, while one patient with an mRS score of 3 was admitted to a rehabilitation facility. Thus, favorable outcomes were achieved in 86.2% of patients (25/29) (mRS score <2).
DISCUSSION
In our study, we evaluated the safety and efficacy of the new NeuroForm Atlas microstent device used during coil embolization of wide-neck aneurysms. In our study, all stents were deployed successfully, and all aneurysms underwent coil embolization without technical problems. Several features of the NeuroForm Atlas stent help in successful deployment. The stent can be delivered via a 0.0165 inch or 0.017 inch microcatheter, the size used for coil delivery. This makes obtaining access to the distal aneurysms with small parent arteries easier. In addition, The NeuroForm Atlas stent has a unique structure that utilizes a closed cell for re-crossing of the microcatheter and an open cell for better anchorage and wall apposition [6]. These changes were introduced to improve stent deliverability, vessel wall apposition, and coil scaffolding and to overcome the foreshortening problems associated with the NeuroForm EZ system. Furthermore, smaller and increased numbers of alternative open cells provide better scaffolding and allow adequate coil stability at the bifurcated aneurysm or highly tortuous parent arteries. In addition, when compared to the braded stent, the low metal-to-artery ratio (6-12%) and segmental expansion ability of the stent system result in highly successful stent deployment without changing the parent artery direction. In addition, the rate of foreshortening of the NeuroForm Atlas stent is very low (2.9-6.3%), enabling very high deployment accuracy. Due to these advantages, successful deployments are similar to or better than those reported with the use of other stent systems such as the LVIS Jr. microstent, with which Behme et al. reported a success rate of 100%, or the LEO Baby stent, with which Aydin et al. reported a success rate of 93.5% [1,2].
In our study, no cases of stent-related ipsilateral stroke or neurological death occurred at the 6-month follow-up, resulting in a relative safety of 100%. Moreover, favorable outcomes were observed in 86.2% patients (25/29). This result is in accordance with those of Ten Brinck et al. [10], who reported favorable outcomes in 84.6% patients (22/26) treated using the NeuroForm Atlas stent in a preliminary study. Although only two patients with SAH (2/27) were included, Ulfert et al. [11] reported that none of their patients developed new symptoms or experienced permanent reductions in mRS scores. Another study by Jankowitz et al. [6] reporting the safety of NeuroForm Atlas system documented a stent-associated late thromboembolic event in one of the 30 patients with unruptured aneurysms (3.3%) at the 12-month follow-up. Taken together, these results suggest that the NeuroForm Atlas microstent exhibits comparable safety to the LVIS Jr. system [2].
In our study, immediate favorable outcomes and complete occlusion were observed in 94.2% (33/35) and 68.5% (24/35) of cases, respectively. At the 6-month follow-up, successful occlusion was observed in 93.1% (27/29), and complete occlusion was observed in 65.5% (16/29) of cases. Ten Brinck et al. [10] reported favorable and complete occlusion rates of 69.2% and 53.8% at 6 months, respectively. In addition, Ulfert et al. [11] reported satisfactory immediate angiographic outcomes: complete aneurysm obliteration was observed in 84% cases, while neck remnants were observed in the remaining 16%. Furthermore, high-resolution time-of-flight magnetic resonance angiography revealed an occlusion rate of 100% at the 5-month follow-up [11]. Jankowitz et al. [6] reported a complete occlusion rate of 86.7% for the NeuroForm Atlas system. Follow-up occlusion rates for stent-assisted coil embolization using the LEO Baby or the LVIS Jr. systems range from 56.5% to 90.0%, with one meta-analysis reporting a complete aneurysm obliteration rate of 60.6% [1,9,12]. Our findings are in accordance with the results of these previous studies, highlighting the efficacy of the NeuroForm Atlas microstent.
Despite the structural advantages, the NeuroForm Atlas stents also have some drawbacks in use. When deploying the stent at a concave surface, it is difficult to re-access the aneurysmal sac due to the tightness of the open cells. In contrast to the woven-design stent, NeuroForm Atlas stent system cannot ensure flow diversion. In addition, the NeuroForm Atlas stent cannot be re-sheathed. Indeed, currently no method exists for dealing with stents that have been deployed at an inappropriate position, and excessive attempts at removal can affect coil stability and damage the intima of the parent artery.
In the present study, case No. 20 was rather difficult, as the NeuroForm Atlas stent could not be re-sheathed. When the microstent is advanced through a relatively tortuous segment in the microcatheter, the microcatheter has a tendency for spontaneous withdrawal. To address this issue, a closed-cell stent can be re-introduced into the sheath, allowing for repositioning of the microcatheter and redeployment of the stent. However, as re-sheathing of open-cell stents such as the NeuroForm Atlas is not possible, surgeons must be aware of microcatheter tension and should carefully withdraw the microcatheter when the parent artery is tortuous. If the microcatheter is withdrawn before the distal tip of the stent exits the microcatheter, the transcatheter technique can be used. In this situation, the microcatheter containing the stent can be removed, and a new microcatheter can be securely positioned in the parent artery. This method may aid in reducing the risk of microcatheter drop and stent deployment at an undesired location.
The present study possesses some limitations of note, including its single-center retrospective design and short-term follow-up period. As our non-randomized study included only 31 consecutive patients, our results may have been influenced by selection bias. Furthermore, we did not include a control group of patients undergoing alternative endovascular treatments or patients with giant aneurysms. Indeed, only three patients had aneurysms larger than 10 mm, while seven patients had aneurysms smaller than 3 mm. However, our study is advantageous in that we utilized DSA at follow-up assessments.
CONCLUSION
In this study, we observed that stent-assisted coil embolization with NeuroForm Atlas stent may be safe and effective in the treatment of wide-neck intracranial aneurysms. Furthermore, NeuroForm Atlas stent-assisted coil embolization is feasible for the treatment of both ruptured and unruptured wide-neck aneurysms. However, long-term angiographic follow-up is required to completely elucidate the durability of the NeuroForm Atlas stent, as well as the associated recurrence and retreatment rates.