NTRODUCTION
Fever above 38℃ (100.4°F) is common in the first few days after major surgery [7,8]. Although fever may be caused by infection of the surgical site, most early postoperative fever is caused by surgery-induced inflammation and resolves spontaneously [9,12,19]. Moreover, the likelihood of early postoperative fever tends to be greater in patients who have undergone longer and more extensive surgical procedures [5].
We often encounter cases in which patients show postoperative fever unrelated to wound infection after spinal surgery. Postoperative fever may appear for a variety of reasons. Prolonged operation time and seroma due to a relatively more extensive surgery are risk factors for non-pathologic fever following general spinal surgery [23]. In the clinical field, it is helpful to investigate the incidence and risk factors for delayed postoperative fever as a basis for reducing the cost burden to rule out surgical site infection and to determine the cause of fever. Thus, we retrospectively analyzed postoperative fever in a selective and homogeneous patient population consisting of patients who underwent posterior cervical fusion using cervical pedicle screws (CPS), with or without a subsequent anterior approach [4,17,18,21].
MATERIALS AND METHODS
The study was approved by the Institutional Review Board of Gangneung Asan Hospital (GNAH 2018-02-001), with the consent process waived owing to the retrospective nature of the study. From March 2012 to December 2017, 119 patients at our institution underwent posterior cervical spinal surgery under general anesthesia. All operations were performed by a single surgeon, who performed all steps from skin incision to closure in all the operations. The minimum patient follow-up period was 6 months. Patients underwent decompression with laminectomy or laminoplasty and fusion using CPS placement. All CPSs were inserted using the freehand technique via a process that followed the safety steps, including repeat balltip probing and checking the feedback of the screw trajectory. If ball-tip probing suggested a pedicle breach, the CPS was converted to a lateral mass screw [18,21].
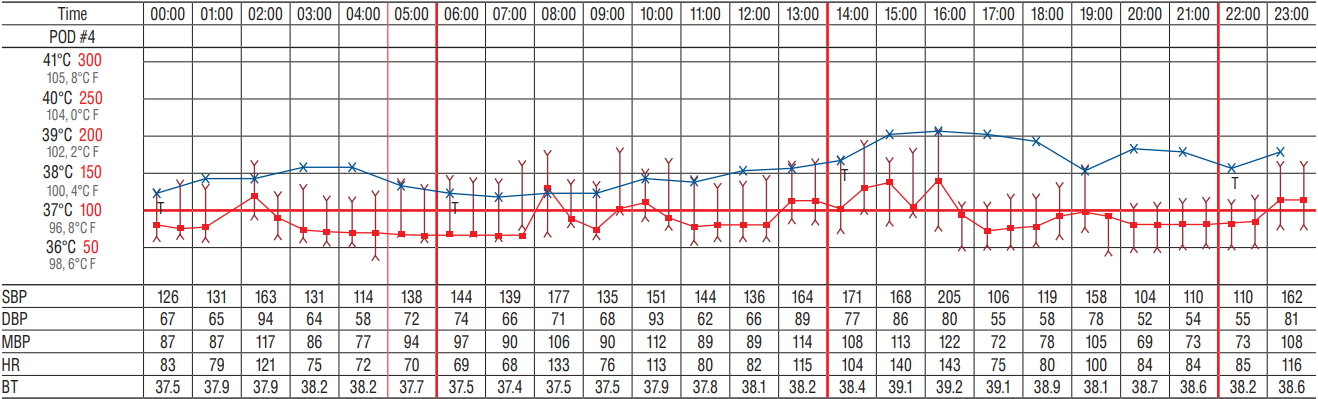
Patients underwent surgery for degenerative diseases, trauma, and tumor. Delayed fever was defined as no fever until postoperative day 3, followed by an ear temperature ≥38.0℃ on day 4 and on subsequent days. Body temperature was measured at least once every 8 hours. In patients who developed fever, body temperature was measured at least twice every hour. Patients were not considered febrile if they developed fever immediately after surgery to postoperative day 3, because the cause of fever during that period was surgery-induced trauma (Fig. 1).
To only evaluate patients with non-pathologic fever, patients with infectious conditions were excluded, including patients with wound dehiscence, spondylitis, and postoperative pneumonia. Patients with multiple traumas who required joint surgery in addition to spinal surgery were excluded, as were patients with a surgical level extending beyond the cervical spine.
Patients who underwent surgery from March 2012 to February 2014 were administered cefazolin 1 g twice daily as a prophylactic antibiotic until postoperative day 3. However, patients who underwent surgery from March 2014 to December 2017 were administered prophylactic cefazolin 1 g twice daily until postoperative day 1. No patient received additional antibiotics unless the cause of postoperative fever could not be identified. The origin of fever was always discussed with the patient’s medical specialist to exclude infectious causes, thereby excluding patients with drug-related or post-transfusion fever. Surgical site drains were left in all the patients and were removed only when the amount of drained fluid was <100 mL per day, or <30 mL every 8 hours.
Patients’ medical charts were reviewed. Data collected included patient age, sex, presence of diabetes mellitus or hypertension, smoking history, body mass index, diagnosis, surgical level, laminectomy or preservation of the lamina, performance of revision surgery, operating time, period of treatment with prophylactic antibiotics, and the performance of transfusion during the perioperative period.
Tests for statistical significance included Student’s t-test, Mann-Whitney U test, chi-squared test, and univariate and multivariate logistic regression. A p value <0.05 was defined as statistically significant.
RESULTS
Demographics of included patients
Overall, 94 males (84%) and 18 females (16%) were enrolled. The mean age was 58.4 years. Among the total number of patients, 108 (96.4%) underwent a posterior only approach surgery and four (3.6%) underwent a combined additional anterior approach surgery. Surgeries included 39 (34.8%) one-level surgeries, 31 (27.7%) two-level surgeries and 42 (37.5%) three or more level surgeries. A total of three revisional surgeries were performed, all on patients included in the no fever group. The above patients’ demographics were not significantly different between the two groups.
Prevalence of postoperative fever and infection
Of the 112 patients who met the inclusion criteria, 28 (25%) were febrile and 84 (75%) afebrile. The culture results for patients with fever were all negative, and none of these patients developed infection of the surgical site for 6 months after surgery.
Risk factors for postoperative fever
The incidence of laminectomy and trauma or tumor as the underlying medical disease differed significantly in febrile and afebrile patients. The five patients with tumors included one case of schwannoma and four cases of cancer metastasis. There was no significant difference in fever incidence with or without malignancy in tumor patients (Table 1). Of the 112 patients, 59 (52.7%) underwent laminectomy and 53 (47.3%) did not. Multivariate logistic regression analysis showed that laminectomy (odds ratio [OR], 10.251; p=0.000) was a statistically significant risk factor for postoperative non-pathological fever. However, tumor surgery (OR, 2.089; p=0.543 compared with degenerative disease or trauma surgery) and underlying medical disease (OR, 2.465; p=0.152) were not significantly associated with postoperative non-pathological fever (Table 2).
DISCUSSION
Most early postoperative fever is caused by surgically stimulated inflammation and resolves spontaneously. However, surgeons associate this fever with infection and therefore administer prophylactic antibiotics. Rates of infection of the surgical site have been reported to be higher following posterior cervical spine surgery (2.9-18.2%) than following anterior cervical spine surgery [14,20,22,28]. Two factors that commonly trigger an evaluation of bacterial infection are 1) fever after the third postoperative day and 2) a temperature above 39℃. However, this practice has not been supported by high-quality clinical research [2,8,26]. In this study, of the 119 consecutive patients who underwent posterior cervical surgery, 28 (24.3%) developed delayed postoperative fever, whereas only one (0.8%) developed surgical site infection. Between pathologic and non-pathologic fever groups, the difference in treatment modality is whether additional antibiotic therapy was administered after prophylactic antibiotics. Pathologic fever was defined as that in which the cause of fever was identified as infectious by the patient’s culture study, and additional antibiotic treatment was started. On the other hand, non-pathologic fever patients did not receive additional antibiotics.
The overall incidence of non-pathologic delayed fever after general spine surgery was 13.2% [23]. To date, there is no literature reporting delayed fever following posterior cervical spine surgery. To the best of our knowledge, this is the first study on homogeneous surgical methods limited to posterior cervical fusion. Previous studies have found that long operation times are associated with a higher prevalence of postoperative fever [3,5,24]. Moreover, in our previous study we reported that a relatively bigger surgery requiring prolonged operation time is a significant risk factor for postoperative non pathologic fever [23]. In that study, the operation time could have been a risk factor because it was analyzed on various surgical methods at various surgical levels within the broad category of general spine surgery. However, in this study we included very homogeneous surgical methods that only involved posterior fusion using CPS for the cervical spine. Therefore, the operation time of each patient was relatively uniform and there was no significant difference in the operation time according to the occurrence of postoperative fever.
All 112 patients included in this study underwent posterior fusion surgery using CPS. This technique has some disadvantages, such as the fact that CPS was inserted through a laterally located starting point and made a large medial angle, similar to an anatomical cervical pedicle lateral angle [18]. This may have resulted in a larger dead space under the incision, leading to postoperative non-pathologic fever despite the absence of infection [23].
Obliteration of the dead space may facilitate wound healing, with careful drainage or obliteration of all dead spaces within a wound regarded as an almost universally accepted precept of surgery [6]. Our previous study of non-pathologic fever in patients who underwent general spinal surgery strongly suggested that surgical site inflammation induced by seroma after drain catheter removal was the cause of fever during the late acute and subacute postoperative periods. High volumes of hematoma or seroma after drain catheter removal in patients who undergo more extensive surgery may also cause fever and tissue trauma, depending on when fever occurs [23]. In contrast, use of a drain at the surgical site was found to be unrelated to postoperative hematoma formation and wound dehiscence [11]. The incidence of postoperative non-pathologic fever after laminectomy was significantly higher than in patients who did not undergo laminectomy. Results from small group head-to-head analysis showed that postoperative non-pathologic fever occurred in 24 of 59 (40.7%) patients who underwent laminectomy and in four of 53 (7.5%) patients who underwent laminoplasty (p<0.001, Table 3). The OR of laminectomy was 10.25 (Table 2). Laminectomy may result in a wider dead space between muscle and dura, with a seroma more likely to be present in this space. These results are in agreement with those of previous studies.
Although minimally invasive muscle preserving laminectomy techniques have been recently introduced, these procedures include decompression only without fusion [16,25]. Cervical laminectomy with posterior fusion is generally known to be a more invasive surgery and have a higher morbidity than laminoplasty [15]. This is not surprising as laminectomy with fusion requires additional muscle exposure, spinal fixation, and bone arthrodesis, which can result in greater intraoperative blood loss and postoperative pain [10,27]. In this study, we only included patients who underwent posterior cervical fusion using CPS. Because of the higher incidence of non-pathologic postoperative fever associated with surgery-induced dead space, we suggest that laminectomy is a more extensive procedure than laminoplasty if combined with fusion.
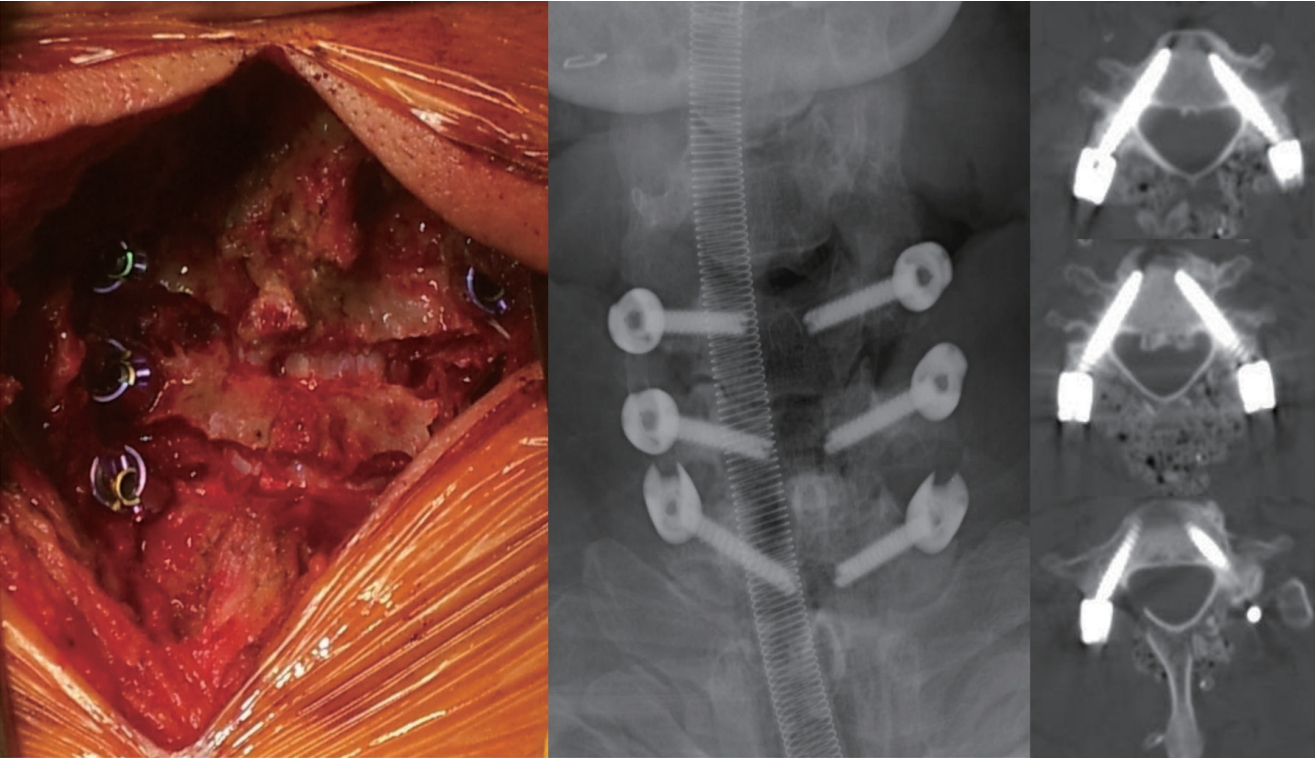
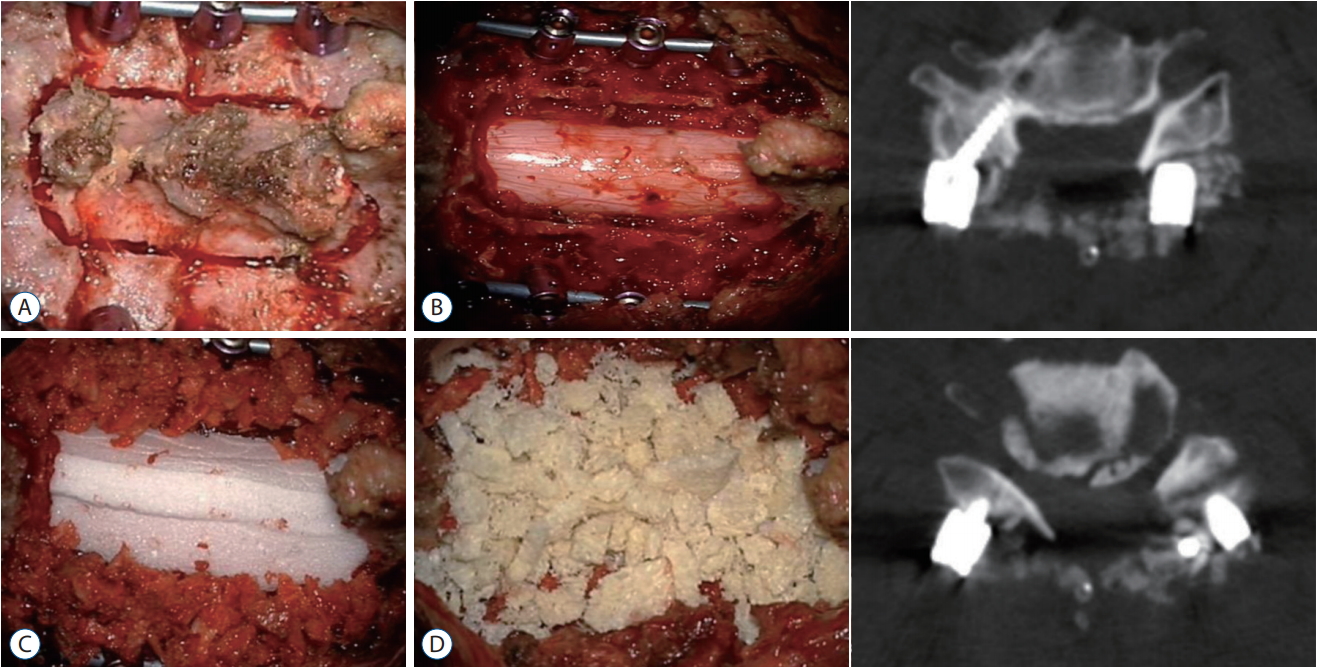
Patients who did not undergo laminectomy included 1) patients with foraminal stenosis who underwent facetectomy with a posterior approach (Fig. 2), 2) patients with sufficient cord decompression achieved by reduction only and instrumentation for cervical subluxation and dislocation, and 3) patients with cervical spondylomyelopathy who underwent laminoplasty (Fig. 3). These methods are superior to laminectomy in reducing dead space and preserving the original anatomical structure between the dura and muscles. Most early postoperative fever is caused by surgery-induced inflammation [9,12,19]. Thus, surgery that preserves the lamina may help to reduce seromas and inflammatory stimuli associated with the dead space, reducing the incidence of postoperative fever (Fig. 4). Moreover, the higher incidence of postoperative fever following more extensive or trauma surgery may be caused by a greater degree of tissue inflammation [1,2,13].
We developed a laminoplasty method to reduce the dead space and create a barrier between the dura and muscle. In the first step, we formed a parallel gutter with a match headshaped burr (Legend Match Head - Fluted; head diameter, 1.7 mm; Medtronic-Sofamor Danek Inc., Memphis, TN, USA) on both sides of the lamina and made it fractured. The lamina was then withdrawn dorsally using the bulged cord. Finally, to maintain lamina elevation, the fractured laminae were anchored using absorbable sutures (Coated Vicryl Plus 1-0; Ethicon, Somerville, NY, USA) through a spinous process. This technique differed from the open-door method of laminoplasty by providing for symmetrical muscle closure in the midline. In addition, this method reduced the dead space by minimizing the space between the lamina and surrounding structures (Fig. 3).
This study had several limitations, including its retrospective design, inclusion of patients treated at a single center by a single surgeon, short follow-up period, and the small sample size.
CONCLUSION
Of the 112 patients who underwent posterior cervical fusion surgery using CPS, 28 (25.0%) developed postoperative fever without infection after 4 days. These results suggest that postoperative fever is relatively common following posterior fusion surgery, especially when laminectomy is performed.