INTRODUCTION
Mechanical thrombectomy (MT) is the primary modality for the treatment of acute ischemic stroke (AIS) caused by large artery occlusion (LAO). In addition, the MT technique continues to evolve in terms of its effectiveness and diversity. Initially, the effectiveness of stent retriever techniques was demonstrated via several randomized controlled trials and meta-analyses, and the usefulness of contact aspiration technique was shown in several studies [2,4,5,9,10,17,20,29,30]. In addition, a number of studies demonstrated that the chance of first-pass reperfusion was increased in Solumbra technique thrombectomy (stent retriever with simultaneous aspiration) [8,16,21,22].
Along with the evolution of MT techniques, devices for thrombectomy have also developed. The Solitaire AB stent (ev3; Covidien, Irvine, CA, USA) was the first stent-retriever device used in MT, and was developed further into the Solitaire flow restoration (FR) device and subsequently to the Solitaire 2 revascularization device. Solitaire is a nitinol stent retriever with laser-cut, attached to a push-wire with a closedcell scaffolding design [27,28]. However, the Solitaire FR stent retriever had a major disadvantage of poor visualization. The next generation Solitaire stent retriever, the Solitaire Platinum (Medtronic, Dublin, Ireland) has radiopaque platinum markers, which are spaced 10 mm apart. The use of a radiopaque device is known to be associated with first-pass reperfusion [12,18]. In addition to the characteristics of the stent retriever, the size of the stent may affect the outcomes of MT. The appropriate stent diameter is disputed, and several reports suggested conflictingly, that a stent with a larger or smaller diameter was better [13,31,33]. However, in terms of stent length rather than diameter, Haussen et al. [12] reported that longer stent retrievers enhance thrombectomy performance, probably due to the larger device-thrombus interaction area and smaller chances of missing the target site.
For these reasons, the authors used Solitaire Platinum 4├Ś40 mm stent retriever with a Solumbra technique. Therefore, the purpose of our study was to assess the potential benefits of SolitairePlatinum 4├Ś40 mm stent retriever with its radiopacity and long length, and compared it with other Solitaire stent retrievers, especially in patients who underwent MT with Solumbra technique. In addition, the technical considerations involved in Solumbra technique thrombectomy with Solitaire Platinum 4├Ś40 mm stent retriever are also discussed.
MATERIALS AND METHODS
Study population
This retrospective study with prospectively collected data was approved by the Local Institutional Review Board (IRB No. VC17RESI0048) of each participating center. The data of patients with LAO who underwent Solumbra technique thrombectomies with a Solitaire stent retriever of equal diameter (4 mm) between January 2018 and July 2019 were obtained from each institutionŌĆÖs stroke database and evaluated. All of the procedures were performed by two experienced neuro-interventionalists at two centers. A total of 70 patients were identified for enrollment. These patients were dichotomized into : 1) a 4├Ś40 group using 4├Ś40 mm Solitaire stent retrievers (Solitaire Platinum 4├Ś40 mm stent retriever) and 2) a 4├Ś20 group using 4├Ś20 mm Solitaire stent retrievers (Solitaire FR 4├Ś20 mm or Solitaire Platinum 4├Ś20 mm stent retrievers). Prior to thrombectomy, intravenous tissue plasminogen activator (IV t-PA, alteplase) was administered to patients within 4.5 hours after stroke onset at a maximum dose of 0.9 mg/kg in accordance with the European Cooperative Acute Stroke Study (ECASS) III trial [11]. The inclusion criteria were as follows : 1) occlusion of the distal intracranial carotid artery (ICA), middle cerebral artery (MCA, M1, or M2), or posterior circulation (vertebral artery, or basilar artery) established by computed tomography angiography (CTA); 2) neurologic deficits; and 3) Solumbra technique thrombectomy with 4 mm Solitairestent retriever. The exclusion criteria were : 1) the detection of hemorrhage on the initial CT scan; 2) presence of a large ischemic core with an Alberta Stroke Program Early CT Score (ASPECTS) Ōēż6; 3) MT with a simple stent retriever or the contact aspiration technique. and (4) Solumbra technique thrombectomy with a stent retriever other than a 4 mm Solitaire stent retriever, such as a Solitaire FR 6├Ś30 mm, a Solitaire Platinum 6├Ś40 mm, a Trevo XP Provue (Stryker Neurovascular, Fremont, CA, USA), Eric (MicroVention Terumo, Tustin, CA, USA), or Revive (Codman Neurovascular, San Jose, CA, USA) devices. All patients underwent CT immediately after the intervention to evaluate hemorrhage. In addition, vessel status and hemorrhage were evaluated by CTA 24 hours after MT. Hemorrhagic transformation of the infarct and vessel status was confirmed by magnetic resonance angiography (MRA) with susceptibility-weighted imaging on day 7 after MT.
Device selection and Solumbra technique
Solumbra technique thrombectomy with a 4 mm Solitaire stent retriever was performed in patients with AIS caused by LAO. All of the MT procedures were performed using the Solumbra technique, entailing thrombus retraction with a stent retriever, such as the Solitaire FR 4├Ś20 mm (ev3; Covidien) or the Solitaire Platinum 4├Ś20 mm or 4├Ś40 mm (Medtronic) and simultaneous aspiration with a 5 Fr SOFIA (Sofia 5; MicroVention-Terumo, Tustin, CA, USA) or a 6 Fr AXS Catalyst 6 (CAT6; Stryker Neurovascular, Mountain View, CA, USA). In almost cases, an 8 Fr balloon-guiding catheter (BGC) (FlowGate2 [FG2]; Stryker Neurovascular, Fremont) was applied. An illustration of MT with the Solumbra technique is shown in (Fig. 1). Under consciousness sedation, an 8 Fr FG2 BGC was placed in the proximal ICA. A microcatheter (Excelsior XT-18; Stryker Neurovascular, Fremont) with a microwire was advanced as distally as possible from the occlusion site, and the aspiration catheter was approached close to the occlusion site, followed by deployment of the stent retriever in the distal portion of the occlusion site. After the 3 to 5 minutes of waiting after stent deployment to promote stent clot integration [32], the aspiration catheter with suction and the stent retriever were slowly removed as a single unit. At this time, a dual aspiration technique was used at the BGC with manual aspiration [15].
Multivariable factors and outcome and complications
Multivariable factors including patient sex, age, risk factors, prior stroke or transient ischemic attack (TIA), history of previous anti-platelet or anti-coagulant use, ASPECTS score, application of IV t-PA, stroke etiology by Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification [1], site of the arterial occlusion, and procedure time (time from groin puncture to reperfusion) were reviewed. All patients underwent clinical assessment using the National Institutes of Health Stroke Scale (NIHSS) (range, 0-42; with higher scores indicating more severe neurologic deficit) and modified Rankin Scale (mRS) scores at 3 months (a favorable clinical outcome was defined as mRS Ōēż2). The radiologic results were evaluated according to the thrombolysis in cerebral infarction (TICI) grading system, successful recanalization (TICI grade of 2b or 3), first-pass reperfusion (modified TICI, mTICI 2b or 3 with the first pass), and first-pass complete reperfusion (mTICI 3 with the first pass). Various complications, such as post-thrombectomy hemorrhage at 24 hours, symptom-related hemorrhage at 24 hours, vessel perforation, arterial dissection, distal emboli, hemorrhagic transformation of the infarct on MRA 7 days after MT, and 3-month mortality were reviewed. Post-thrombectomy hemorrhage at 24 hours was defined as the occurrence of intracerebral hemorrhage or subarachnoid hemorrhage on a CTA scan obtained 24 hours after the procedure. All multimodal factors and clinical data were analyzed by all authors.
Statistical analyses
All data were analyzed using Stata Statistical Software, release 15 (Stata, College Station, TX, USA). Between-group comparisons were calculated using StudentŌĆÖs t-test/Mann-Whitney U test or chi-squared test/FisherŌĆÖs exact test. Multivariate logistic regression analyses were performed for variables with <0.2 level of significance in univariate analysis. Two-tailed p-value of Ōēż0.05 were considered to indicate significant difference.
RESULTS
Baseline characteristics and procedure detail
Twenty-five patients (14 males, 56.0%) were treated via Solumbra technique thrombectomy with 4├Ś40 mm Solitaire Platinum stent retriever (4├Ś40 group), and 45 (27 males, 60.0%) underwent Solumbra technique thrombectomies with 4├Ś20 mm Solitaire stent retrievers (4├Ś20 group). The mean age of the patients in the 4├Ś40 group was 72 years (standard deviation [SD], 12.7) and that of the 4├Ś20 group was 69 years (SD, 13.1). There were no significant differences in multiple risk factors such as hypertension, diabetes mellitus, atrial fibrillation, coronary artery disease, dyslipidemia, smoking, history of prior stroke or TIA, history of anti-platelet use, previous anti-coagulation use, the proportion of left hemisphere strokes, and the rate of IV t-PA application, between 4├Ś40 and 4├Ś20 groups. The median initial NIHSS value, and ASPECTS scores were 10 and 9, respectively, in the 4├Ś40 group and 8 and 9, respectively, in the 4├Ś20 group, without significant difference. There was no significant difference in stroke etiology between the two groups. The site of arterial occlusion in each group was as follows (4├Ś40 group : 4├Ś20 group) : MCA, 13 : 27; distal ICA, 10 : 13; and posterior circulation, 2 : 5. In terms of procedure, there were no statistically significant differences in procedure time and the rate of BGC application between the two groups (p=0.247 and 0.776, respectively). The distribution ratio of the two-aspiration catheters (CAT6 : Sofia5) was 21 : 4 in the 4├Ś40 group, and 33 : 12 in the 4├Ś20 group (p=0.186). Radiopaque devices were significantly more common in the 4├Ś40 group (p=0.001), suggesting that 25 non-radiopaque Solitaire FR 4├Ś20 mm stents were included in the 4├Ś20 group (Table 1).
Outcomes and complications
No statistically significant difference was found in the rate of successful recanalization, between the two groups (4├Ś40 group : 4├Ś20 group, 96.0% : 95.6%; p=0.842). However, the proportion of first-pass reperfusions and first-pass complete reperfusions was significantly higher in the 4├Ś40 group, compared to the 4├Ś20 group (68.0% vs. 46.7% and 48.0% vs. 33.3%, p=0.004 and 0.007, respectively). There were no significant differences in complications, between the two groups (Table 2).
Predictors of reperfusion and full reperfusion with first pass
In multivariate logistic regression analysis, the use of radiopaque Solitaire stent retriever (odds ratio [OR], 2.08; 95% confidence interval [CI], 1.22-3.84; p=0.014), and longer Solitaire Platinum 4├Ś40 mm stent retrievers (OR, 2.81; 95% CI, 1.34-4.10; p=0.008) were correlated with first-pass reperfusion. In addition, multivariate logistic regression analysis for first-pass complete reperfusion indicated that the use of radiopaque devices (OR, 1.88; 95% CI, 1.20-3.12; p=0.022) and longer Solitaire Platinum 4├Ś40 mm stents (OR, 2.12; 95% CI, 1.48-3.76; p=0.012) were independent predictors (Table 3).
DISCUSSION
Currently, the development of various thrombectomy techniques has enhanced the clinical and radiologic outcomes of patients with LAO [6,7,19]. Recent advances in MT pursuit the first pass effect (first-pass reperfusion or first-pass complete reperfusion), beyond simple successful recanalization [25]. The importance of the first-pass effect has been reported in various studies, where it was associated with a significantly higher chance of favorable clinical outcomes with the retrieval of the entire thrombus as a single mass on the first attempt [23,24,34]. Fewer stent passages reduced the risk of procedure-related complications, such as parenchymal hematoma and other vessel damage [3]. Therefore, the utility of the Solumbra technique contributes to reperfusion or complete reperfusion from the first pass [14,21,25]. Based on these studies, the authors used Solumbra technique for MT in most cases. In addition to thrombectomy techniques, the device may be considered a factor affecting the outcomes of MT. There are several controversies related to the selective advantages of stent retrievers with an appropriate diameter. However, recent studies have suggested that stent retrievers with longer lengths and radiopaque characteristics yield better outcomes [12,13,18,31]. In our study, longer and radiopaque stent retrievers were found to increase the first-pass effect. The reperfusion and complete reperfusion rates with first pass were significantly higher in the group with 4├Ś40 mm long stent retrievers than in those with 4├Ś20 mm short stent retrievers. Furthermore, the multivariate analysis in our study showed that stent retrievers with longer length and radiopacity improved the first-pass effect in MT with Solumbra technique. These findings revealed the effectiveness of Solitaire Platinum 4├Ś40 mm stent retrievers compared to other 4 mm Solitaire stent retrievers, especially in MT with the Solumbra technique.
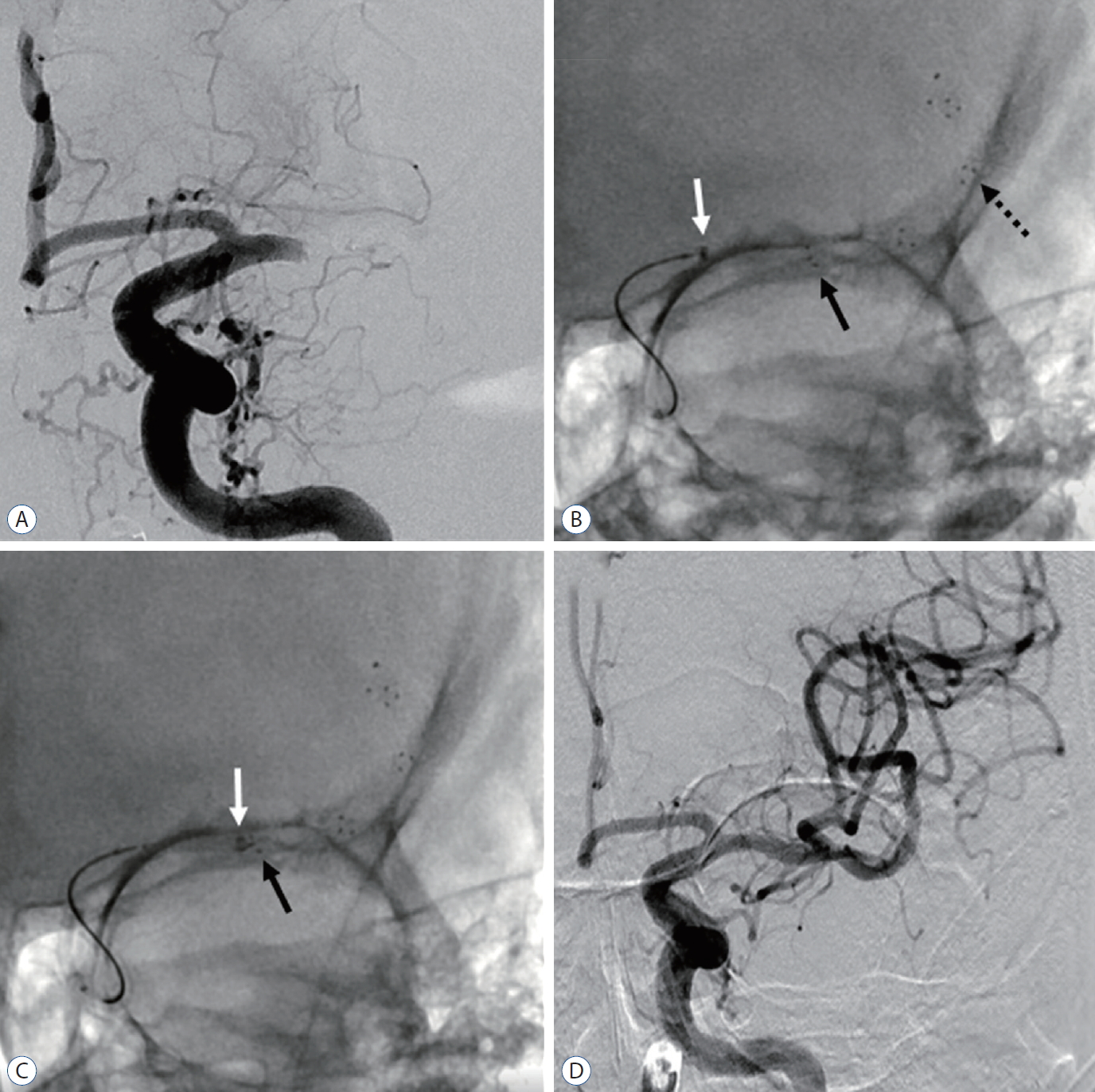
Longer stent retrievers have theoretical advantages because of the larger interaction area between the device and the thrombus, with lower chances of missing the target site than their shorter counterparts. In addition, the radiopaque characteristics of the device allow the interventionalists to view the entire stent, and confirm its optimal location and adequate vessel-wall apposition of the stent. Based on these characteristics, the usefulness of the Solitaire Platinum 4├Ś40 mm stent retriever and its technical considerations during the Solumbra technique thrombectomy was shown in (Fig. 2). Under roadmap guidance, the microcatheter was navigated distal to the occlusion site, and the Solitaire Platinum 4├Ś40 mm stent retriever was deployed to cover the distal and proximal ends of the occlusion. The aspiration catheter was navigated close to the clot, and the microcatheter was removed to increase the aspiration flow (Fig. 2A) [26]. Next, the stent retriever was gently pulled with weak force and the distal tip of the aspiration catheter was moved to the distal lesion as close to the occlusion site as possible to contact the thrombus. At this time, the distal tip of the aspiration catheter should be placed just proximal to the site of the thrombus, between the two markers (mid-portion of the marker and the proximal end of the working length marker) of the Solitaire platinum 4├Ś40 mm stent retriever (Fig. 2B). After waiting several minutes to enable stent-clot integration, retrieval of the whole Solumbra system was performed for clot retrieval, with simultaneous continuous suction at the aspiration catheter and dual aspiration through the BGC. When the distal tip of the aspiration catheter was adequately positioned between the mid-portion marker and the proximal end of the working length marker without crossing the mid-portion marker, the thrombus could be retrieved as a single mass (Fig. 2C). However, frequent failures associated with thrombus retrieval occurred when the distal tip of the aspiration catheter was located more distally, beyond the mid-portion of the stent, and re-captured more than half of the stent retriever (Fig. 2D).
In the thrombectomy procedures using the Solumbra technique, the aspiration catheter should re-capture less than half or one-third of the stent retriever to ensure an adequate stent retriever capture area to fully integrate with the clot. In addition, during the Solumbra system retrieval, the aspiration catheter is moved further distally depending on its tension, and the stent retriever is captured further by the aspiration catheter. In addition to the advantage of a long stent, the radiopacity of the Solitaire Platinum 4├Ś40 mm stent retriever with its markers 10 mm apart facilitate the correct positioning of the aspiration catheter and adjust the adequate capture range of the stent retrievers, especially during Solumbra technique thrombectomy. Therefore, a long and radiopaque stent retriever such as the Solitaire Platinum 4├Ś40 mm stent retriever, is preferred for MT by Solumbra technique.
The major limitations of this study were its relatively small sample size, and the retrospective non-blinded format. Since thrombectomy in the 4├Ś20 mm Solitaire stent retriever group was performed earlier than in the 4├Ś40 mm Solitaire Platinum stent retriever group, it may be assumed that the learning curve affected the outcome. However, all thrombectomy procedures in this study were performed by neuro-interventionalists with several years of experience. Therefore, the learning curve would not have a significant influence on the outcome. Furthermore, the baseline characteristics in the two groups were well balanced and there were no statistically significant differences. The disadvantages of longer stent retrievers include vessel damage or larger interface area with the vessel and consequently more friction. However, in our study, there were no significant differences in hemorrhage and dissection between the two groups. In addition, our study did not include the data associated with Solitaire FR 4├Ś40 mm retriever, which is a non-radiopaque and long Solitaire stent retriever. Other potential unmeasured confounding variables were not controlled for, although every effort was made to adjust for the possibility of spurious results.
CONCLUSION
In this study, the use of the Solitaire Platinum 4├Ś40 mm stent retriever for Solumbra technique thrombectomy in patients with LAO was highly effective, without increased periprocedural complications, compared with prior versions of the Solitaire FR 4├Ś20 mm stent and the Solitaire Platinum 4├Ś20 mm stent. The radiopacity and long length of the Solitaire Platinum 4├Ś40 mm stent retriever may contribute to more achievement of first-pass reperfusion and first-pass complete reperfusion, especially with Solumbra technique thrombectomy. Future prospective multicenter and in vitro studies are needed to corroborate our findings.