INTRODUCTION
Lumbar disc herniation (LDH) and lumbar stenosis are common spinal pathologies. While lumbar stenosis is more common in the elderly, LDH often affects the younger population and is thus, more associated with loss of productivity in the socio-economic aspect.
Hence, the medical community has examined different aspects of LDH and lumbar discectomies, the primary surgical treatment for LDH [8]. Epidemiologic trends including incidence, demographic factors and different surgical approaches have been delved into but have shown relatively small changes during the last decade [9]. Surgical results, infection rates and recurrence rates are also commonly studied [2,16,18]. For many surgeons, the focus has been on reducing LDH recurrence rates and postoperative infection rates.
However, little has been studied regarding the loss of work capability after LDH. There are no reports on the loss of work capability after conservative treatments for LDH and scant studies on post-discectomy loss of work capability. The evaluation of loss of work capability after lumbar discectomy is very difficult and complex due to the numerous intertwining factors that affect the opportunity cost of lumbar discectomies.
Furthermore, the patients undergoing lumbar discectomies and their employers want clear answers about how long the patient would need sick leave and whether the patient could return to their previous job. Of course, these questions are also very difficult to answer because there are many variables and unexpected complications.
Overall, the complication rate of microdiscectomies is 10.8% [17]. Nerve root injury, surgical error, durotomy, hematoma, wound complication, recurrent herniation and reoperation were reported as complications after lumbar disc surgery. In contrast, the success rate after lumbar disc surgery is about 80% (63-96%) [5]. Assuming that patients without postoperative complications have had successful discectomies, we should further study these patients in order to better understand the socio-economic effects of lumbar discectomies.
This study is a prospective observational study of how long it takes for the patients who undergo single segment lumbar discectomies without complications to return to work (RTW). We also investigated the overall rate of patients returning to work and recorded their clinical evaluations at the time of RTW. In addition, this study examined how employment type is related to the RTW period as a social factor.
MATERIALS AND METHODS
This study was approved by the Institutional Ethics Review Board of Chuncheon Sacred Heart Hospital, Hallym University Medical Center (CHUNCHEON 2014-01-003). This study investigated the RTW in patients without complications after lumbar discectomies. Thus, factors and complications that may adversely affect the surgical results were excluded. This study also focused on patients with regular jobs, so that we could document the RTW status. Surgical indications were for patients who were diagnosed with LDH on magnetic resonance imaging (MRI) and did not respond to conservative treatment for at least 6 weeks. All patients underwent surgery with one of three spinal surgeons at our institution. The operations were performed using microscopic discectomy techniques. The patients were discharged 3 days after surgery began outpatient follow-up 2 weeks after surgery.
Inclusion criteria : patients with regular jobs who underwent surgical treatment for single-segment LDH between September 2014 and December 2018. Exclusion criteria : patients with previous discectomies at other levels or instrumentations, including dynamic fixation or motion segment preservation. Patients with recurrent disc herniation at the same level after discectomy, multilevel discectomies, postoperative infections, postoperative hematomas, or severe neurologic deficits at presentation, such as cauda equina syndrome. Patients who suffered trauma after the discectomy, such as mild traumatic brain injury, falls, and compression fractures. Patients with spondylolysis and spondylolisthesis. Patients lost to follow-up or unable to interview by phone.
Preoperatively, the sex and age of the patients were recorded for demographic analysis. The degree of pain at presentation and prior to surgery was assessed by the Oswestri Disability Index (ODI) and the Numeric Rate Scale (NRS). Preoperative muscle strength was measured using the Royal Medical Research Council of Great strength grading scale. We evaluated disc degeneration at the surgical level and at the most degenerated level using the Pfirrmann grade on the MRI [7]. The degree to which the nerve roots were compressed by the herniated disc was measured from 1 (minimum) to 5 (most severe) according to Kang et al.'s report [10,11].
Postoperatively, outpatient or telephone interviews were conducted at 1-month intervals. At the time of each interview, pain assessments were conducted using the ODI and the NRS. For the socioeconomic evaluation, the type of employment was divided into self-employed, regular employee, and contracted employee. If a patient could not RTW within 6 months, the patient was judged to have failed to RTW. Patients who could perform telephone interviews after returning to work were also asked to self-evaluate the degree of loss of their own work capability at 6, 12, and 18 months after surgery.
The duration of hospital stays and weeks until RTW were measured. The period until RTW, the pain at RTW, and the failure rate to RTW were compared by employment type.
RESULTS
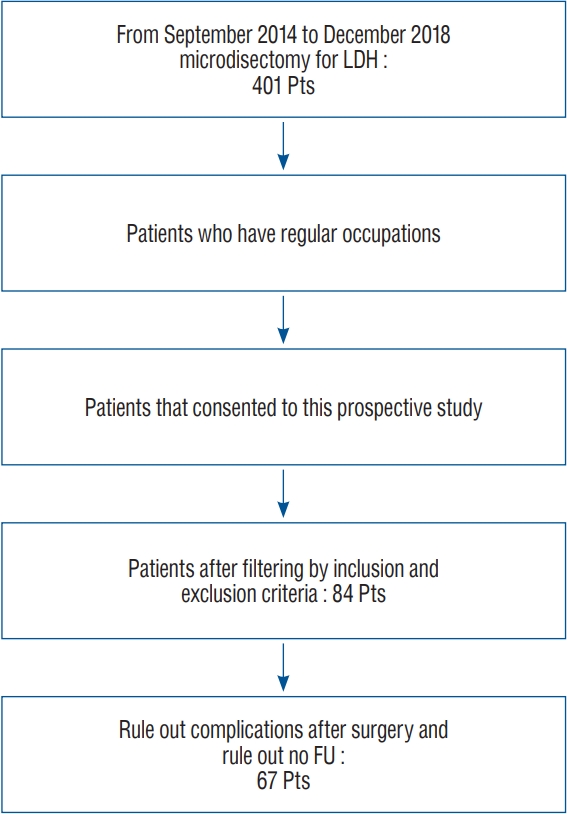
This study was a prospective observational study in a single institution. The authors performed 850 spinal surgeries from September 2014 to December 2018. Among them, 401 were microdiscectomies for LDH, and 84 patients were eligible for this study. Their average age was 43.3±9.4 years, with mean age 44.1±1.0 years for males (n=68) and 40.1±3.0 years for females (n=16). Seventeen cases were removed from analysis due to lack of follow-up, infection, or re-operation, and 67 patients remained in our final analysis (Fig. 1).
Of the 67 patients analyzed, there were 54 males and 13 females. The average age was 42.5±9.3 years. During the 6 months after surgery, three patients failed to RTW, and three others resigned after 4 weeks, 9 weeks, and 3 months of returning to work, respectively. The six patients who could not RTW were two accommodation workers, one self-employer of a restaurant, one regular desk worker, one truck driver and one construction worker.
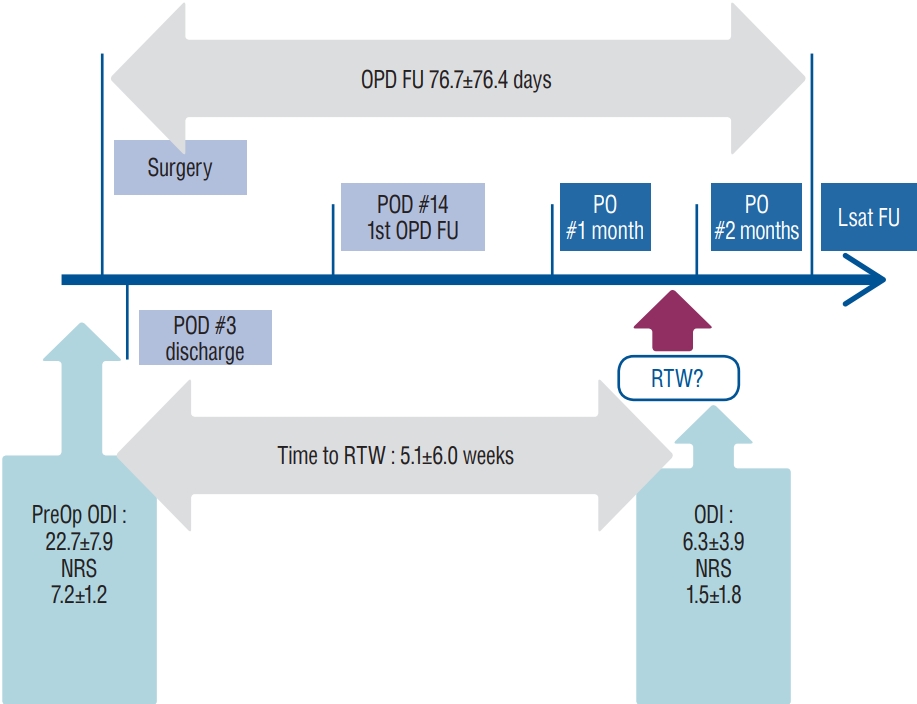
Sixty-one patients (51 males and 10 females) successfully returned to work after lumbar discectomy. The mean age of these patients was 42.0±8.2 years. Clinically, the preoperative average symptom duration was 10.6±26.2 weeks. The preoperative NRS and ODI were 7.2±1.2 and 22.7±7.9, respectively. Mean postoperative hospital stay was 3.6±0.9 days, and the final outpatient follow-up period was 76.7±76.4 days. The time to RTW was 5.1±6.0 weeks. At the time of RTW, NRS was 1.5 ±1.8 and ODI was 6.3±3.9. NRS at the last follow-up was 0.6±1.2 and ODI was 2.8±3.1, respectively (Fig. 2).
There were no clinical, radiological or insurance differences between males and females except NRS when they returned to work (Table 1).
Amongst the patients that returned to work, there were 16 self-employed workers, 42 regular employees and three contract workers. The time to RTW of self-employed, regular and contract workers were 5.9±8.8, 4.2±4.3, and 13.3±2.3 weeks, respectively (analysis of variance, p=0.030).
At the time of RTW, the ODI was 6.8±3.6 for the self-employed, 6.5±3.9 for full-time workers and 1.0±1.7 for contract workers (p=0.049) (Table 2).
The 61 patients also self-estimated the loss of their work capabilities at 6, 12, and 18 months after the discectomies. Twenty-five patients reported no loss of labor force 6 months after discectomy. The other 36 reported reductions in productivity at 6 months postoperatively. They estimated that they had lost 22.8±15.6% of their work capability compared to the preoperative baseline. No one changed jobs or positions after RTW.
Factors potentially associated with loss of work productivity after RTW were assessed. There were no differences in clinical factors, including preoperative pain severity, preoperative motor weakness, and surgical outcomes. There were also no differences in employment status, insurance type and time to RTW. There were no statistical differences in MRI findings, such as root compression and Pffirmann grade of disc degeneration (Table 3).
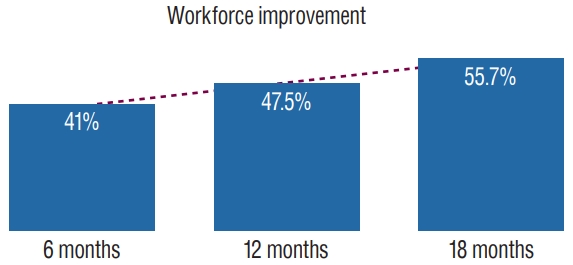
The self-estimated loss of work productivity changed over time. The number of patients that reported no loss of productivity increased from 25 at 6 months to 29 at 12 months, and then to 34 at 18 months after surgery. Overall, the self-estimated loss of productivity decreased over time (Table 4 and Fig. 3).
DISCUSSION
The objective of this study was to determine the economic implications of surgical treatment of LDHs. The study included 67 patients in a prospective observational study conducted at a single institution. The patients returned to work at an average of 5.4 weeks after single-level lumbar discectomies. Six of 67 patients (9.0%) were unable to RTW within 6 months following surgery. Six months after surgery, 25 out of 67 (41.0%) reported no loss of work capability, while 36 reported some loss of work capability.
In reviewing the literature, there are very few studies on RTW after spinal surgery compared to other topics. The timeframe to RTW after spinal surgery is necessary data, but it is difficult to investigate properly and researchers are generally less interested in the topic. Instead, they are more interested in the surgical results and complications than in assessing when patients RTW. A few studies have investigated the duration of sick leave prior to RTW in patients after lumbar discectomies, but interestingly, the results vary widely depending on the country of origin.
In our South Korean study, the patients returned to work 5.4 weeks after lumbar discectomies. In contrast, a Denmark paper on RTW after lumbar discectomy reported different results. The authors investigated RTW in 351 patients, of whom 62% returned to work within 2 years after lumbar discectomy [19]. The study reported that sustained RTW was associated with high education level, positive expectation towards future labor market attachment, preoperative stable labor market attachment, preoperative higher physical quality of life, and less disability.
On the other hand, a German group demonstrated that the type of employment affects the RTW after lumbar discectomies [1]. In this study of 511 patients, the mean time to RTW was 10.5 weeks. Self-employed people returned to work in 5.4 weeks, civil servants in 10.2 weeks, and regular employees in 14 weeks. While the duration differs from our data, their results demonstrated similar findings to our own, that RTW is associated with the patients’ social status.
Finally, a Turkish military doctor reported that about 6 weeks is required before patients can RTW [4]. Others have reported good-to-excellent clinical results in nearly 90% of patients after lumbar discectomy, with the majority returning to work within 1 month [12].
Different social security systems across countries may explain some of the variations in the patients’ ability or willingness to RTW after lumbar discectomies. For instance, Schade et al. [15], reported that RTW was not influenced by any clinical findings or MR-identified morphological alterations, but rather, depended solely on psychological factors (i.e., depression) and psychological aspects of work (i.e., occupational mental stress). Interestingly, there are some reports that longer sick leaves are negative predictors of patients’ RTW. Silverplats et al. [18], reported that patients taking sick leaves longer than three months showed a lower RTW rate than those who took less than 2 months of sick leave after lumbar discectomies.
Other studies have investigated factors related to RTW. There have been reports of longer labor loss periods in patients with clinically persistent symptoms 2 months after surgery. Puolakka et al. [13] reported that ODI >20, leg pain, and poor motivation to work were risk factors for extension of work disability. Furthermore, newer minimally invasive discectomies led to shorter hospital stays and earlier RTW compared to microdiscectomy or open discectomy [14]. In terms of postoperative rehabilitation, 10.1% of patients who received rehabilitation did not have RTW, compared to 18.1% of the control group that did not undergo postoperative rehabilitation [6]. Operative techniques and postoperative rehabilitation may be more interesting for surgeons performing lumbar discectomy because these factors can be modulated to affect postoperative outcomes.
Finally, lumbar discectomies may affect the patients’ systemic health. Bosković et al. [3] reported that the quality of life and mental health values after lumbar microdiscectomies, as measured by the SF36-PHYS domain improved from 25.7 at the beginning of the study to 46.4 over the following 6 months. Likewise, in our study, we found that the self-estimated loss of work productivity gradually improved over 18 months after surgery. This information is important to patients and should be communicated to dispel some of the concerns regarding lumbar discectomies (Table 4 and Fig. 3).
A limitation of this study is the small number of enrolled patients. Because personal information related to occupation is the content of the study, there were many patients who could not be enrolled in the study, and many patients refused to be enrolled in the study. In addition, some patients were excluded due to complications such as infection. It would be nice if more subjects were enrolled, but the results are not expected to make a significant difference.
Specifically, the number of contract workers was relatively small compared to other employment statuses. Despite the small sample size, we were able to demonstrate that it seems to take contract workers longer to RTW, at 13.3 weeks (p=0.030). Contract workers also reported better ODI when they returned to work (p=0.049) (Table 2).
Perhaps, in the case of contract workers, they may not want to reveal their employment status and refused to participate in the research because of their employment type. Or they may have already decided to stop working before surgery. There is a possibility that contract workers could not get a job for longer periods compared to other groups after surgery according to their job. An employer who knows that a contract employee has undergone surgery may have advised him to work again after the workforce is recovered. We think these results are evidence that the employment of contract workers is unstable compared to other groups regardless of the disease.
Six patients were unable to return to work or quit work within 6 months. We did an investigation into the jobs of those six people. However, we have not investigated whether the six quit work for personal reasons or if they quit work due to a loss of workforce due to surgery. It is another one of the limitations of this study.
Overall, this study provides valuable data in demonstrating that patients’ employment status may affect their ability to return to work successfully after lumbar discectomies. Although the sample size was small, we believe the results of this study should be considered when surgeons discuss potential surgical outcomes with patients.
CONCLUSION
Lumbar discectomy is associated with loss of work productivity. In this study, six of 67 patients (8.95%) did not return to work, about 5 weeks of sick leave were required after single segment lumbar discectomies. The length of sick leave after lumbar discectomy is associated non-clinical factors (i.e., employment state). Loss of work capability occurred after lumbar discectomies; however, more than 40% of patients reported no productivity loss 6 months after surgery.