INTRODUCTION
The primary goal of spinal surgery is to attain sufficient neural recovery from the damaged spinal cord and roots. Several methods have been developed to achieve optimal results for various disorders in the cervical spine, including degenerative diseases, traumatic injuries, and tumors. There are two main surgical approaches employed in the cervical spine : the anterior approach and the posterior approach. Anterior cervical surgery includes anterior cervical discectomy and fusion, and posterior cervical surgery includes laminectomy alone, laminoplasty, and laminectomy and fusion (LF).
The anterior approach surgery has an advantage due to its direct decompression of compromised structures. However, the rates of dysphagia and recurrent laryngeal nerve palsy are relatively high compared with the rates obtained with the posterior approach [13]. Additionally, the degeneration of adjacent levels can occur with the anterior procedure [2]. Posterior approaches, including laminectomy alone, laminoplasty, and LF, are usually conducted in cases of multilevel cord compression. Shifting the spinal cord posteriorly induces indirect decompression. However, laminectomy alone is generally avoided due to the risk of delayed postlaminectomy kyphosis [11]. Laminoplasty is performed as an alternative to laminectomy, achieving sufficient decompression and mechanical solidity [3,4]. LF provides better long-term stability than laminectomy alone by inducing arthrodesis and has a wider surgical indication than laminoplasty as it facilitates lordotic change from kyphosis [1]. However, complications after posterior surgery, such as axial pain, C5 palsy, postoperative kyphosis, and pseudomembrane formation are not uncommon [7,12].
The appropriate surgical method for cervical disorders has been controversial for many years. In this study, we present an innovative surgical method for cervical spine disorders entitled posterior floating laminotomy (PFL), which overcomes the drawbacks of LF while retaining the strengths of laminoplasty.
MATERIALS AND METHODS
Patient enrollment
This study was performed under an Institutional Review Board-approved protocol in compliance with regulations set by Gangneung Asan Hospital (IRB No. 2019-11-006), and no patient consent was required as no identifying material has been included. We retrospectively reviewed the medical records of patients who underwent cervical spinal surgery between 2012 and 2019. A total of 85 patients were enrolled. Conventional LF was performed on 66 patients from 2012 to 2019, while PFL was consecutively performed on 19 patients from 2016 to 2019. From 2016, the surgical method was determined on a case by case basis. Surgery indications were trauma, cervical spondylotic myelopathy, ossification of posterior longitudinal ligament, foraminal stenosis, and tumor. Surgical indications were not different between the groups and detailed classification are described in Table 1. Exclusion criteria were patients with infection, corpectomy, and fusion including the C1 or below the T2 level.
Surgical methods
A cervical pedicle screw (CPS) and a lateral mass screw (LMS) were used for both the conventional LF group and the PFL group. When ball-tip probing, feedback suggestive of malpositioning of the screw led to abandonment of the CPS procedure and conversion to LMS insertion.
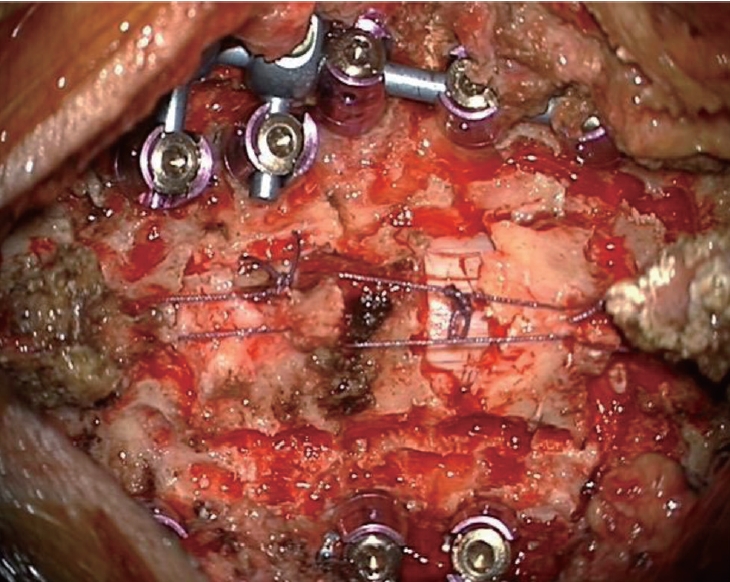
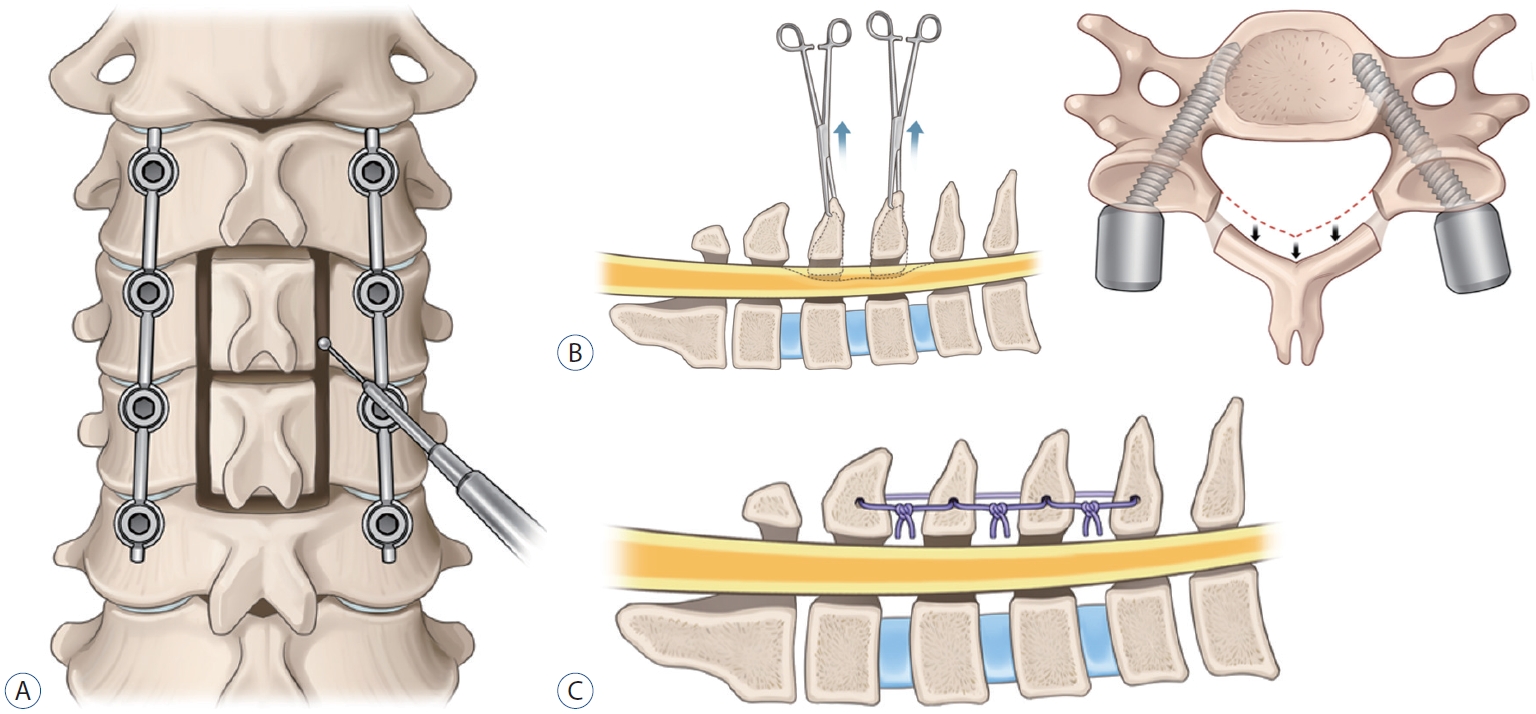
In the conventional LF group, after confirmation of the screw position by anterior-posterior and lateral radiographs, laminectomy was performed using a high-speed drill with a small round burr (1.8 mm). Additionally, decorticated local bone (i.e., spinous process and lamina bone chips) mixed with allobone was applied over the duraform, which covered the spinal cord, to promote segmental fusion and was used for posterolateral fusion. In the PFL group, laminotomy was performed using a high-speed drill with a small round burr to make gutter. Next, only the lamina without ligamentum flavum was disconnected en bloc and shifted to posteriorly with Allis forceps while some proportion of ligamentum flavum was preserved, since the isolated lamina is unstable and difficult to reattach to the original sites. If the inner layer of the lamina compressed the spinal cord even after posterior shifting, additional internal decompression through removal of inner wall of lamina, central part of ligamentum flavum, or epidural fat was performed. After shifting posteriorly, floating lamina was adhered to the paraspinal muscles, tendons, and upper and lower spinous processes with threads (Fig. 1). Lastly, decorticated bone chips were applied at the gutter to make bone fusion for long-term stability. Schematic images of the surgery are illustrated (Fig. 2).
Outcome evaluation
A comprehensive review of medical records was performed to gather data regarding the baseline characteristics, radiological parameters, and functional outcomes. The baseline characteristics of the patients, including age, sex, diabetes mellitus (DM), hypertension (HTN), smoking, body mass index (BMI), osteoporosis, history of previous cervical operation, and classification, were recorded.
The radiological parameters were analyzed with lateral spine X-rays before surgery, immediately after surgery, and at the last follow-up. We measured cervical lordosis (CL), the T1 slope (T1S), segmental lordosis (SL), and the C2-7 sagittal vertical axis (SVA) on lateral spine X-rays. CL, defined as the C2-7 Cobb angle, was evaluated based on the angle between the lower endplate of the C2 vertebra and the lower endplate of the C7 vertebra. T1S was evaluated based on the angle between the upper endplate of T1 and the horizontal line. SL was evaluated from the angle between the upper endplate of the upper instrumented vertebra and the lower endplate of the lower instrumented vertebra. C2-7 SVA was measured as the distance between a plumb line from the center of the C2 body to the superior posterior endplate of C7. These measurement methods are presented in Fig. 3.
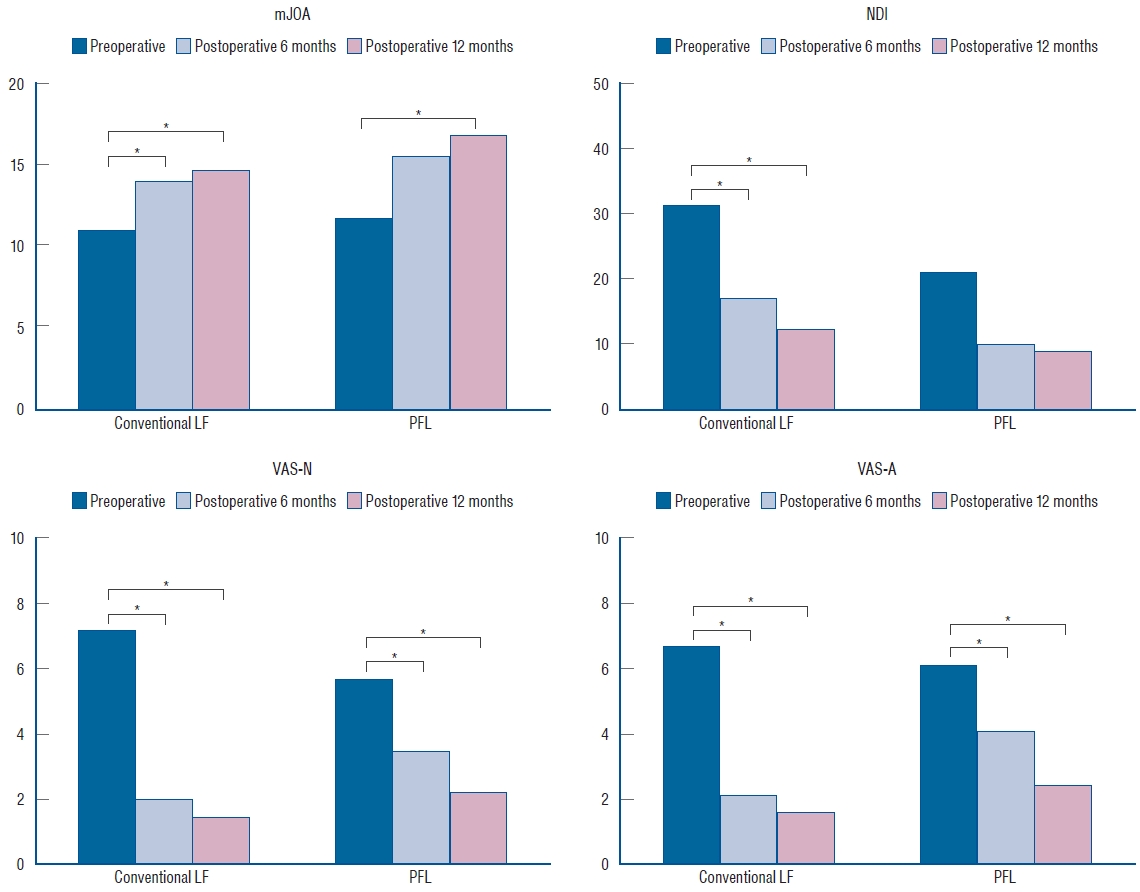
In addition to radiological parameters, functional outcomes were obtained before surgery, immediately after surgery, and at the last follow-up. Functional outcomes consisted of modified Japanese Orthopaedic Association (mJOA), neck disability index (NDI), and visual analog scale (VAS) scores. The mJOA score is a quantitative scale that evaluates the severity of myelopathy. The scale is representative of four components : 1) motor function in the arms, 2) motor function in the legs, 3) sensation, and 4) bladder function. Scores are estimated from 0 to 17, with a lower score correlating with higher disability [10]. The NDI score is a clinical assessment of disability, specific to the cervical spine, which has a high degree of reliability and internal consistency [28]. The scores are estimated from 0 to 50, with a higher score correlating with higher disability. Pain severity was measured with the VAS score, with VAS for the neck (VAS-N) and the arm (VAS-A). The VAS score was measured from 0 to 10, with 0 representing no pain and 10 representing the worst pain [15].
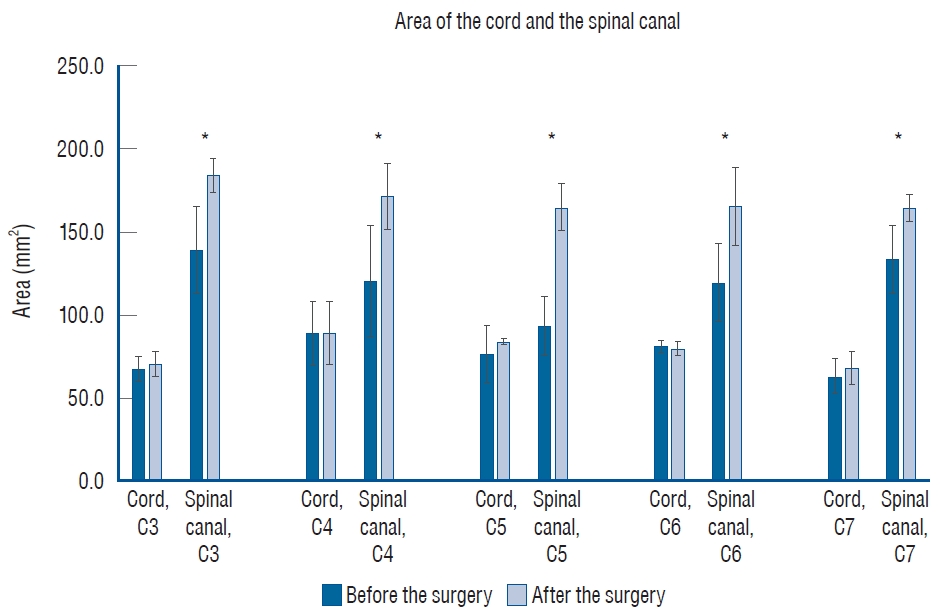
We performed the postoperative magnetic resonance image (MRI) in 1 month after the PFL surgery to evaluate the degree of decompression. From the T2-weighted axial images, the area of the cord and the spinal canal were measured at each pedicle level from C3 to C7, before and after the surgery (Fig. 4). To discriminate the subarachnoid space from the ligamentous or osseous structures, we set the borderline of the spinal canal area (i.e., the subarachnoid space) along the inner margin of low signal intensity [22,25]. The measurements were viewed on Surgimap software version 2.3.1 (Nemaris Inc., New York, NY, USA). All parameters were measured independently by two observers, and the average value of each parameter at each level was taken for independent calculations.
Postoperative computed tomography (CT) images were obtained immediately and 1 year after the operation to evaluate fusion status. Fusion was defined as definite bony bridging on axial CT images. Perioperative data such as the number of levels fused, screw fixation method, estimated blood loss (EBL), length of hospital stay (LOS), operation time, non-pathologic fever defined as a fever without an infection [26], and perioperative complications were also collected. Complications were defined as any subsequent event after the operation requiring further treatment.
Statistical analysis
Quantitative data were presented as the mean┬▒standard deviation unless otherwise indicated. Independent T-tests were used to assess continuous variables. Chi-square test and FisherŌĆÖs exact test were used for categorical variables. Significant differences in functional outcomes among the three different time points were assessed using one-way repeated measures analysis of variance (ANOVA). We performed a Bonferroni correction on one-way repeated measures ANOVA and the variables were considered statistically significant with p<0.017. For all the other analyses, the results were considered to show statistical significance when p<0.05. All statistical tests were two-sided. We used R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria) for all statistical analyses.
RESULTS
Of the 85 included patients, 66 patients received conventional LF and 19 received PFL. There was no difference between the groups regarding the age (p=0.53), sex (p=0.31), DM (p=0.37), HTN (p=0.69), smoking (p=1.00), BMI (p=0.83), osteoporosis (p=1.00), history of previous cervical operation (p=0.22), and classification (p=0.24). These baseline characteristics are summarized in Table 1. After the operation, all degenerative patients demonstrated neurological improvement and none of the trauma patients with spinal cord injury experienced aggravation of their neurological function in either group, except one case of restenosis in PFL group due to the postoperative cervical trauma.
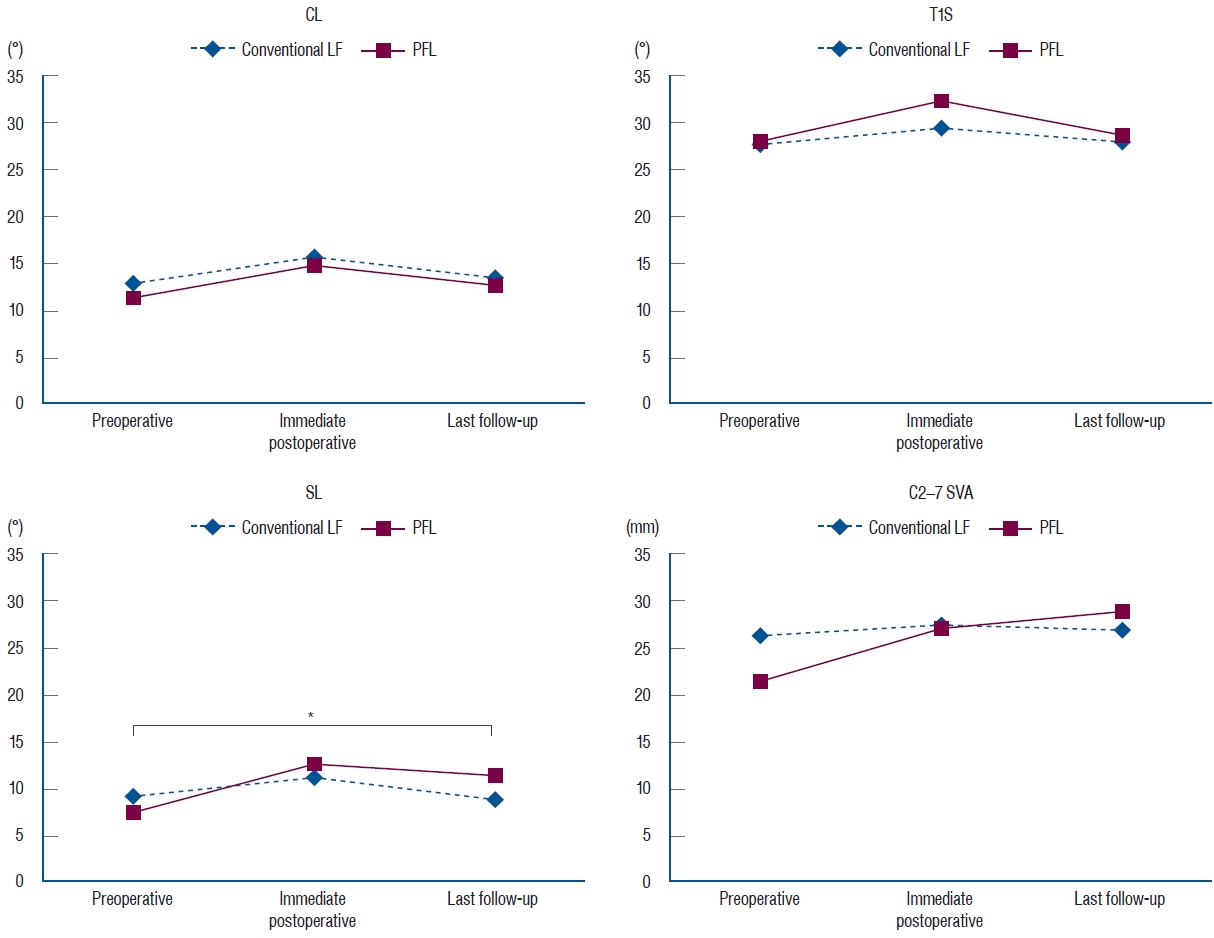
Radiological parameters, including CL, T1S, SL, and C2-7 SVA, were not different between the groups, but a difference was observed in the SL angle preoperatively and at the last follow-up. SL difference between the preoperative time and the last follow-up was -0.3┬░ in the conventional LF group and 4.7┬░ in the PFL group (p=0.04) (Table 2 and Fig. 5). Functional outcomes, consisting of mJOA, NDI, VAS-N, and VAS-A scores, were measured at the preoperative time, postoperative 6 months, and postoperative 12 months and showed significant differences (p<0.05) in each group (Table 3 and Fig. 6).
The area of the cord and the spinal canal from C3 to C7 which was measured at the T2-weighted axial MRI are presented in Table 4 and Fig. 7. There were statistically significant differences in the area of the spinal canal from C3 to C7, between before and after the surgery. Follow-up CT 1 year after the operation revealed the formation of bony continuity at the gutter between the lateral mass and the lamina, whereas immediate postoperative CT showed a gap between the lateral mass and the lamina (Figs. 8 and 9). Although it was difficult to specify when the bone fusion occurred, it was possible to identify the fusion status with a CT scan.
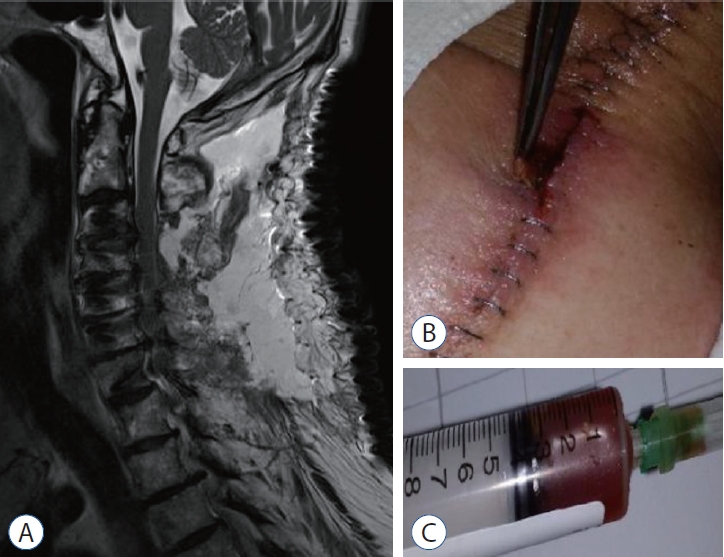
Perioperative outcomes are presented in Table 5. The numbers of levels fused after conventional LF and PFL were 2.8 and 3.0 (p=0.48), respectively. Screw fixation methods were not different between the groups (p=0.42). Although the total operation times for the conventional LF group and the PFL group were different (conventional LF : 169.6 vs. PFL : 223.7 minutes, p=0.01), the operation times per fusion level were not (conventional LF : 72.3 vs. PFL : 90.2 minutes, p=0.08). EBL (p=0.28), LOS (p=0.99), and non-pathologic fever (p=0.34) were not different between the groups. Wound infection occurred in five patients in the conventional LF group and did not occur in the PFL group (p=0.58). Seroma, identified in MRIs, occurred in six patients in the conventional LF group and in one patient in the PFL group (p=1.00) (Fig. 10). C5 palsy occurred in one patient in each group (p=0.39). Screw fracture occurred in one patient in the conventional LF group and did not occur in the PFL group (p=1.00). Restenosis due to postoperative cervical trauma occurred in one patient in the PFL group and did not occur in the conventional LF group (p=0.22). The mean durations of postoperative follow-up were different between the groups (conventional LF : 35.2 vs. PFL : 20.0 months, p=0.01).
DISCUSSION
Various surgical methods have been developed for cervical spinal diseases. LF is one of the most recent procedures introduced for cervical disorders. It provides better long-term stability than laminectomy alone by inducing arthrodesis, and has a wider surgical indication than laminoplasty, allowing the reduction of kyphosis to lordosis [1].However, postoperative neck pain, kyphosis, pseudoarthrosis, pseudomembrane formation are considered drawbacks for this procedure [7,9,12]. We hypothesized that the posterior column can be preserved after LF by restoring the posterior column, including the laminae, at the very site where it had been cut. There are several merits for this procedure.
First, weight bearing for the anterior and middle columns can be distributed to the posterior column by bony reconstruction and muscle attachment, thereby preventing postoperative kyphotic change. Although the incidence of postoperative kyphosis is lower in LF than in laminectomy alone, postoperative kyphosis is a demanding complication after both procedures [1,18]. In our study, the SL angle difference between the preoperative time and the last follow-up was -0.3┬░ for conventional LF and 4.7┬░ for PFL (p=0.04). The SL angle difference can be interpreted as the curvature maintenance capacity, which is related to postoperative kyphosis. By reattaching the posterior bony structures to their original sites, through the bone fusion of the floating lamina which was initially adhered to the paraspinal muscles, tendons, and upper and lower spinous processes, the progression of postoperative kyphosis can be mitigated. Since the posterior column dominantly supports the cervical load compared to the anterior vertebral body [20,23] and the large amount of laminectomy is the risk factor of the postoperative kyphosis [6,16], gutter bone fusion is believed to mandatory for the stabilization of the cervical alignment after the surgery.
Second, after bony structure reconstruction with gutter fusion, it is possible to physically protect the spinal cord from the back. Managing the empty space after laminectomy is an important but frequently overlooked issue. There was definite bony bridging at the gutter between the lateral mass and the lamina in our study in follow-up CT 1 year after the operation. Only after bone healing with gutter fusion did the complication risk at the empty space decrease.
Third, pseudomembrane formation can be prevented. Several reports have indicated that postlaminectomy pseudomembrane is a result of epidural hematoma or epidural scarring and a source of chronic inflammation and neurological deterioration [12,24]. After covering the bony cap of the spinal cord, pseudomembrane formation at the operation site is less likely.
Lastly, it is well known that dead space management is crucial for wounds. A major principle in managing the dead space is reducing the amount of space at the site through soft tissue reconstruction and bony support [8]. This is extremely important not only for traumatic injuries, but also for infectious diseases [5,17]. Dead space at the surgical site is considered to be related to hematoma or seroma formation, which increases the risk of bacterial growth [14]. Several methods, including suction drain, vacuum-assisted wound closure, myocutaneous flap, and antibiotic loaded bone cement, have been proved to reduce the postoperative dead space [14,19]. Postoperative seroma is also known to occur in cervical spine surgery [27,29]. Wound infection and seroma occurred less frequently in the PFL group than in the conventional LF group but no statistical significance was found in our study due to the small patient number of the PFL group. This result may be attributed to the greater decrease in dead space after the operation in the PFL group than in the conventional LF group due to the restoration of bony structures.
It is important to ensure that the re-attached laminae are completely fused with the adjacent bone. Restenosis due to postoperative cervical trauma occurred in one patient in the PFL group. This patient slipped down at the stairway in a month after the PFL and came to the clinic with arm and leg weakness. CT revealed that the restored laminae compressed the spinal cord. Emergent operation was performed, and the patient recovered to the previous normal neurologic status. This case highlights the significance of the bone fusion achievement after surgery since the bone fusion is essential not only for the stabilizing the alignment but also for the prevention of restenosis, especially after the PFL surgery. It is generally believed that it takes at least 6 months for complete bone fusion [21]. Therefore, to obtain satisfactory results after surgery, it is necessary to be careful during the postoperative follow-up period.
Our study does have several limitations. First, since this study is a retrospective comparative study, randomized distribution to the conventional LF group and the PFL group was not possible. Second, the number of patients in the PFL group was relatively small compared to the number in the conventional LF group. Third, the follow-up period for the PFL group was shorter than that for the conventional LF group and was short overall. Long term follow-up for both groups is needed. PFL surgery has only been performed for a short period at our institute. In the next report, it will be possible to compare the two groups with similar follow-up and number of patients.
CONCLUSION
PFL was found to be safe and to achieve good results for cervical disorders. Our study showed that PFL achieves excellent alignment preservation as well as lower complication rates compared to conventional LF. Additionally, PFL demonstrated satisfactory improvements in several functional outcomes, specifically mJOA, NDI, VAS-N, and VAS-A scores. However, because of the aforementioned limitations, we could not draw a strong conclusion that PFL is superior to conventional LF. More number of the PFL patients are needed to make strong conclusions. Further randomized controlled trials comparing the conventional LF and PFL for cervical diseases should be performed to reach a more obvious conclusion.