INTRODUCTION
Spontaneous sphenoidal encephaloceles are uncommon entities and the presence of lateral sphenoidal encephalocele is a rare congenital anomaly3). Sternberg's canal is a lateral craniopharyngeal canal resulting from incomplete fusion of different sphenoid bone components5).
Congenital skull base abnormalities are believed to be the result of incomplete or premature fusion of the normal bony elements involved in the complex process of central skull base ossification. Due to their rarity, these lesions are seldom discussed in the medical literature and, to date, only isolated reports and small series are found4). The persistence of these abnormalities is often associated with cerebrospinal fluid (CSF) leak and encephaloceles8).
The efficacy and safety of the trans-sphenoidal approach for the resection of pituitary tumours and the treatment of associated CSF rhinorrhea has encouraged surgeons to use the transnasal route for the repair of all CSF leaks in the middle cranial fossa and sphenoidal sinus region1,7,10).
In the present case, we report the effectiveness of surgical treatment of a persistent Sternberg's canal by an endoscope-assisted trans-sphenoidal approach.
CASE REPORT
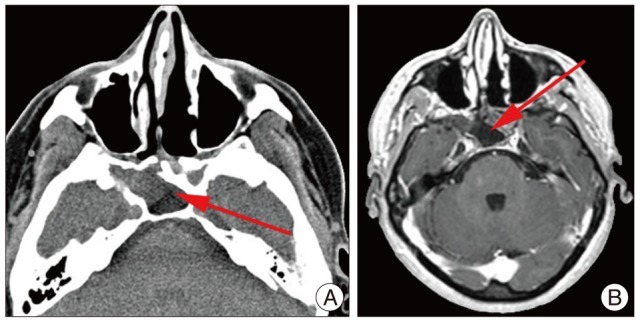
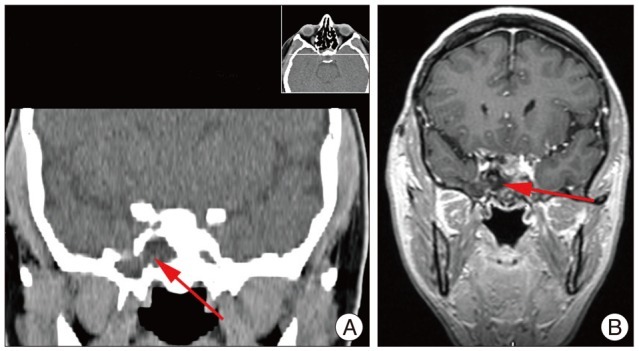
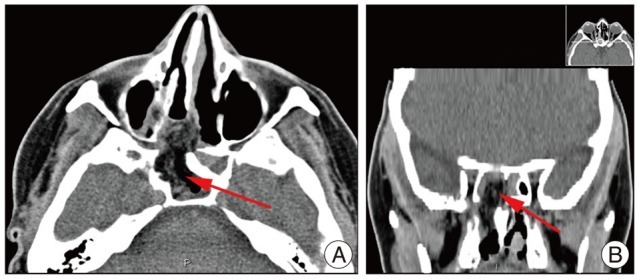
A 45-year-old female presented with complaints of intermittent right-sided watery nasal discharge for one year, without headache, nausea or fever. The symptom was worsened by clinostatic position : during the night, the patient referred watering fluid in the pharynx. This was accompanied by confusion sensation and, sometimes, positional headache. There was no history of meningitis or trauma. β2-Transferrin-analysis and albumin/prealbumin tests of the nasal discharge indicated cerebrospinal fluid. The high resolution computed tomography of facial massix scans, including coronal reconstructions, revealed a particularly extended sphenoidal sinus on the right side (Fig. 1A, 2A). Magnetic resonance imaging with contrast medium demonstrated peripheral enhancement of the lesion. We diagnosed the lesion as sphenoidal encephalocele (Fig. 1B, 2B).
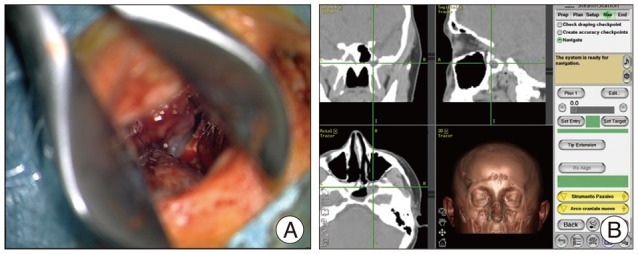
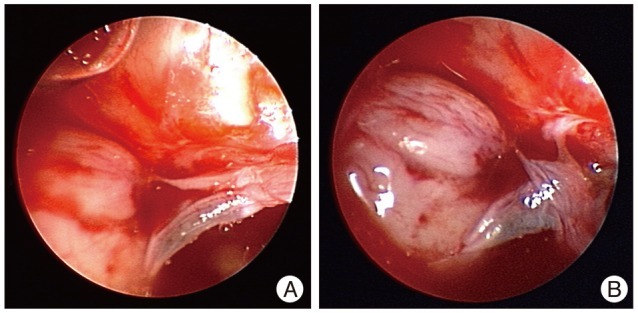
We decided to approach the lesion by an endoscope-assisted trans-sphenoidal approach, supported by neuronavigation, and the parasellar bony defect was confirmed (Fig. 3). The right temporal lobe pole was herniated into the accessory sphenoidal cell. Furthermore, the endoscope-assisted observation permitted to individuate cerebrospinal liquor outflow, under brain pulsation (Fig. 4).
The herniated brain material was removed under endoscopic control, until the individuation the bone defect on anterior wall of accessory cell. After abdominally fat and muscle graft by a right paraombelical incision, under intraoperative microscopic control, a sphenoidal accessory cell duraplasty was accomplished by inserting grafts of abdominal fat into the "bottleneck" of the meningocele. With the aid of neuronavigation, reduction of the right sphenoidal encephalocele was obtained and the persistent canal was sealed with the aid of fat, muscle graft and fibrin glue.
The nasal discharge stopped immediately after surgery and postoperative computed tomography demonstrated the complete reconstruction by a duraplasty (Fig. 5).
Three years later the patient had no evidence of cerebrospinal fluid leakage.
DISCUSSION
Spontaneous CSF leaks have been estimated an infrequent entity, but recently this idea has changed9)). Skull base malformations and obesity are considered risk factors for their development6). An overpneumatized sphenoid sinus, especially in its lateral wall, is often a site where a CSF leak may emerge13). This pneumatization might contribute to weakening of the sphenoid roof. In fact, pit holes in the floor of the middle cranial fossa have been indicated as causes of encephaloceles, especially when associated with large pneumatization. In the presence of sufficient pneumatization, Sternberg's canal may act as the site of origin of congenital meningoceles or CSF fistulas12). Furthermore, normal spikes of CSF pressure, and evidently hydrocephalus, may facilitate the development of small holes with herniation of the dura/arachnoid or brain tissue13).
The treatment of spontaneous sphenoidal CSF fistulae has historically involved both extra- and intracranial approaches. The extracranial approaches are desirable from a noninvasive standpoint; however, they fail to provide control of possible lateral extension of the sphenoidal sinus, where several of these fistulae arise8).
The transnasal approaches to the sphenoid sinus have been proven to be safe and effective in the treatment of CSF rhinorrhea associated with post-trans-sphenoidal pituitary surgery, postoperative anterior cranial fossa cranial base surgery, and even medial intrasphenoidal and sellar encephalocele1,6).
The endoscope-assisted observation provided the treatment of sellar and parasellar lesions, although pure endoscopic trans-sphenoidal approach have been proposed for this purpose2,4,11,14).
Surgeons performing endoscope-assisted microneurosurgical procedures have to see through an operative microscope during specific microsurgical approach. The visualization of the same structures as seen through a different tool, also considering that scope with a different viewing angle provides quite different vision.
During microsurgical procedures, the operative microscope provides direct illumination and magnification of the operative field. However it allows detailed view only of superficially located structures requires manipulation and retraction of intact superficial anatomical sectors, which unavoidably results in iatrogenic traumatism. This may be obviated combining microsurgical techniques to the use of the endoscope, which allows atraumatic vision of the structures located beyond and behind the superficial structures "around the corner".
Endoscope-assisted management is technically challenging, nevertheless its advantages are a good view of the surgical field while being less traumatic than pure trans-sphenoidal or transcranial approaches.
CONCLUSION
Spontaneous sphenoidal encephaloceles are rare entities often associated with a persistent Sternberg's canal. A case of middle cranial fossa spontaneous CSF fistulae, involving a temporal encephalocele through lateral excision of this sinus, has been presented.
Our experience shows how the endoscope assisted trans-sphenoidal approach allows a wide, safe, and direct route to the lateral recess of the sphenoid sinus. Compared with traditional transcranial routes, this approach provides a good exposure of the bony defect with minor morbidity and considerable advantages.