INTRODUCTION
Fabry's disease is an X-linked lysosomal storage disorder caused by mutation of the gene that encodes an enzyme alpha-galactosidase A, a mutation inducing accumulation of glycosphingolipids in lysosome, especially in vascular endothelial and smooth-muscle cells1-17). Patients with the disease commonly have a cerebral vasculopathy causing premature ischemic stroke, usually in the vertebrobasilar circulation. Its prevalence was reported to be high as 4.9% in men and 2.4% in women15), but hemorrhagic stroke especially in middle-aged patients with Fabry's disease is sufficiently rare13). We report an unusual case of cerebral aneurysmal rupture resulting in a subarachnoid hemorrage (SAH) with Fabry's disease.
CASE REPORT
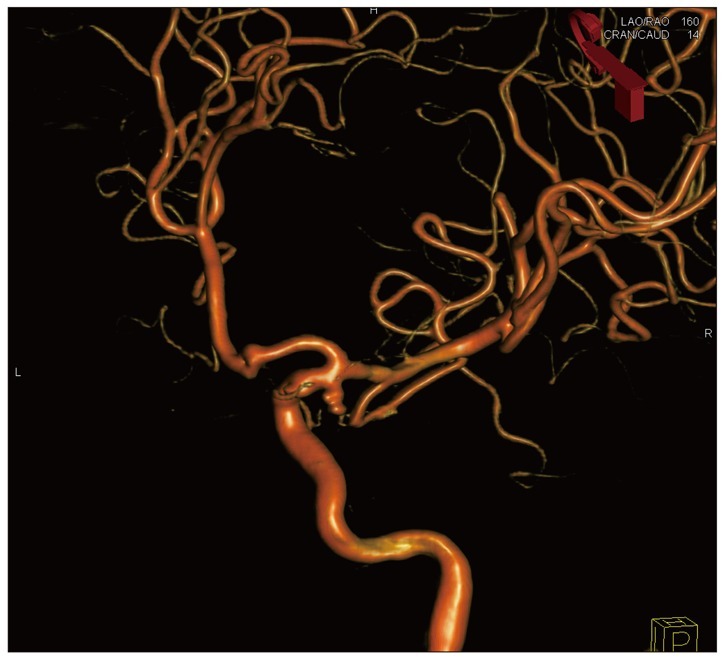
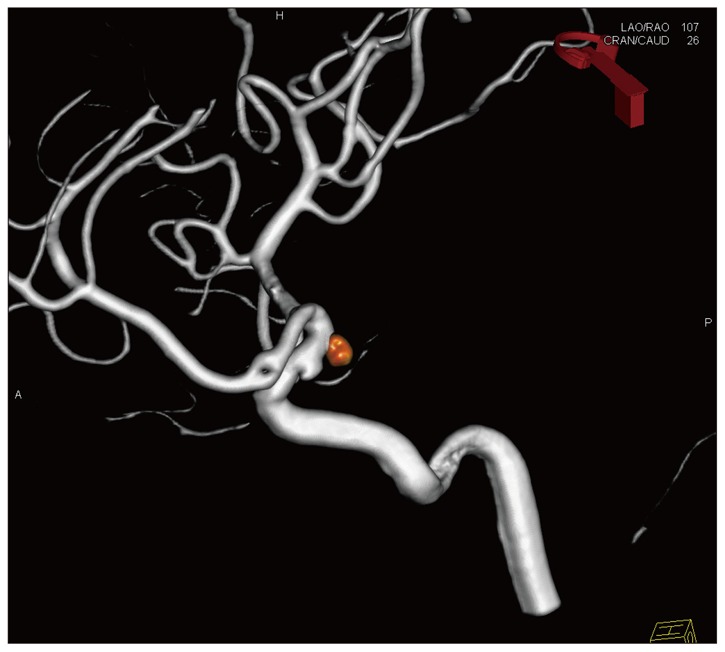
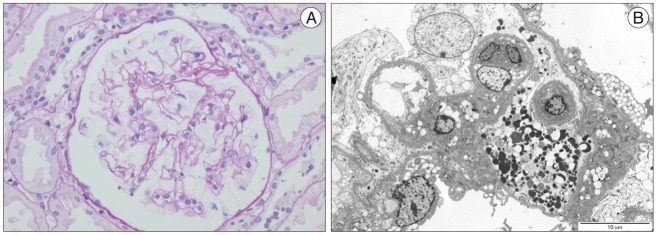
A 42-year-old woman, who had no previous medical history experienced the sudden onset of severe headache and followed by loss of consciousness. A computed tomography revealed that subarachnoid hemorrhage was located in the basal cistern. Cerebral angiography on the day of admission demonstrated a saccular aneurysm of the right posterior communicating artery (Fig. 1). The aneurysm was treated by an endovascular coil embolization (Fig. 2). Postoperative computed tomography revealed the resolved subarachnoid hemorrhage without posthemorrhagic hydrocephalus and infarction. The patient recovered favorably without any neurological deficit. During her admission, she showed proteinuria in urine analysis. In kidney needle biopsy, the pathologic findings implied nephrosialidosis (mucolipidosis of lysosomal stroage disease) consistent of Fabry's disease (Fig. 3). The patient was transferred to the department of nephrology, where she was treated with a gene therapy and medical management. The patient recovered favorably, discharged without any neurological residual symptom.
DISCUSSION
Estimates on the prevalence of classic Fabry's disease are varied from 1 in 40000 to 1 in 1170011), a variation that indicates the patients are frequently misdiagnosed and spend years or even decades receiving inappropriate treatment. A study of 721 patients with cryptogenic stroke, aged 18-55 years, showed a high prevalence of Fabry's disease : 5% (21/432) of men and 3% (7/289) of women15). In a Belgian Fabry study to investigate prevalence of Fabry's disease, 49 patients (4.9%) were found to have intracranial hemorrhage in a cohort of 1000 young patients with cerebrovascular disease. Meanwhile, 16 patients with intracranial cerebral hemorrhage had a SAH4), and 15 were found to have cerebral aneurysm in the same study but they were not associated with aneurysmal rupture as SAH4,15). The frequency of stroke in men aged 25-44 years can be up to 12 times more frequent than that is expected in the general population while women can have nearly 10 times higher prevalence of stroke when compared to normal women older than 18 years. Renal and cardiac diseases are more frequently seen in patients with cerebrovascular disease17).
Because Fabry's disease is an X-linked disorder, female patients are regarded as carriers of mild feature of the disease at worst, but there are researches showing a high frequency of cerebrovascular events in woman. Such findings may imply that cerebrovascular involvement at least in a subgroup of clinically affected female patients could be as severe as in hemizygous male patients9). Male hemizygotes with this disease are generally more severely affected than heterozygote females, but disabling clinical features and disease progression are what female patients often undergo6,10). Meanwhile, ischemic strokes with no specific cause are judged to be cryptogenic one, which is more common in younger rather than older patients. Thus, Fabry's disease should be considered in all cases of unexplained stroke in younger patients, especially in cases with combination of cerebral stoke in the vertebrobasilar artery system and proteinuria15,17).
Although the mechanism linking glycolipid accumulation to cerebral stroke in Fabry's disease has been poorly understood, cerebral microangiopathy may be a hallmark of the disease, implying that lipid deposit in the vascular endothelial and the smooth muscle cells cause oxidative stress, vascular dysfunction, vessel occlusion, and tissue ischemia2,8,9). These pathological mechanisms are associated with increased risk of premature strokes, progressive white matter lesions, and dolichoectasia. Cerebral stroke frequently occurs before Fabry's disease is diagnosed and other key signs of the disease are found12,16,17).
As for Fabry's disease, ischemic stroke occurs more frequently than hemorrhagic stroke and can be a consequence of cardiac embolism or cerebral vasculopathy. Sims et al.16) reported that most patients of the disease had ischemic stroke (105 of 121, 86.8%) and 13 of 77 males (16.9%) and 3 of 44 female (6.9%) experienced hemorrhagic stroke, for which specific stroke type was not described. Hemorrhagic stroke can be a consequence of hypertension secondary to chronic renal failure or weakening of vessel walls due to lipid deposition. Meanwhile, none of the patients exhibited intracranial hemorrhage within the vertebrobasilar region3,8,9,16). Reisin et al.14) reported that 44.4% (16 of 46) adult patients without clinical history of cerebral stroke or prior dialysis had a evidence of small vessel disease and 11% (5 of 46) showed cerebral micro-bleeding on magnetic resonance image5).
CONCLUSION
Fabry's disease is uncommon but requires clinical concern. The disease is frequently associated with ischemic strokes, but hemorrhagic strokes such as an aneurysmal rupture to be SAH is rare, especially in middle-aged patients. Further investigation is needed to reveal risk factors, vascular anatomy, and causative mechanisms. In addition, studies with larger cohorts of high-risk patients may help to formulate definite answers for the disease.