INTRODUCTION
Due to the recent development of technology and various devices, electrical and electronic equipment use in the operating room is growing. Increased use of electrical and electronic equipments may cause a greater risk of burns to operating room workers as well as patients despite the use of improved safety devices.
There are some reports about burns that occurred directly to patients, which were caused by use of electrical operating appliances such as electrocautery or laser equipment during surgery. However, it is hard to find reports about the occurrence of burns upon the electrocautery after disinfecting the surgical site with alcohol in Korea. Reports about the incident of burns related to neurological surgery are hardly found as well. Furthermore, investigations and statistics about incidents of burns in operating room are not even known. In the U.S., Food and Drug Administration has conducted research and statistics about fire in the operating room. There are more than 100 incidents of fires occurring in the operating room every year and 10% to 20% caused serious damage. As a result, it caused the death of two patients on average1,2,10,11).
Fires in the operating room can be prevented. Otherwise, it could do serious damages to medical staffs and patients that could arouse economic and legal issues to the hospital. Therefore, all medical staffs should always be aware of the possibility of the fire hazard.
This case is reported as an incident of burns that occurred to a patient upon electrocautery after disinfecting the site for surgery with alcohol during the preparation for neurosurgery in the operating room where exposed to oxygen.
CASE REPORT
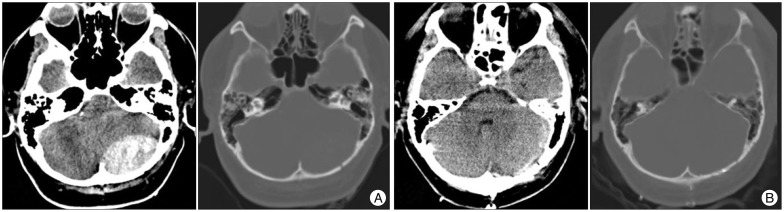
After a 33-year-old male patient who was in an advanced state of inebriation, was admitted to the emergency room after falling down stairs and losing his consciousness. Since an epidural hematoma on his occipital lesion was detected on a brain CT scan, urgent craniotomy and hematoma evacuation should be carried out immediately (Fig. 1). Patient's hair was shaved for surgery, and his head was fixed in his prone position using a Sugita head holder (Mizuho Ikakogyo, Tokyo, Japan). Then the surgical site was disinfected using 75% alcohol. The patient had a deep laceration of about 10 cm and his occipital bone was exposed before the surgery. He also had experienced heavy bleeding in the superficial arteries on the scalp. At the moment a monopolar electrocautery was ready to be used in order to stop the bleeding. All of a sudden, a spark was set off on residual alcohol vapor and the surgical site as well as surgical drape caught flame in the fire. After the fire was extinguished immediately using saline, the surgical drape was removed.
The patient suffered the second-degree burns on his cheeks, forehead and about 40% of the scalp (Fig. 2). First, the patient underwent a craniotomy and removal of hematoma. The patient woke up with a clean state after the surgery. Then, he received treatments from plastic surgery and he recovered without any other surgical treatments. However, a cosmetic issue was generated due to discoloration on facial area.
DISCUSSION
Status of fire in operating room
Although fires in operating room are rare, patients, medical staffs and surgical instruments can be serious damaged upon the occurrence of fire. And even casualties in most severe cases.
Actual reports about fires in operating rooms have not been published yet according to statistical data in Korea, even though the possibility of fire accidents in operating rooms still exists. In fact, according to the U.S. Emergency Care Research Institute, more than 100 incidents of fire occurs in operating rooms every year and the most common causes for ignition include electrical surgical factors (68%), electrocautery (19%) and laser (13%), respectively. The most common burned areas include respiratory tract during anesthesia (34%), face, head, neck and chest in order1,2,3,10,11).
The cause of incident of fire upon surgery
First, regarding the fuel as a factor that causes fire in surgery, 7.5% povidone iodine was used after the practice of using of 70% alcohol as a disinfecting solution for the surgical site before neurosurgery. In 2007, Chung et al.9) claimed that the alcohol-containing antiseptic was the biggest factor to cause fires in the operating room, and drapes should be conducted after the antiseptic dried out in order to prevent fire in the operating room. In 2005, Metlzer et al.14) claimed that alcohol-containing antiseptic should be applied enough, but thinly, to be able to dry out in order to prevent the fire in the operating room. There is much remaining alcohol in folded drape areas (Fig. 3). Therefore, folding drapes should be avoided as much as possible in order to evaporate alcohol easily. Briscoe et al.6) examined the function of flammable antiseptic upon the fire in the operating room and reported that 70% of alcohol-containing antiseptic (mainly chlorhexidine) ignited at 90℃. However, it even ignited at lower temperatures such as 30℃ to 70℃ in 100% oxygen supplied environment. These temperatures can be reached easily by using typical electrocautery. In addition, the ignition temperatures on drape, sterilized paper, towels and cotton mesh were investigated and the temperature ranged between 730℃ to 770℃. With oxygen and nitrous oxide, the ignition temperature would fall below 500℃. In recent years, many hospitals have replaced fabric with disposable cloth for surgical drapes. The disposable surgical cloth has many advantages as follows: it is less expensive than fabric and has waterproof property that is treated with a fire resistant material like lint. Additionally, this chemically treated disposable cloth can delay the fire from being started. But it will be burned out quickly once the fire starts. Hence caution is strongly still needed. In case of this patient, fire was caused due to the use of electrocautery before the alcohol solution had evaporated sufficiently. This demonstrates that alcohol solution was the cause for the fire.
Second, there are some other factors that can cause ignition in the neurological surgery operating room such as flames, heat sources, sparks from electrical circuits and static sparks. Various kinds of surgical instruments such as laser or electrocautery can cause the ignition13,17,18). In addition, there has been a report about occurrence of a third degree burn on the site where nerve monitoring devices were attached during the surgery15). Therefore, it is absolutely necessary for surgeons to be extra cautious.
Third, 100% of oxygen is used in the neurological surgery operating room under general anesthesia. In 2001, Barker et al.4) confirmed that the concentration of oxygen rose around the head and neck during anesthesia, and oxygen was especially accumulated within drapes, increasing the risks of fire in the head and neck upon the use of 100% oxygen through mannequins experiment. In order to prevent such accidents, people have to make sure that the oxygen does not leak around the endotracheal intubation and do not create the dead space upon drape to prevent the oxygen from stagnating on the head and neck.
Finally, the biggest cause of fires in the operating room is the lack of awareness of medical staffs about fire. Meltzer et al.14) insisted that everyone in the operating room should be aware of the possibility of fire on antiseptic. In 2008, American Society of Anesthesiologists pointed out that education, preparation of fire extinguisher goods in the operating room, handling protocols and policy, and communication between surgical staffs are the key for fire prevention in the operating room3,7,8,16).
Points for improvements
Causes of fires in the operating room can be summarized into four categories: 1) Alcohol solution for antiseptic was not dried sufficiently. 2) Alcohol on drape was not dried enough because they were folded prior to surgeries. 3) People in the operating room were not aware of risk of fire on alcohol for antiseptic, and fire extinguisher goods have not been equipped in the operating room. 4) Proper hemostasis was not present at the bleeding focus.
Therefore, we have to follow alternatives and safety rules, to prevent the similar situations, as follows: 1) Doctors can use disinfecting solutions on the skin before the surgery as long as they don't contain alcohol (e.g. povidone iodine solution, chlorhexidine gluconate). 2) Drapes should not be folded to prevent the antiseptic from stagnating on the site upon the use of antiseptic containing alcohol, and the surgery should be carried out after the antiseptic has dried completely. 3) All the medical staffs in the operating room should be aware of risks of fire of alcohol as well as electrocautery. 4) Fire extinguisher goods must be equipped in the operating room. When the patient is the fuel source, a CO2 extinguisher (effective on electrical fires and flammable liquids) would be preferable because of its lack of ammonium phosphate, in which reduces the level of contamination and tissue damage12). 5) Appropriate method to stanch the blood should be selected before disinfecting the skin, through sutures and pressure upon massive arterial bleeding.
CONCLUSION
This report explored the risks of fires upon use of electrocautery after sterilization with alcohol which can cause a fire in the operating room full of oxygen. We always have to be aware and be careful about the possibility of a fire by following safety rules to minimize hazardous accident occurrence.