INTRODUCTION
Neurenteric cysts are rare benign, congenital, malformative endodermal lesions in the central nervous system (CNS)2,4,21). Solitary neurenteric cysts of the upper cervical spine are very rare. Intraspinal neurenteric cysts are usually located in the cervical and thoracic regions9,13,31), and most of the cysts are ventrally located at the intradural and extramedullary compartment of the spinal cord4,12,16,26). Neurenteric cysts commonly manifest during the second and third decades of life1,17,29), and surgical excision by a posterior approach is the most preferred treatment13,31). We report a case of cervical intradural extramedullary neurenteric cyst without other associated malformation, which was treated via a posterior approach. We present clinical, radiological and surgical characteristics of the neurenteric cyst and discuss them with reference to the literature.
CASE REPORT
A 15-year-old boy presented with a 2-month history of progressive neck and both shoulders pain which was not responding to medical treatment. There was no history of trauma, and his neurologic examination at the time of admission was fully normal. Motor strength and sensation of all extremities were intact, and any long tract sign was not detected.
Laboratory findings of the blood and the urine were within normal limits. Electrodiagnostic examinations were performed, and abnormal finding was not checked on the nerve conduction studies and needle electromyography. But the bilateral posterotibial and the left median somatosensory pathway dysfunction was confirmed on somatosensory evoked potential (SSEP) test.
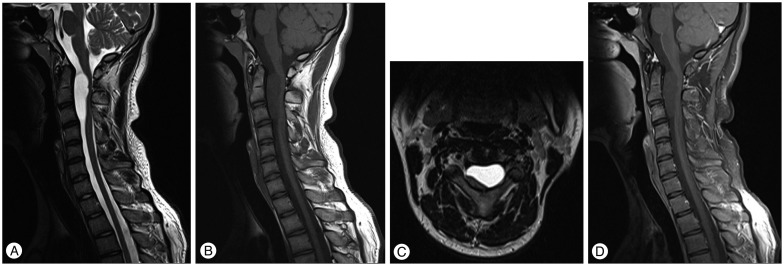
He underwent radiological evaluations with cervical X-rays, magnetic resonance (MR) imaging and computed tomography (CT). MR images of the cervical spines revealed well-delineated lobulated mass, measuring about 2.7×1.6×4.8 cm, and the cystic mass was an intradural extramedullary lesion located ventrally to the cord, extending from the C1 to the C3 level (Fig. 1). The adjacent cervical spinal cord was displaced dorsolaterally and was prominently flattened by the lesion, but the signal change of the spinal cord was not definite. The C1-3 vertebral columns were slightly displaced forward by the mass. The cyst showed markedly low signal intensity on T1-weighted MR images (T1WI) and high signal intensity on T2-weighted images (T2WI). And the cyst was isointense with cerebrospinal fluid (CSF) on both T1WI and T2WI. The lesion was not enhanced after the administration of gadolinium contrast material. The bony structures and the soft tissues were normal. Cervical CT scan was performed for further evaluation of the bony structures and the soft tissues, but we could not find any definite abnormal findings.
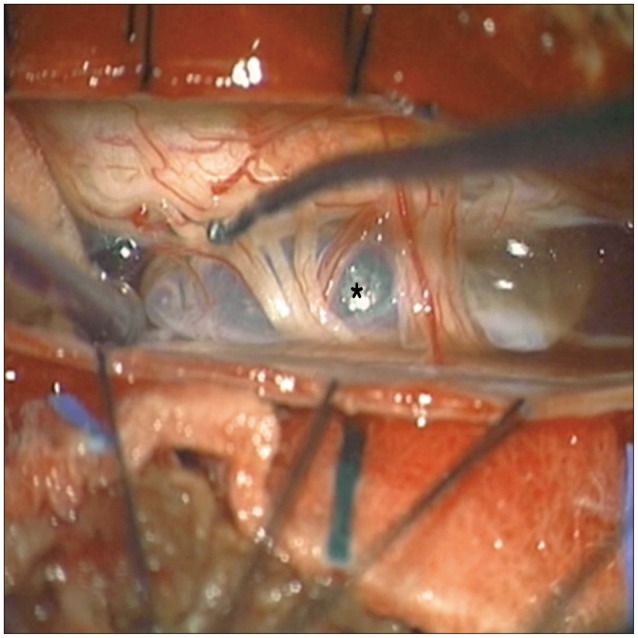
We planned surgical treatment via a posterior route, and then hemilaminectomy was performed for the C1, C2, and C3 vertebrae. Bone and soft tissues were found to be normal. After the dura was opened, the thin-walled cyst was noted anterior to the cord (Fig. 2). The cyst could be completely excised with preservation of the surrounding neurovascular structures, since the mass had not adhered to the surrounding structures except for the attachment to the arachnoid membrane and the denticulate ligaments. Sticky fluid was aspirated from the cyst. All the procedures were performed under intraoperative SSEP and motor evoked potential monitoring. There was no abnormal finding on the intraoperative monitoring.
Histopathology of the excised cyst showed a ciliated pseudostratified columnar epithelium containing mucinous contents (Fig. 3). There was no neural, glial or ependymal cell in the cyst wall. According to the pathologic result, the final diagnosis was neurenteric cyst.
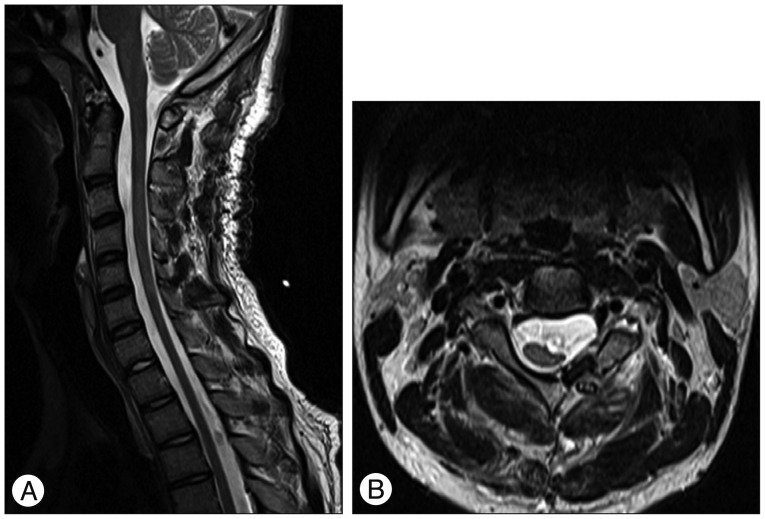
The patient's postoperative course was uneventful. The pain showed significant improvement immediately after the operation. Postoperative neurological function was normal and the patient suffered no recurrence during the 10-month follow-up period. On the postoperative MR imaging, there was no residual lesion and the compressed spinal cord was significantly expanded (Fig. 4).
DISCUSSION
Neurenteric cysts are rare congenital cysts of the CNS. First described by Puusepp24) in 1934, neurenteric cysts have had several names, including enterogenous cyst, enteric cyst, endodermal cyst, gastroenterogenous cyst, gastrocytoma, intestinoma, and archenteric cyst4,9,11,13). Saunders first introduced the term 'Neurenteric cyst'28) which has been accepted currently in the literature.
Although the pathogenesis still remains unclear, neurenteric cysts are generally thought to result from failure of separation of neuroectodermal and endodermal elements during week 3 of embryogenesis3,15,32). Notochord and foregut fail to separate, causing primitive endodermal cells to be incorporated into the notochord, and these displaced alimentary cells ultimately become the cyst11,20,21).
Most reported neurenteric cysts occur in the spine, usually ventral to the spinal cord11,25,28). Intraspinal neurenteric cysts are commonly located in the cervical and thoracic region, and in rare cases they are found at the craniovertebral junction, lumbar and sacral regions9,13,31). Most of these cysts are located in intradural extramedullary compartment of the spinal canal, and fewer than 5% of them are situated in the intramedullary compartment2,4,12,16,17,25). They account for 0.7% to 1.3% of all spinal cord tumors5,17,23,26,29). Intraspinal neurenteric cysts usually manifest during the second and third decades of life1,5,17,29), and they are 1.5 to 3 times more common in males1,8,23,25,26). The patient in our case was also within these scopes mentioned above.
Intraspinal neurenteric cysts may occur as an isolated spinal cyst or in concomitant with other congenital anomalies18). In about 50% of cases, spinal neurenteric cysts are accompanied with vertebral anomalies such as Klippel-Feil deformity, vertebral defects and spondylolisthesis, and besides the association with other congenital malformations such as intramedullary epidermoid cyst, meningomyelocele, syringomyelia, diastematomyelia and spinal lipoma have been noted6,20,30). In the present case, any vertebral anomaly nor congenital malformation was not identified on the preoperative radiologic evaluations and the intraoperative findings.
Wilkens and Odom32) classified neurenteric cysts into three types based on histological features : type A, simple or pseudostratified, cuboidal or columnar epithelium with or without cilia lying on a basement membrane; type B, similar to type A with addition of mucous glands, serous glands, smooth muscle, fat, cartilage, bone, elastic fibres, lymphoid tissue or nerve ganglion; type C, similar to type B with addition of ependymal or glial tissue. According to this classification, the histopathological result of our case belongs to type A.
Most presenting symptoms of neurenteric cyst are related to the compression of adjacent spinal cord by the lesion22) or the inflammatory reactions to the cyst contents15). Pain is the most frequent symptom of spinal neurenteric cysts, and the pain can either be local (54%) or radicular (31%)22). Other rare presentations include aseptic meningitis, bacterial meningitis, chronic pyrexia, and paraplegia5,10,16).
In some cases, the clinical course is characterized by fluctuation of symptoms, which may be related to intermittent ruptures of the cyst or to alterations in the rates of mucin production and reabsorption by the cyst wall17,25).
Neurological signs of patients with solitary neurenteric cyst are occasionally insidious or even absent, despite the severe compression of the spinal cord6,26). For this reason, diagnostic evaluation for these patients is often delayed until they have suffered from motor weakness or other signs of myelopathy26).
Radiographic studies include plain spine radiographs, CT scans, and MR imaging scans19). MR imaging is the essential diagnostic modality. Almost all of neurenteric cysts are hypointense on T1WI and hyperintense to isointense on T2WI6,10). Typically the cysts rarely show rim enhancement by contrast medium4,21,27). The cyst fluid on MRI scans may appear isointense to hyperintense compared with the CSF on both the T1WI and T2WI, and these various signal patterns are thought to correlate with different protein content of the cyst fluid or hemorrhage within the cyst4,5,10,14). MR imaging can directly visualize the morphology of the lesion and any associated cord change, whereas the associated bony abnormalities are better delineated on a CT5,29).
The differential diagnosis of intraspinal cystic lesions includes arachnoid cyst, dermoid cyst, epidermoid cyst, teratoma, parasitic cyst, ependymal cyst, cystic cord tumors, and masses with associated syrinx and myelomalacia5,8,27). Definitive preoperative diagnosis of neurenteric cyst has seldom been possible, and the final diagnosis should be established by histopathological examination8,26).
The treatment of choice for intraspinal neurenteric cysts is complete surgical excision. Nevertheless, the complete resection is not always possible, and only 36% of the cysts were totally removed among cases reported in the review by Paleologos et al.22). It is usually either because of the ventral location to cord or because of the adherence of a part of the cyst to the medullary substance5,22). When the cysts are located in the extramedullary compartment with a clear plane of dissection between the lesion and the neural elements, complete resection can be achieved5,17,26).
Although some authors have reported conservative treatments such as cyst aspiration with or without cyst marsupialization and cystosubarachnoid shunting, especially in the cases of intramedullary cyst, the current authors do not recommend simple aspiration because of the significant risk of delayed recurrence and of postoperative aseptic meningitis due to fluid content of the cyst5,17,22,26).
Various surgical approaches have been described depending upon the level and the location of the lesion. Several surgeons have reported an anterior approach for the removal of a cervical neurenteric cyst2,7,10,29,30), but the anterior approach is more extensive procedure requiring subsequent fusion. A posterior approach that resect a ventral intradural lesion is not always easy, especially if the lesion is situated in the upper cervical spine. It is also important to identify the vascular anatomy of ventrally located lesions because the posterior approach may compromise the abnormal vasculature19). Nevertheless, the posterior approach have been preferred by many authors because the procedures are relatively straightforward and have an advantage of working space during the removal of the cyst3,13,26,31). In our case, although the lesion was extending along the upper cervical spine (C1 to C3), the cyst was successfully removed via posterior route.
Recurrence has rarely been reported in the literature. Prognosis generally appears better when the patients do have those below : no abrupt clinical course, no severe neurological deficit before diagnosis, no atrophic change of spinal cord on MRI, and when total removal of the cyst is achieved (58.6% complete recovery versus 27.9% for partial excision)22).
CONCLUSION
Intraspinal neurenteric cysts are rare developmental lesions in the adolescent. Moreover, solitary neurenteric cysts occurred in the cervical spinal canal are extremely rare. However, the neurenteric cyst should be included in the differential diagnosis of an intradural cystic mass, even if there is no evidence of associated vertebral or visceral abnormalities. Generally, the diagnosis of these lesions can be delayed or be omitted, especially if a patient present only with persistent neck pain and not having neurological deficits. We reported a rare case of solitary intraspinal neurenteric cyst which was located ventrally to the cord at the high cervical level and was confirmed as a neurenteric cyst through the pathological diagnosis.