INTRODUCTION
Mucosa-associated lymphoid tissue (MALT) lymphoma is one of the most common lymphomas and accounts for about 7% of all newly diagnosed non-Hodgkin's lymphoma (NHL)4,8). The clinical course of MALT is relatively indolent and, in the majority of cases (50%), the lymphoma arises within the stomach4). Primary central nervous system lymphoma (PCNSL), an uncommon variant of extranodal NHL, can affect any part of the neuraxis, including the eyes, brain, leptomeninges, or spinal cord3). Herein, we present a rare case of PCNSL, which occurred one year after radiochemotherapy for gastric MALT lymphoma. We propose some possible mechanisms to explain this rare phenomenon and present a literature review.
CASE REPORT
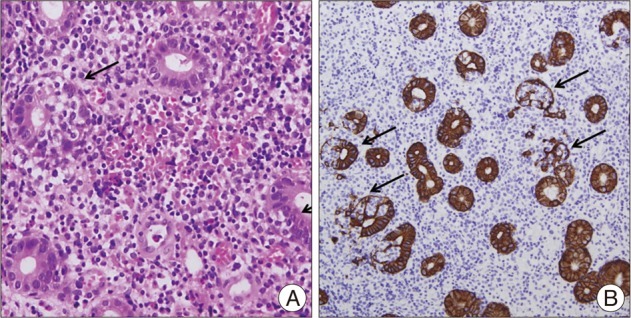
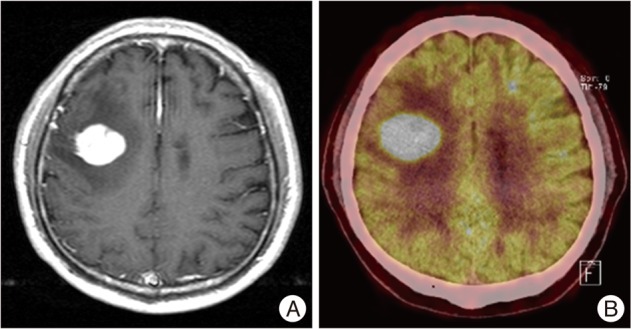
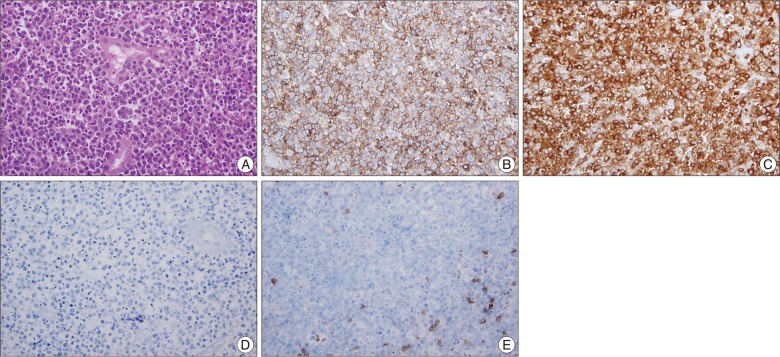
A 62-year-old man with a 3-day history of left facial palsy was admitted to our hospital. From the past medical history one year before he came to our department, he underwent antibiotic eradication therapy of Helicobacter pylori, 3600 cGy of local stomach fractional radiotherapy, and 6 cycles of chemotherapy using chlorambucil for gastric MALT lymphoma (Fig. 1). For 3 years, he has been taking medicines for diabetes, hypertension, and chronic obstructive pulmonary disease with asthma. One year ago, he was diagnosed as having chronic kidney disease (stage IV) due to diabetes. A cranial magnetic resonance (MR) image revealed a 3.3Г—3.5-cm round mass in the right frontal lobe. This mass was hypointense on the T1-weighted image and isointense on the T2-weighted image and showed peritumoral edema. Moreover, administration of a contrast agent revealed strong homogeneous enhancement (Fig. 2A). A whole body positron emission tomography-computed tomography scan revealed no evidence of hypermetabolic malignancy, except highly increased fludeoxyglucose uptake in the mass in the right frontal lobe (Fig. 2B). We performed the excisional biopsy of solitary mass that located non-eloquent area because we could not rule out the possibility of the malignant intra-axial tumor. The histological diagnosis of PCNSL from diffuse large B-cell lymphoma (DLBL) was made (Fig. 3). The patient had no postoperative complications and was transferred to the Department of Hemato-oncology for chemotherapy with high-dose methotrexate and cytosine arabinoside. Thereafter, the patient's condition deteriorated, and he died of pneumonia 3 months after the operation.
DISCUSSION
MALT is acquired through chronic inflammation/antigenic stimulation in organs that are normally devoid of lymphoid tissue2,4). The discovery of a common mucosal immune system linking anatomically separate compartments of MALT has shown that lymphocytes involved in MALT leave the mucosa following antigenic stimulation and preferentially circulate back to MALT organs by interacting with a receptor/ligand system involving high endothelial venules2,4,8). In the case of gastric MALT lymphoma, Helicobacter pylori appears to play a key role in not only the development of MALT but also the consecutive lymphomatous transformation2,8).
Aria et al.1) reported a case similar to our case. In 2009, they reported the case of a 53-year-old man in whom CNS metastasis from gastric MALT lymphoma was noted for the first time. However, we think that there were some discrepancies in their case report. MALT lymphoma is characterized by a mass predominantly consisting of small cells4). Transformed centroblast- or immunoblast-like cells may be present in variable numbers in MALT lymphoma; however, when solid or sheet-like proliferations of transformed cells are noted, the tumor should be diagnosed as DLBL and the presence of accompanying MALT lymphoma noted4). The term high-grade MALT lymphoma should also not be used; moreover, a large B-cell lymphoma arising at a MALT site or being associated with lymphoepithelial lesions should not be considered a MALT lymphoma4). Aria et al.1) diagnosed their patient as having gastric MALT lymphoma with a high-grade component. Subsequently, after 4 years, he was diagnosed as having DLBL in the left parietal lobe of the brain. They suggested that the histopathological findings, including lymphocytic subsets, were almost identical between the primary gastric MALT lymphoma and the secondary brain lymphoma. According to the WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 2008, the gastric tumor patient in the case reported by Aria et al.1) should have been diagnosed as having DLBL instead of gastric MALT lymphoma with a high-grade component4). Therefore, we feel that Aria et al.1) should change their diagnosis to CNS metastasis from DLBL of the stomach.
Histologically, a proportion of CNS lymphomas may be classified as a part of the MALT spectrum, which can range from small lymphocytic to plasmacytoid to marginal zone cell-type lymphomas6,7). Marginal zone B-cell lymphoma (MZBCL) was initially described by Isaacson and Wright as an indolent low-grade lymphoma in the MALT of the gastrointestinal tract5). A similar lymphoid infiltration was subsequently recognized in the mucosa of other organs, including the lung, bladder, salivary gland, conjunctiva, and lacrimal gland, as well as tissue sites such as the thyroid, breast, thymus, orbit, skin, liver, and CNS that do not have a mucosa4,7). When MALT lymphomas occur in the CNS, they are distinguishable from high-grade PCNSL. Unlike most CNS metastases of systemic lymphomas, CNS MALT lymphomas are localized and low-grade lesions7).
Elucidating the correlation between the first MALT lymphoma and the second PCNSL seems difficult; 3 possible pathogeneses have been postulated for the development of the second PCNSL. First, the MALT lymphoma and PCNSL developed independently at a distance of time. Although there was a relatively short interval between the development of the first and second tumors, the 2 tumors are distinct. In other words, we consider that the PCNSL was a second primary lesion. The second possibility is that there was a malignant transformation of the MALT lymphoma and then it metastasized to the brain. We cannot rule out the possibility of metastasis because the immunoprofiles of specimens obtained from the stomach and brain were the same. However, we carefully reexamined the previous gastric specimens and did not discover any components of DLBL in the gastric specimens. Third, although not proven, there is the possibility of coexistence of a MALT lymphoma and a high-grade lymphoma in the stomach. Initial gastric biopsy was underestimated to MALT lymphoma instead of DLBL. The findings of this report may be noteworthy when compared to those of previous reports. Neurosurgeons should pay attention to the pathological variety and dynamic pathological changes in lymphomas during examination and treatment of patients.