INTRODUCTION
Pediatric intracranial aneurysm is rare, reported as accounting 0.5-4.6% of total intracranial aneurysms [6,15]. Infantile intracranial aneurysms are much rare and have few different clinical characteristics compared to adults [3]. There was an aggressive case of 7-month-old patient with ruptured fusiform anterior cerebral artery (ACA) aneurysm who underwent endovascular treatment, and we introduce the case to share the experience of treatment.
CASE REPORT
Case presentation
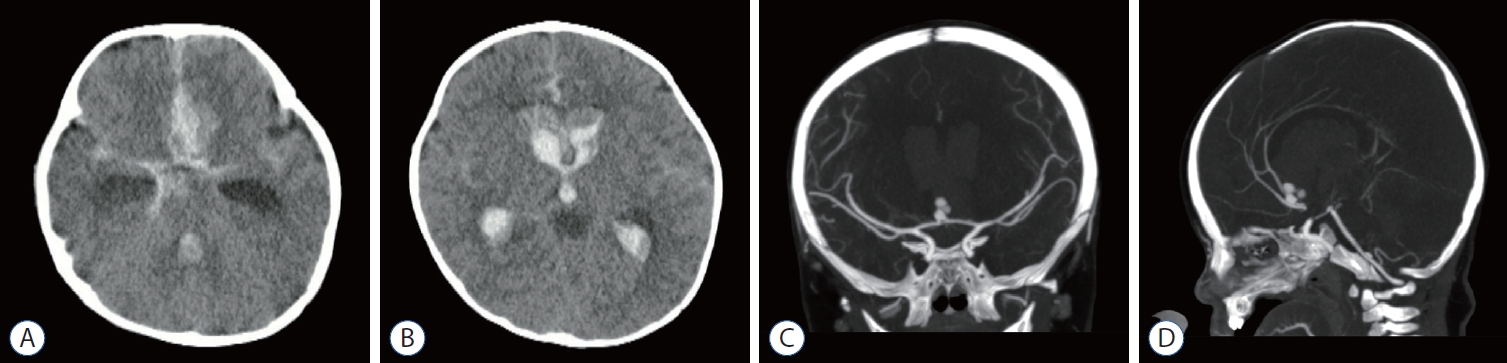
A 7-month-old male infant without perinatal medical history presented with generalized tonic-clonic seizure sustained for 30 minutes with relapsing pattern. After administration of 1 mg of lorazepam, seizure was subsided and levetiracetam was administered additionally. Initial Glasgow coma scale was E1V1M2 with decerebrated posture and the patient was hyperventilating. Both pupil size was fixed at 2 mm without light reflex and anterior fontanelle was bulged. Immediate brain computed tomography (CT) was performed and there was thick subarachnoid hemorrhage at basal cistern with massive intraventricular hemorrhage. Additional CT angiography showed ruptured proximal A2 segment of ACA aneurysm (Fig. 1).
Treatment
To control increased intracranial pressure, extraventricular drain catheter was first inserted at right Kocher’s point under general anesthesia and then the patient was transferred to angioroom. Femoral artery catheter was inserted with ultrasonogram, and 4 French Davis diagnostic catheter was placed at left internal carotid artery (ICA) without femoral sheath. In initial transfemoral cerebral angiography (TFCA), the aneurysm had a fusiform shape covering the entire A2, including the origin of the orbitofrontal artery in the proximal A2 just above the fenestration channel. The aneurysm was close to 6 mm in size with multiple blebs and appeared to have ruptured at the superior part. An aneurysm-sized pseudoaneurysm was seen around the rupture point and contrast leakage was consistently observed during TFCA and coiling. There were no certain angiographic findings suggestive of dissection, and an accurate diagnosis was difficult due to failure of magnetic resonance imaging. However, this is a fusiform aneurysm covering the entire A2 segment and considering that pediatric-type dissecting aneurysms may be different from adult-type dissecting aneurysms, a dissecting aneurysm cannot be ruled out. At first, coil embolization was considered for the persistent rupture, and coiling was performed on the true aneurysmal wall and pseudoaneurysm sac. However, anterograde ACA perfusion was undesirable due to intravascular space thrombus formation and high intracranial pressure in the serial angiogram, and coil instability was also accompanied, so endovascular trapping was planned. Because there was a perforator around the anterior communicating artery (ACoA) and it was thought to be good to maintain embryologic circulation, complete trapping was performed while preserving the orbitofrontal artery (Fig. 2). Total occlusion of aneurysm was achieved and there was no post-procedural thromboembolism. Postprocedural angiogram showed minimal leptomeningeal collaterals (Fig. 2C).
Outcome and hospital course
The patient admitted to pediatric intensive care unit. There was no improvement of neurologic status after coil embolization. At follow-up brain CT, diffuse cerebral edema with left uncal herniation and decreased grey-white matter differentiation was observed, diffuse hypoxic brain damage was suspected. Non-convulsive status epilepticus was excluded by portable electroencephalography which showed diffuse cerebral dysfunction. At postoperative day (POD) 3, transcranial doppler (TCD) ultrasound was performed and biphasic waveform was detected which means cerebral circulatory arrest. Poor prognosis was informed to parents and they decided not to perform further major operation, but wanted to maintain all medical treatment. At POD 53, chronic subdural hematoma with 4 cm-thickness was detected incidentally in brain CT and it was resolved after burr hole trephination and drainage. Inotropic agent was tapered off but need for respiratory support was sustained, so tracheostomy was performed at POD 65. With best medical care including pituitary hormone replacement, the patient transferred to general ward at POD 128 and discharged to home with portable ventilator at POD 337.
DISCUSSION
There are not many cases of infantile intracranial aneurysm. The incidence of intracranial aneurysms in the pediatric population is 0.5-4.6% of aneurysms in general population [6]. Buis et al. [3] reported systemic review of 131 cases from 1996 to 2005 about intracranial aneurysm under 1 year-old and revealed that infantile intracranial aneurysms most frequently occur at middle cerebral artery (MCA) and 50% of ruptured patient recovered to Glasgow outcome scale (GOS) 5 otherwise 31% remained under GOS 2.
Mohotti et al. [9] narrowed down the category and analyzed intracranial aneurysms in neonates. They reviewed reported cases of neonatal intracranial aneurysms from 1949 to 2017, 37 cases were reported and almost patients presented with seizure after aneurysm rupture and the location of aneurysms were MCA in 50% and distal branch in 2/3. Proportion of dissecting aneurysm is reported as 16-45% in children which is higher than general population, and there is a tendency for the rate of dissecting aneurysms to increase with younger age [5,8,12,13]. Ruptured ACA dissecting aneurysm, is particularly rare and is known to have a poor prognosis [7,16].
Trauma, infection and connective tissue disease are known as possible causes of pediatric aneurysm [3]. In this case, genetic study was not performed due to refusal of parents, but trauma and infection were excluded. Although the pathophysiology of primary pediatric intracranial aneurysm is still unclear, it is thought that hemodynamic stress upon congenital vascular anomaly with weak and thin vessel walls forms aneurysm [15]. To explain the different spatial distribution of pediatric intracranial aneurysm compared with adults, is essential to understand the embryology of ICA. Padget [11] analyzed the development of the intracranial arteries and divided it into several stages. At first, the primitive ICA divides into cranial and caudal branches, then primitive olfactory artery and medial olfactory artery origin from the cranial branch. Medial olfactory artery, the primitive form of ACA, branches orbitofrontal artery in early development stage and form a bifurcation with A2 segment of ACA. ACoA is known to be made from plexiform anastomosis and fusion of the ACAs on both sides and develops later [2,11]. The most common location of pediatric intracranial aneurysm is MCA bifurcation [15] and there were few supporting explanations of the tendency that MCA is not stable because it is a phylogenetically new vessel and contains a large blood flow from early embryonic stage [8,14].
In this case, ruptured aneurysm was located at proximal A2 segment of ACA and incorporated with orbitofrontal artery. It is correlated with the tendency of pediatric intracranial aneurysm which is more likely to occur in ACA than ACoA than adults [15]. Our hypothesis is that the tendency is based on the accumulated high hemodynamic stress upon orbitofrontal artery as the first branch of ACA during development. ACoA, on the other hand, develops from a vascular network perpendicular to the direction of blood flow, so it does not receive much hemodynamic pressure.
Seventy three percent of infantile intracranial aneurysms present with rupture and eventually have typical symptoms of subarachnoid hemorrhage such as altered mentality, seizure, headache, and vomiting. It can be difficult to differentiate with other cause because infants cannot explain symptoms, so physicians must evaluate the presence of fontanelle bulging or sunset sign. Giant aneurysm (≥25 mm) located in the posterior circulation is often found as a neurologic deficit due to mass effect [3].
There is no controlled study about treatment of pediatric aneurysm until now. However, there are efforts to establish treatment strategy with evidence based on uncontrolled study and generalization from study of adults. Beez et al. [1] reviewed modern treatment of pediatric aneurysm and showed that proportion of endovascular treatment increased after International Subarachnoid Aneurysm Trial (ISAT) which proved the superiority of coil embolization for ruptured aneurysms in prognosis when both clipping and coil embolization are possible. Endovascular treatment is especially suitable for posterior fossa aneurysm, giant aneurysm and unruptured aneurysm. Otherwise, it should be considered that clipping has better long-term durability which is important for children who have long remaining lifespan, so they emphasized the importance of an interdisciplinary decision-making process involving neurosurgeons and neurointerventionists [1,10]. Vasospasm and delayed cerebral ischemia seems to be less symptomatic due to well-developed collateral circulation and higher cerebral blood flow in children [4,8]. And it is much easier to conduct TCD ultrasound because of thin bone thickness and opened fontanelle [3].
CONCLUSION
Subarachnoid hemorrhage due to intracranial aneurysm rupture is rare but fatal, so it should be considered as a differential diagnosis in infants and should be treated actively. We share our experience about the treatment of ruptured intracranial aneurysm of infant which is rare and fatal.