INTRODUCTION
In the past decade, the unruptured intracranial aneurysm (UIA) detection rate has increased rapidly in Korea, and the treatment of these UIAs has increased accordingly10).
Because the natural history of UIA has not been clearly defined, the decision to treat incidentally detected UIAs smaller than 5 or 7 mm in diameter remains controversial, especially when these UIAs are located in the anterior circulation.
The carefully conducted International Study of UIAs (ISUIA) reported a very low rupture rate for small anterior circulation UIAs17,21). Furthermore, a recent study based on a European population reported an overall annual incidence of SAH from the rupture of small incidental aneurysms in the anterior circulation of 0.2%, which was therefore comparable with data from the ISUIA3). However, other recent studies on UIA in the Japanese population, such as the Small Unruptured Aneurysm Verification Study (SUAVe Study) and the Unruptured Cerebral Aneurysm Study (UCAS), reported a higher rupture rate for small anterior circulation UIA15,16).
The reasons underlying the observed difference in rupture risk between Western and Japanese populations are currently unclear. More importantly, little information is available about the natural history of small anterior circulation UIA in the Korean population. Therefore, we conducted a retrospective cohort study at our institute.
MATERIALS AND METHODS
Data from patients diagnosed with UIA from March 2000 to May 2008 at our hospital were subjected to a retrospective anaylysis. This study was approved by the Institutional Review Board at our hospital (B-1307-210-114).
Patient selection
The patient inclusion criteria were age 18 years or older and presence of at least 1 UIA with a largest dimension >3, determined using a standard measuring device. Patients with a history of ruptured aneurysm at another location that had been repaired via open surgical or endovascular treatment were included.
We excluded patients who 1) had a previous intracranial hemorrhage event of unknown origin, 2) could not care for themselves indicated by a modified Rankin score of >2 at the time of aneurysm identification, 3) had fusiform, traumatic, or mycotic aneurysms, 4) had giant aneurysms (>25 mm in size), 5) had aneurysms related to arteriovenous malformations, and 6) had aneurysms located at the cavernous portion of the internal carotid artery or the posterior circulation18).
Data collection
For the purpose of follow-up, day 0 was defined as the day when an imaging study first identified a patient's UIA. We also collected data regarding baseline characteristics. Patient factors such as age, sex, hypertension (HTN), diabetes mellitus (DM), heart disease (HD), smoking history, previous episode of subarachnoid hemorrhage (SAH) from a ruptured aneurysm at another location, and angiographic factors such as aneurysm size, location, and multiplicity were analyzed. Patients were categorized into 2 groups according to their age : вүҘ70 years and <70 years. Aneurysms were categorized according to size and location. All UIAs were classified into the following categories based on size : 3-4.9 mm, 5-6.9 mm, 7-9.9 mm, and 10-24.9 mm. Because all of the aneurysms larger than 25 mm in size were treated, we excluded these aneurysms. All UIAs were also classified into the following categories based on location : middle cerebral artery (MCA), anterior communicating artery (ACoA), internal carotid artery (ICA), posterior communicating artery (PCoA), and others. "ICA" included the paraclinoid segment, internal carotid artery bifurcation, and origin of the anterior choroidal artery and excludes those located at the origin of the posterior communicating artery and cavernous portion. "Others" included aneurysms at the A1 portion of the anterior cerebral artery and distal anterior cerebral artery. Aneurysms were also divided into 2 groups : non-treated, without any aneurysm repair during the follow-up period, and treated, with aneurysm repair via an open surgical or endovascular procedure. The UIA size was measured via catheter angiography or three-dimensional computed tomography (CT) angiography, and the largest UIA dimension was used for the analysis.
After diagnosis, the patient's clinical status was followed up on the basis of their medical records. Aneurysm rupture was assessed using the information available from the patient's last outpatient or emergency department visit. At the time of data collection, if a patient had not undergone a follow-up for more than 6 months, a telephone interview was conducted to confirm the patient's clinical status.
The primary end point of the study was UIA rupture. The secondary end-point of the study was the ninth year after UIA diagnosis. During the follow-up period, some patients underwent either an open surgical or endovascular treatment prior to aneurysm rupture. Data were no longer collected for a patient at the time 1) when the aneurysm was repaired with open surgical or endovascular treatment, or 2) when the patient died of causes other than aneurysm rupture, or 3) when the patient could no longer be followed.
Statistical analysis
Data were analyzed using IBM SPSS statistical software, version 19.0 (IBM Corp., Armonk, NY, USA). We compared the baseline characteristics of not-treated group and treated group. Student t-test was used to compare the continuous variables and chi-square test was used to compare the categorical variables. Continuous variables are presented as meanВұstandard deviation (SD).
The annual and cumulative rupture rates of unruptured aneurysms according to the follow-up period were calculated using a life table. Risk factors for aneurysmal rupture were determined using a Cox proportional hazards regression model. Univariate Cox proportional hazards regression analyses were performed to assess categorical variables associated with aneurysmal rupture. The cumulative rates of aneurysmal rupture according to the risk factors confirmed via univariate Cox proportional hazards regression analysis were compared using the Kaplan-Meier method and statistical differences were revealed by log-rank test. Subsequently, a multivariate Cox proportional hazards regression model was used to identify independent risk factors for aneurysm rupture. Factors related to UIA rupture with a p-value<0.2 in a univariate analysis were included in a multivariate analysis. p-value<0.05 was considered statistically significant.
RESULTS
Characteristics of patients
A total 1339 aneurysms in 1006 patients met the inclusion criteria. During the follow-up period, 685 aneurysms underwent treatment prior to rupture at a median interval of 1.1 months (range from 0-67.4 months) after day 0. Among them, 209 aneurysms were repaired with open surgical treatment and 476 aneurysms were repaired with endovascular treatment. Six hundred fifty-four UIAs were followed-up without any repair. Among these, 38 occured in patients whose died of causes other than aneurysm rupture, and another 93 occured in patients whose follow-ups were discontinued; 18 aneurysms ruptured after a median follow-up period of 1.6 years (range from 27 days to 9.8 years) after day 0.
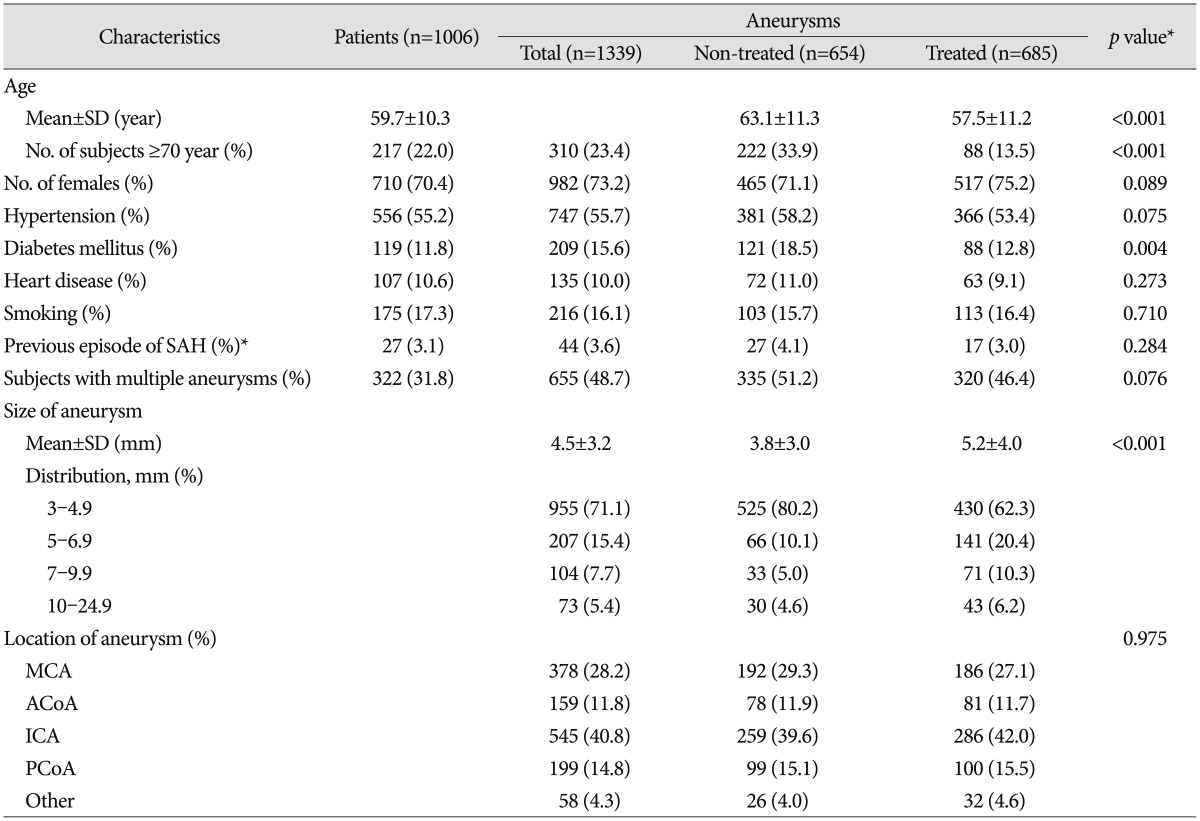
The baseline characteristics of patients and aneurysms are shown in Table 1. The mean UIA size was 4.5Вұ3.2 mm. Among all UIAs, 86.5% were smaller than 7 mm. A comparison of the non-treated and treated groups revealed statistically significant differences in patient age, DM, and UIA size.
Natural history of the aneurysms
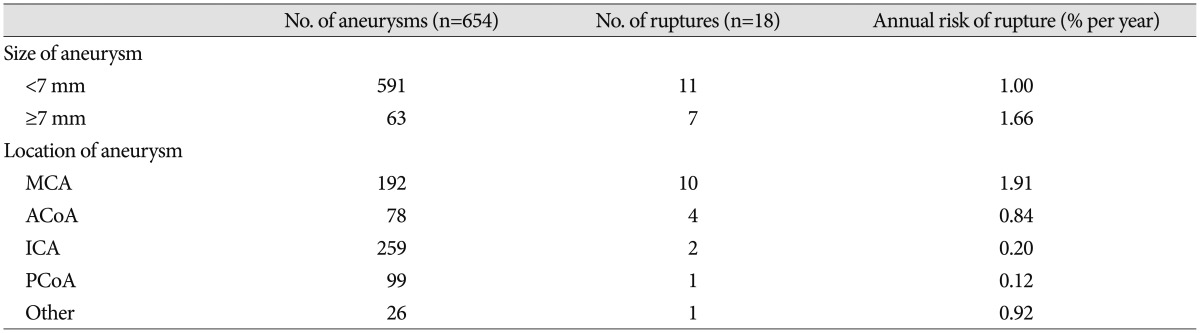
In our analysis, 18 aneurysms ruptured during a 9-year follow-up period, and the annual rupture risk was 1.00%. The cumulative rupture rates, calculated using the Kaplan-Meier method, were 0.62% within 1 year, 1.60% within 2 years, 1.78% within 3 years, 3.40% within 5 years, and 9.04% within 9 years.
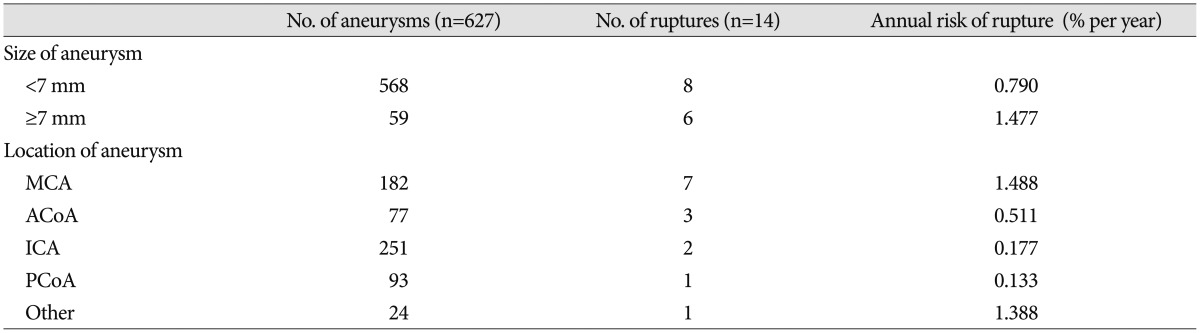
For aneurysms with largest dimension <7 mm, the annual rupture risk was 1.00%. In particular, in the absence of a history of SAH, the rupture risk for aneurysms smaller than 7 mm was 0.79% (Table 2, 3).
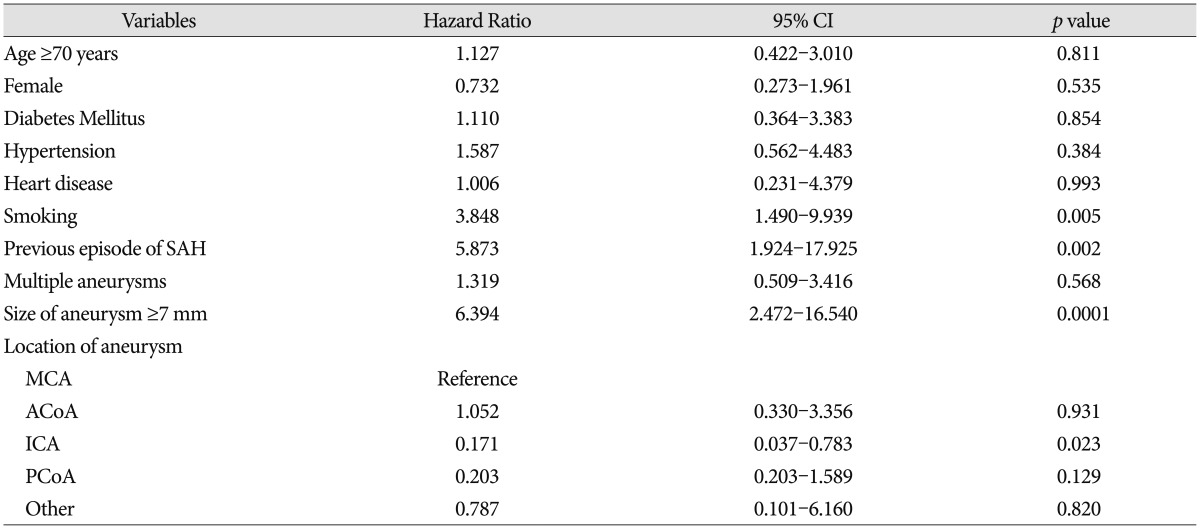
Hazard ratios (HRs) for ruptures were obtained using univariate and multivariate Cox proportional hazards analyses. In the univariate analyses, an older age (вүҘ70 years), larger aneurysm size (вүҘ7 mm), DM, HTN, heart disease, smoking history, previous episode of SAH, and aneurysm multiplicity increased the rupture risk. Among these factors, a smoking history, previous episode of SAH, and larger aneurysm size (вүҘ7 mm) were statistically significant (Fig. 1). Compared with aneurysms located at the middle cerebral artery, aneurysms located at the ICA had a significantly lower HR for aneurysmal rupture (Table 4).
A multivariate Cox proportional hazards analysis indicated that a smoking history, previous episode of SAH, and a larger aneurysm size (вүҘ7 mm) were independent risk factors for an increased risk of aneurysmal rupture (Table 5). Furthermore, the multivariate analysis found no statistically significant difference in the rupture risk according to the aneurysm location.
DISCUSSION
Little is known about the natural course of UIAs in the Korean population. Recently, a longitudinal study based on national representative insurance claim data demonstrated a rupture rate of 0.9 cases/100 people per year11). However, that study used ICD-10 diagnostic code criteria in insurance-claim data and therefore did not provide detailed information about the aneurysm rupture risks based on characteristics such as size and location.
Our study determined an overall annual rupture rate for UIA of 1.00%. In particular, the annual rupture rate of aneurysms smaller than 7 mm in diameter at diagnosis (0.79%) was lower than the overall annual rupture rate. Additionally, the cumulative rupture rates were 0.62% within 1 year, 1.60% within 2 years, 1.78% within 3 years, 3.40% within 5 years, and 9.04% within 9 years. A prospective study of a Western population reported an overall annual rupture rate of 0.2%. This rate is lower than the rate determined in our study3). However, the rate determined in the UCAS for a Japanese cohort was similar to that of our study (0.95%)16). The annual and cumulative rupture rates reported from a long-term follow up study of unruptured UIAs in a Western country were also similar to those in our study (1.1% and 10.5%, respectively)8).
Our study also demonstrates that the natural history of UIA is influenced by the size of the aneurysm. In particular, aneurysms larger than 7 mm were associated with a statistically significant increase in the rupture risk. This finding is consistent with the results of the ISUIA regarding Western populations and of the UCAS regarding a Japanese cohort.
The most important finding of our study is that the rupture risk of UIAs smaller than 7 mm and in the absence of a history of SAH was 0.79% per year. This result is higher than that reported by the ISUIA (about 0.05% per year). However, the rate in our study is similar to the rupture risk reported by UCAS for aneurysms smaller than 5 mm (0.36% per year) and that reported by the SUAVe study (0.34% per year)16,17).
The aneurysm rupture risk is well known to different among countries. Compared to other populations, the Japanese population has a higher risk of SAH, even though the incidence of UIA in the Japanese population is similar to that in Western populations2,19). Although reason for the difference in the UIA rupture risk of Korean and Japanese populations and that of Western populations might be multifactorial, but racial genetic differences may play an important role. An accumulating body of evidence indicates that inflammation is a critical contributor to aneurysm pathogenesis1). Additionally, some studies suggest that Asians may be more susceptible to intracranial atherosclerosis12). Our study shows that for a Korean patient population, the rupture risk for a small anterior circulation UIA without a previous episode of SAH differ from the risk of Western populations, but similar to that of the Japanese population.
In our study, independent risk factors for aneurysm rupture were a smoking history, previous episode of SAH, and a larger aneurysm size (вүҘ7 mm). Some previous reports demonstrated mechanisms by which smoking increases the risk of aneurysm rupture. For example, the aneurysmal wall is weakened by vessel wall inflammation due to smoking, which in turn increases aneurysmal growth. In addition, smoking triggers a transient increase in blood pressure, which contributes to aneurysm rupture5,67,14). Ishibashi et al.4) reported that a previous episode of SAH was a risk factor for aneurysm rupture but did not identify a mechanism. Many studies have also reported a correlation between the aneurysm size and rupture rate3,46,813,20). However, these studies did not use the same datum points. Nevertheless, a greater increase in aneurysm size is associated with a greater increase in the rupture rate.
Several reports discussed hypertension, age, sex, hyperlipidemia, alcohol consumption, and aneurysm location, morphology, and multiplicity as risk factors for aneurysm rupture3,46,89,1320). However, these factors were not statistically significant in our study. An additional multivariate analysis of various factors associated with aneurysm rupture will be needed to identify the risk factors for aneurysm rupture.
The limitations of our study included the retrospective nature and relatively small cohort. Additionally, the annual and cumulative rupture rates might have been underestimated because patients with a strong likelihood of aneurysm rupture were treated. However, 90.3% of aneurysms in the non-treated group were smaller than 7 mm. Therefore, although the overall rupture risk might have been influenced by selection bias, the influence of a small anterior circulation UIA measuring <7 mm in the largest dimension on both the annual rupture risk and our analysis of individual risk factors for rupture would have been small.
CONCLUSION
Our study shows that the natural history of UIAs in Korean population depends on the size of the aneurysm and any previous history of SAH. In Korean population, the annual risk of rupture for small anterior circulation UIAs without an episode of previous SAH is higher than that in Western populations, but it is comparable to the Japanese population.