Desmoplastic Fibroma of the Cranium in a Young Man
Article information
Abstract
Desmoplastic fibroma, which develops predominantly in long bones and the mandible, is a rare and benign but locally aggressive tumor. Desmoplastic fibroma of the cranium is extremely rare. We report a case of desmoplastic fibroma of the frontal bone in a young man. Because of its locally aggressive behavior, complete surgical excision with a safety margin is essential.
INTRODUCTION
Desmoplastic fibroma (DF) is an intra-osseous tumor that frequently occurs in long bones and the mandible15). These tumors are histologically benign but show locally aggressive behavior9). Without complete resection, frequent local recurrence occurs12). DF in the cranium is extremely rare. Since the first report by Gardini et al.7) in 1978, fewer than 20 cases have been described in the literature5,11,14). In this report, we present a case of DF in the cranium. Differential diagnosis and treatment strategy are discussed with a literature review.
CASE REPORT
A 20-year-old man visited our clinic with a 1-year history of worsening headache and swelling of the right frontal region. Physical examination revealed bony swelling with a smooth cortical lining. The swollen area was mildly tender, and the overlying scalp was intact. Neurological examination was unremarkable. Plain skull X-ray films demonstrated a lytic lesion with a sclerotic margin. A computed tomographic (CT) scan demonstrated a 3×3.5-cm focal calvarial thickening and expansion of the diploic space by a hypo-attenuated mass with a sclerotic margin and ground-glass appearance. Magnetic resonance imaging showed heterogeneous signal intensity on T2-weighted images and intermediate signal intensity on T1-weighted images with multifocal enhancement (Fig. 1). There was no soft tissue or intracranial invasion. Focal hot uptake at the lesion site was observed on bone scan.
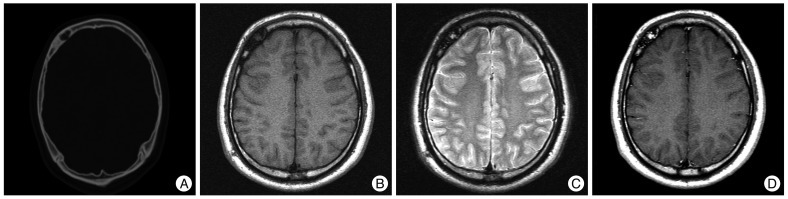
A : CT scan demonstrating focal calvarial thickening of right frontal skull. B, C and D : MRI reveals intermediate signal intensity on T1-weighted images and heterogeneous intensity on T2-weighted images with multifocal enhancement.
The patient underwent a craniectomy under general anesthesia. The lesion was completely excised with sufficient safety margins by inspection under guidance of intra-operative navigation. There were neither scalp nor dural invasions. The gross specimen was bulging with a pinkish color at the lesion site, which contained a round dark-brownish area with a sclerotic margin in the diploic space, slightly expanded and thicker compared to normal bone flaps. Sectioning after decalcification revealed an ill-defined fibrotic area. The lesion was accompanied by yellow necrotic foci and exhibited fibroblastic proliferation within a collagenous background, with extensive hemorrhage and fat necrosis. Tumor cells included spindle cells and lacked significant unclear atypia and mitotic figures. These findings suggested desmoplastic fibroma of the skull. Immunohistochemical stain for smooth muscle actin (SMA) was focally positive (Fig. 2), and S-100 was positive. Other markers such as EMA, CD34, CD68, vimentin, and desmin were negative. All margins were free of tumor cells.

A : Micrograph of the lesion showing spindle cell proliferation with hemorrhage and fat necrosis (H&E, ×100). B : Note fibroblastic proliferation with collagenous background (H&E, ×200). C : Smooth muscle actin staining revealed focal positivity (×200).
DISCUSSION
First described by Jaffe in 1958, desmoplastic fibroma is recognized as a separate entity from bone tumors. DF is a rare benign bone tumor composed of spindle cells accounting for 0.3% of benign bone tumors13). The World Health Organization describes DF as exhibiting "minimal cytological atypia and abundant collagen production"6). DF can occur at any age, but most cases occur before age 301). DF may involve any bone, but commonly occurs in the metaphyses of the long bones, mandible, and pelvis, and cranial DFs are exceedingly rare. DFs affect both genders, although a female preference has been suggested for cranial DF12). Despite benign histological appearance and slow growth, frequent local recurrence puts DF in a category between benign and malignant bone tumors3). Clinical symptoms include headache, cranial asymmetry, ear symptoms, and skull mass. Intracranial involvement was reported in one case, but brain parenchymal invasion has not been reported17).
Radiographically, cranial DFs are often solitary, honeycomb, or trabeculated lytic lesions, with expansion of the diploic space with or without marginal sclerosis8). CT scans typically show destruction and thinning of the cortex. Dense connective tissue and hypocellularity yields heterogeneous signal intensity on T2 and iso-signal intensity on T1-weighted magnetic resonance images with heterogeneous enhancement9,16). These findings are not distinctive compared to other skull lesions such as fibrous dysplasia, hemangioma, eosinophilic granuloma, low-grade osteosarcoma, or metastasis. Given its rarity and nonspecific radiographic findings, it is very difficult to diagnose cranial DFs.
Differential histopathological diagnosis includes benign and malignant spindle cell bone tumors, including fibrous dysplasia, fibrosarcoma, low-grade intra-osseous osteosarcoma, and non-ossifying fibroma10). The crucial differential diagnosis is low-grade fibrosarcoma. Typical fibrosarcoma is more cellular with a herringbone pattern that shows more pleomorphism and higher mitotic activity4). In fibrous dysplasia, recognition of C-shaped, woven bone formation within a fibrous background is an important diagnostic feature. Osteoid production is generally evident in intraosseous osteosarcoma. Non-ossifying fibroma consists of cellular masses of fibrous tissue often arranged in a storiform pattern. Foamy and hemosiderin-laden macrophages are common in non-ossifying fibroma. Hemorrhage and fat necrosis seen in our case are uncommon findings in DF. Immunohistochemistry of DF may be positive for SMA, vimentin, and desmin, while cytokeratin, S-100, EMA, and CD16 are negative18).
Surgical resection with adequate margins, with cranioplasty, is the treatment of choice. Recurrence is rare if negative margins are achieved. Despite some reports that endocrine therapy with tamoxifen can be effective, chemo- and radiotherapeutic approaches in DF have not been established2). So far, there are no reports of recurrence in cranial DF, which may be due to feasibility of wide excision in skull lesions. Since cranial DF remains poorly understood, radiographic follow-up is warranted, especially in incomplete resection cases.
CONCLUSION
DF is uncommon, but should be considered in differential diagnosis of any expansile cranial mass. Because DF may be locally aggressive, en bloc resection with adequate margin is the treatment of choice.