Grading of Intracerebral Hemorrhage in Ruptured Middle Cerebral Artery Aneurysms
Article information
Abstract
Objective
To propose grading of intracerebral hemorrhage (ICH) in ruptured middle cerebral artery (MCA) aneurysms, which helps to predict the prognosis more accurately.
Methods
From August 2005 to December 2010, 27 cases of emergent hematoma evacuation and aneurysm clipping for MCA aneurysms were done in the author's clinic. Three variables were considered in grading the ICH, which were 1) hematoma volume, 2) diffuse subarachnoid hemorrhage (SAH) that extends to the contralateral sylvian cistern, and 3) the presence of midline shifting from computed tomography findings. For hematoma volume of greater than 25 mL, we assigned 2 points whereas 1 point for less than 25 cc. We also assigned 1 point for the presence of diffuse SAH whereas 0 point for the absence of it. Then, 1 point was assigned for midline shifting of greater than 5 mm whereas 0 point for less than 5 mm.
Results
According to the grading system, the numbers of patients from grade 1 to 4 were 4, 6, 8 and 9 respectively and 5, 7, 8, 4 and 3 patients belonged to Glasgow Outcome Scale (GOS) 5 to 1 respectively. It was found that the patients with higher GOS had lower ICH grade which were confirmed to be statistically significant (p<0.01). Preoperative Hunt and Hess grade and absence of midline shifting were the factors to predict favorable outcome.
Conclusion
The ICH grading system composed of above three variables was helpful in predicting the patient's outcome more accurately.
INTRODUCTION
The middle cerebral artery (MCA) aneurysm is about 20-30% of all intracranial aneurysms, and about half of them cause intracerebral hemorrhage (ICH) when rupture of aneurysms occur2,3,6,7). The surgical results have varied, but dramatic improvement after operation can be noted similar to patients with an acute epidural hematoma11).
Shimoda et al.17) classified the ICH in ruptured MCA aneurysm into three categories : 1) temporal ICH, 2) intrasylvian hematoma and 3) ICH with diffuse subarachnoid hemorrhage (SAH). They reported that temporal ICH with the volume less than 25 cc showed good prognosis whereas ICH with diffuse SAH showed bad outcome.
However, this classification has following problems. 1) Aneurysms with certain directions can cause isolated frontal ICH and it does not belong to any of the categories stated above. 2) The definition of intrasylvian hematoma is ambiguous. Patient with both frontal and temporal lobe hematoma can be classified into intrasylvian hematoma but the prognosis depending on the amount of hematoma is not readily reflected. 3) Even in the presence of diffuse SAH, if the volume of ICH is little with minimal midline shifting, the clinical course does not always go so bad. Therefore, we would like to propose a new modified grading system to solve the problems.
MATERIALS AND METHODS
Ninety-five patients of SAH from ruptured MCA aneurysm were admitted from August 2005 to December 2010. Twenty-nine patients (31%) among them had shown ICH more than 5 cc in computerized tomography (CT) scan. The evacuation of hematoma and clipping of aneurysm were performed in 27 patients. The mean age of the patients was 54.3 years, and the male to female ratio was 1 : 1.7. Initial neurological status was described in Hunt and Hess grade. Hematoma volume was calculated from the caliber of CT images.
For the ICH grading system 1 or 2 points were assigned based on the volume of less or greater than 25 mL respectively. According to Shimoda et al.17), extensions of SAH to the contralateral sylvian cistern were named "Diffuse SAH", and it was assigned 1 point in the hematoma scale. One point was assigned to midline shifting more than 5 mm whereas 0 point for less than 5 mm (Table 1). The hematoma score of the most severe patient is 4, which means high amounts of volume with midline shifting and diffuse SAH. The final results were presented as Glasgow Outcome Scale (GOS).

ICH grading system in ruptured MCA aneurysm
Statistical analyses were performed using the Kruskal-Wallis test or chi-square test, and p value less than 0.05 were considered to be significant.
RESULTS
Clinical presentations
The clinical data and outcomes are presented in Table 2. The numbers of patients for the initial Hunt-Hess grade 1 to 5 were 0, 3, 3, 19 and 2, respectively. According to this grading system, the numbers of patients from grade 1 to 4 were 4, 6, 8 and 9 respectively and 5, 7, 8, 4 and 3 patients belonged to GOS 5 to 1 respectively. The initial Hunt-Hess grade was significant factor to final outcome (p<0.05).
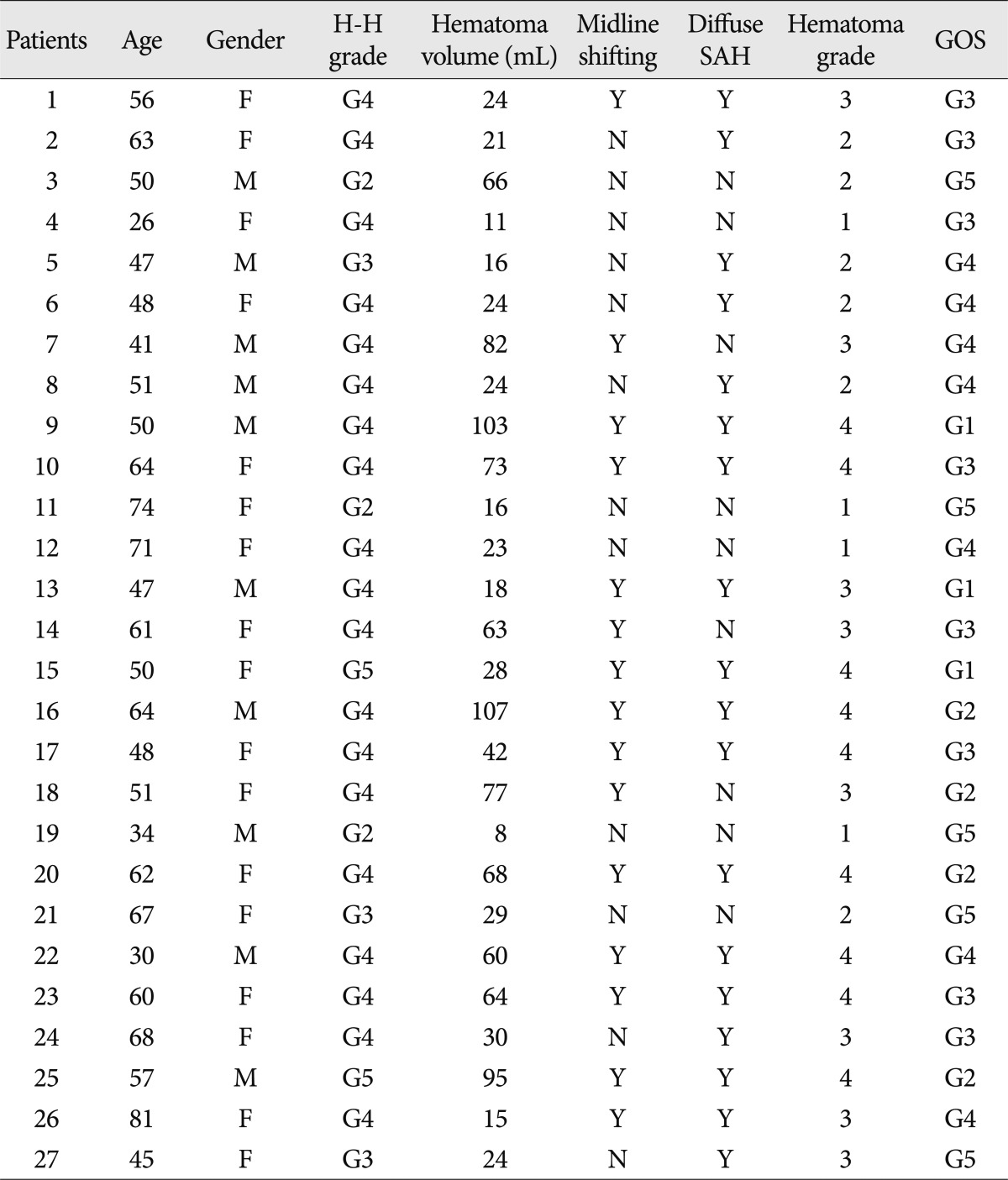
Clinical data of the patients
Hematoma volume and outcome
Fifteen out of twenty-seven patients showed large hematoma more than 25 cc, and twelve of them showed poor initial neurological status. Twelve patients had small hematoma, and eight patients with less than 25 mL had poor grade SAH. The good outcomes (GOS 4 or 5) were found in 5 out of 15 and 7 out of 12 patients with hematoma volume of greater or less than 25 cc, respectively. Hematoma volume alone was not related to outcome (p=0.286).
Diffuse SAH and outcome
Diffuse SAH extending to contralateral sylvian cistern was seen in eighteen out of 27 patients. Most of those patients except two showed poor initial consciousness, and only 33.3% of them showed favorable outcome. Diffuse SAH alone was not related to the outcome statistically (p=0.08).
Midline shifting and outcome
All fifteen patients who had midline shifting in CT scan showed poor initial consciousness with Hunt-Hess 4 or 5. Out of fifteen, twelve patients had poor outcome with GOS 1 to 3. The outcome of twelve patients without midline shifting was relatively favorable in which only 3 patients had GOS of 3 at least. Presence of midline shifting was the statistically significant prognostic variable (p=0.001). Midline shifting was the most important factor than hematoma volume or diffuse SAH.
ICH grade and outcome
ICH grade was composed of hematoma volume, diffuse SAH, and midline shifting. The hematoma grade 4 which means large hematoma and diffuse SAH with midline shifting more than 5 mm in CT scan, showed the worst outcome. Hematoma grade and GOS was found to be correlated with each other statistically (p=0.006).
DISCUSSION
Most spontaneous SAHs result from rupture of intracranial aneurysms, and the shape of SAH along basal cistern is often determined by the location of ruptured aneurysm. For example, thick hematoma around the frontal area of basal cistern means rupture from anterior communicating artery aneurysm. If dense hematoma is located along posterior cerebral artery territory rather than common basal cistern, it may be from rupture of posterior circulation aneurysm. Middle cerebral artery aneurysm is the next to anterior communicating artery aneurysm in cases13). It has two characteristic findings in CT scan. First, dense SAHs are lateralized along the ruptured MCA territory. Second, temporal hematoma without definite SAH may be found, and misunderstood as hypertensive ICH if CT angiography or cerebral angiography is not performed. The formation of temporal ICH is explained by the aneurysm bursting at the dome site completely adherent to pia mater without destructing the cortex around the rupture point, hemorrhage may occur directly into the brain parenchyme without definite SAH15,16).
Kopera et al.14) classified the types of ICH from ruptured MCA aneurysm into three groups as temporal ICH, intrasylvian hematoma, and ICH with diffuse SAH. They reported a favorable outcome in temporal ICH rather than ICH with diffuse SAH. They analyzed these findings from the rapid reduction of IICP by early evacuation of hematoma. These findings were reported in other studies5,15). They commonly reported favorable outcome of temporal hematoma and poor outcome of intrasylvian hematoma with brain swelling. Presence of temporal hematoma without SAH makes the prognosis good after surgery like acute epidural hematoma. The initial neurological status with large hematoma more than 25 mL were much poorer, but the statistical relationship between hematoma volume and prognosis was not found in our study. Large hematoma makes brain more swollen by its mass effect and increasing the local pressure that inhibits hemodynamic circulation.
Diffuse SAH means wide dispersed hematoma extending to contralateral sylvian cistern. Shimoda et al.17) reported the poor outcome of diffuse SAH, and it is due to high rates of cerebral vasospasm and surgical difficulty than temporal hematoma. Diffuse hematoma can be somewhat removed gradually by suction and irrigation in the operating field. According to Inagawa,12) clot removal during operation might ameliorate cerebral vasospasm, but its effect per se does not seem to be significant.
In our study, statistic significance between hematoma volume or diffuse SAH and outcomes was not noted compared to that of midline shifting or hematoma grade. Diffuse SAH showed the value near to statistic significance (p=0.08), and if studied in more cases, it might be gained more important results.
Midline shifting represents the severity of ipsilateral cerebral swelling. Niikawa et al.15) explained sudden formation of ICH might insult the surrounding brain, and blood-brain barrier disruption followed by increased permeability of endothelial cells and the tight junction may occur, resulting in formation of vasogenic cerebral edema. They also can be caused by surgical manipulation that would result in secondary postoperative vasogenic edema. Midline shifting was the most related variable to the outcome statistically.
The ICH grade was made from three variables which are easily detected from CT scan. The prognostic values of CT scan have been reported in many studies, and SAH grade based on the findings were presented since the introduction of CT scan. In general, the severity of CT findings parallel with consciousness level in predicting mortality or good recovery1,4,8-10). MCA aneurysm shows characteristic formation of temporal hematoma, so we thought the hematoma volume should be initially considered in making ICH grade. Diffuse SAH and midline shifting represent overall injury of the brain, and if added to the hematoma volume, they would present typical characteristics of ruptured MCA aneurysms. ICH grade made of three variables would help to predict the outcome and the hypothesis was verified. The ICH grade was statistically significant to predict outcomes.
CONCLUSION
MCA aneurysm shows easy formation of temporal hematoma, diffuse SAH, and ipsilateral cerebral swelling. Hematoma volume and diffuse SAH were not related to the outcomes, but midline shifting alone was the independent factors for the outcomes. The ICH grade made from above three variables helps to predict prognosis of ruptured MCA aneurysm patients. Early or emergent hematoma evacuation and aneurysm surgeries are necessary to lower IICP in such patients.
Acknowledgements
This work was supported by Konkuk University in 2012.