Surgical Decision Making for the Elderly Patients in Severe Head Injuries
Article information
Abstract
Objective
Age is a strong predictor of mortality in traumatic brain injuries. A surgical decision making is difficult especially for the elderly patients with severe head injuries. We studied so-called 'withholding a life-saving surgery' over a two year period at a university hospital.
Methods
We collected data from 227 elderly patients. In 35 patients with Glasgow Coma Score 3-8, 28 patients had lesions that required operation. A life-saving surgery was withheld in 15 patients either by doctors and/or the families (Group A). Surgery was performed in 13 patients (Group B). We retrospectively examined the medical records and radiological findings of these 28 patients. We calculated the predicted probability of 6 month mortality (IPM) and 6 month unfavorable outcome (IPU) to compare the result of decision by the International Mission for Prognosis and Analysis of Clinical Trials in TBI (IMPACT) calculator.
Results
Types of the mass lesion did not affect on the surgical decision making. None of the motor score 1 underwent surgery, while all patients with reactive pupils underwent surgery. Causes of injury or episodes of hypoxia/hypotension might have affected on the decision making, however, their role was not distinct. All patients in the group A died. In the group B, the outcome was unfavorable in 11 of 13 patients. Patients with high IPM or IPU were more common in group A than group B. Wrong decisions brought futile cares.
Conclusion
Ethical training and developing decision-making skills are necessary including shared decision making.
INTRODUCTION
In traumatic brain injuries, age is one of the strongest predictors of mortality and functional outcome14,22). Older age is associated with poorer outcome1,11,16,24). 100% mortality rate in elderly patients aged >80 years, with a Glasgow Coma Scale (GCS) of 11 or less, and other studies have reported that surgery on elderly patients with a GCS of 5 or less was incompatible with survival2). However, an older age is continuously associated with a worsening outcome after traumatic brain injuries11). The decision to offer life-saving, but not restorative, surgery to patients with severe neurotrauma is difficult10). Balancing the risk of not doing enough against the risk of doing too much with the result of poor neurological recovery is emotionally challenging, both for health care providers and the families of patients10).
Decision making is a key competency of surgeons; however, how best to assess decisions and decision makers is not clearly established14). It is hard to learn or study the good decision making. We studied the frequency and the basis of so-called 'withholding a life-saving surgery' over a two year period at a university hospital, in order to analyze how such situations are handled on a daily basis.
MATERIALS AND METHODS
Patient recruitment started in January 2011 and ended in December 2012. During this period, 577 patients were admitted after head injuries. We could collect 227 elderly (over 60 years) patients (Table 1). The level of consciousness was measured by the GCS score on admission. In 35 patients with GCS 3-8, 28 patients had surgical lesion. A life-saving surgery was withheld in 15 patients either by doctors and/or the families of patients (Group A). Surgery was performed in 13 patients (Group B).
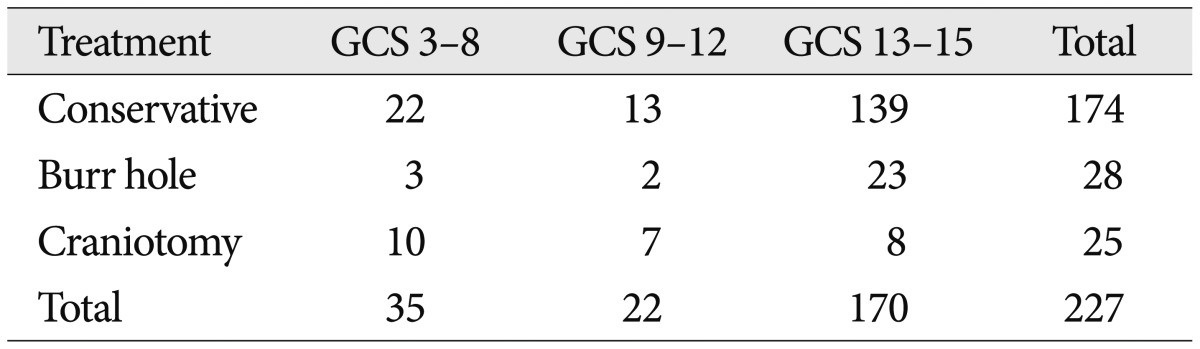
Treatment of elderly patients with head injuries
We retrospectively examined the medical records and radiological findings of these 28 patients. We obtained the predicted probability of 6 month mortality (IPM) and 6 month unfavorable outcome (IPU) to compare the result of decision making by the International Mission for Prognosis and Analysis of Clinical Trials in TBI (IMPACT) calculator22). IPM and IPU were automatically calculated by the IMPACT calculator at the internet homepage (http://www.tbi-impact.org/?p=impact/calc). The predicted risk of mortality or unfavorable outcome was not used during the patient management. The outcome was measured by the Glasgow outcome scale at the time of discharge.
Statistical analysis was performed using the chi-square test or Fisher's exact test. For the statistical significance, we divided the etiology into either known or unknown groups. The outcome was also divided into either favorable (good recovery and moderate disability) or unfavorable (from severe disability to death). Differences were considered significant if the probability value was less than 0.05.
RESULTS
The most common surgical lesion was acute subdural hematoma in both groups (Table 2). Types of the surgical lesion did not affect the surgical decision making. None of the motor score 1 underwent surgery. Although low (1-3) motor score was more common in the group A, this difference could not reach to the statistical significance (p>0.05, by Fisher test). Pupillary response was a major factor of decision making. All patients with reactive pupils underwent surgery. In 18 patients with both dilated pupils, only five of them underwent surgery. The outcome was unfavorable in all (1 death, 3 vegetative states, and 1 severe disability). Causes of injury or episodes of hypoxia/hypotension might affect on the decision making, however, their role was not distinct.
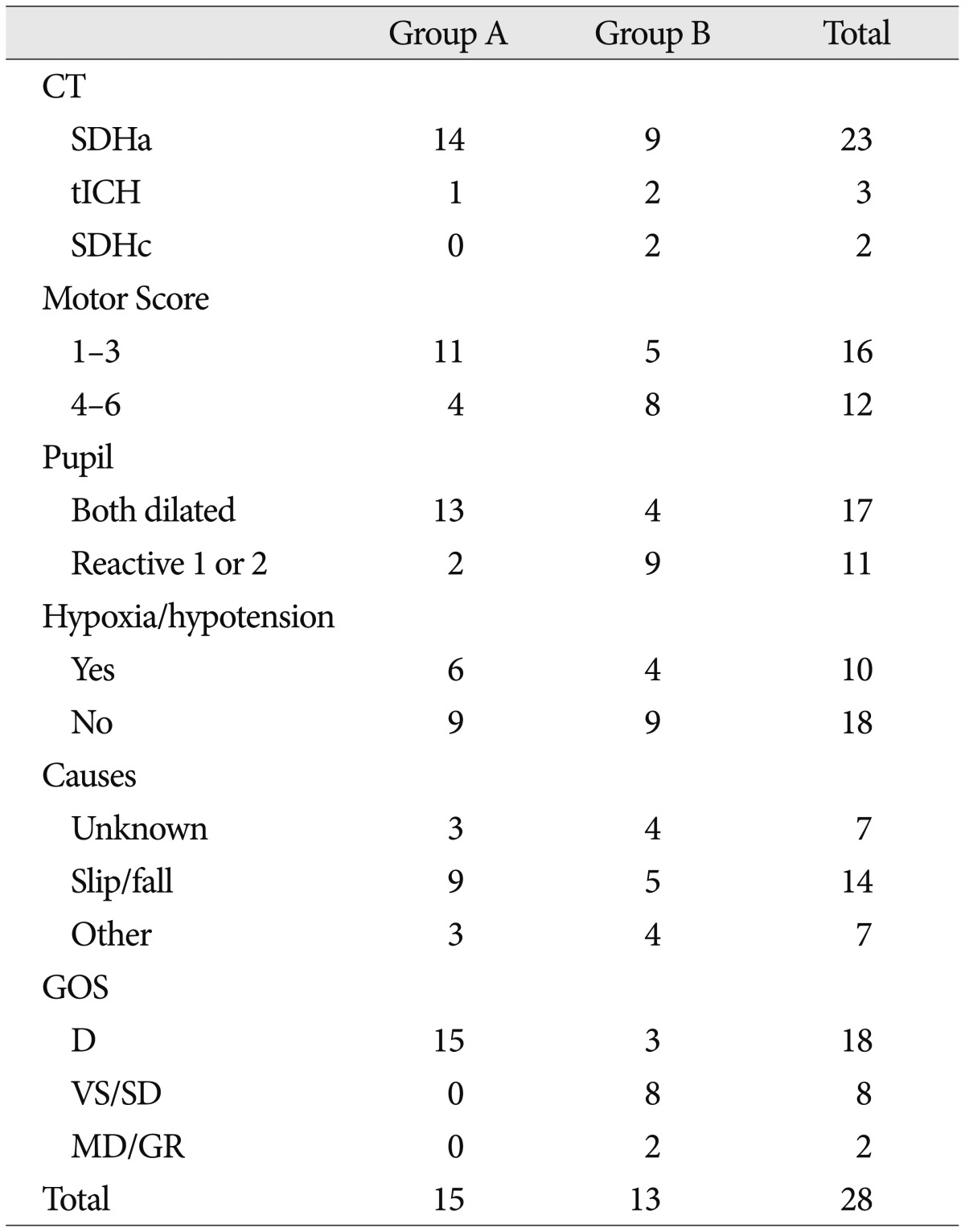
Clinical characteristics of elderly patients with severe head injuries
All patients in the group A were expired within 3 days, except one (case 4). In the group B, 10 patients could survive, however the outcome was unfavorable in 8 patients.
The IPM ranged from 54% to 90% in the group A (mean 82%); from 29% to 91% in the group B (mean 54.2%) by core model (IPMc). The IPU ranged from 73% to 97% in the group A (mean 91.5%); from 44% to 98% in the group B (mean 71.0%) by core model (IPUc). Patients with high IPM or IPU were more common in group A than group B, either by core model or core+ CT model (Table 3). These differences were statistically significant (p<0.05, by Fisher's test).
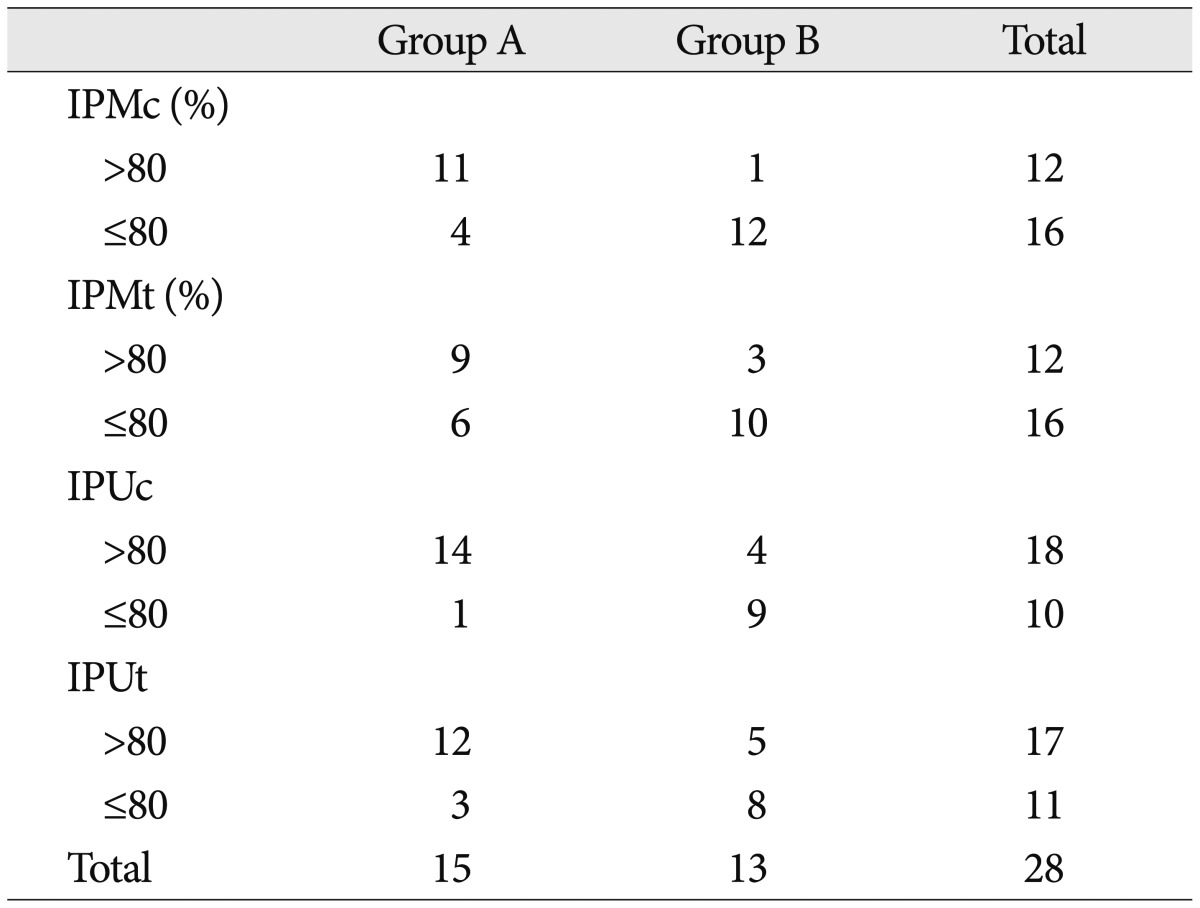
The predicted probability of 6 month mortality by the IMPACT calculator
We tried to illustrate 6 cases; four patients withheld surgery despite of relatively low probability of mortality or young age, two patients underwent surgery even though the risk of mortality was high.
Case 1
This 81-year-old female patient visited our emergency room (ER) with comatose mentality, probably after slip down. She suffered from hypertension and diabetes. She has been taking wafarin after history of stroke. She had a fracture on her left humerus after a slip due to hypoglycemia 10 days before admission. Her GCS score was 7 (E1, V1, M5). Her pupils were reactive on the right side initially, however became bilaterally non-reactive, soon. CT scan revealed an acute subdural hematoma (Fig. 1A). Her family did not want to do surgery due to her age and frequent illness. When we used the best motor score, the IPMc, IPUc, IPMt (core+CT model), and IPUt were 54, 73, 45, and 65 respectively. She died on the next day.

CT scans of Case 1, 2, and 3. There are acute subdural hematoma with active bleeding (A), traumatic intracerebral hematoma (B), and acute subdural hematoma (C).
Case 2
This 80-year-old male patient was discovered on the road with comatose mentality. His GCS score was 7 (E1, V1, M5). His pupils were non-reactive on both sides. His vital signs were normal. There were no evidence of coagulopathy in the laboratory tests. CT scan revealed an acute traumatic intracerebral hematoma (Fig. 1B). His family did not want surgery. The IPMc, IPUc, IPUc, and IPUt were 70, 83, 60, and 76, respectively. He died on the next day.
Case 3
This 61-year-old male patient was transferred to our hospital with comatose mentality after falling. His GCS was 3 (E1, V1, M1). Pupils were non-reactive on both sides. Blood pressure was 60/30 mm Hg. He had a history of coronary angiography and received anticoagulant therapy. CT scan revealed an acute subdural hematoma (Fig. 1C). His family agreed to the do-not-resuscitate (DNR) order. The IPMc, IPUc, IPMt, and IPUt were 84, 91, 92, and 96, respectively. He died on the 3rd hospital day (HD).
Case 4
This 67-year-old male patient visited our ER with comatose mentality. He suffered from dementia. His GCS was 3 (E1, VT, M1). Pupils were both dilated. CT scan revealed a bilateral subdural hematoma (Fig. 2). After CT scanning, his respiration was ceased. A ventilator was applied. Although his family agreed to the DNR order on the 3rd HD, no one could remove the ventilator. The IPMc, IPUc, IPMt, and IPUt were 87, 89, 92, and 95, respectively. He died on the 13th hospital day (HD).
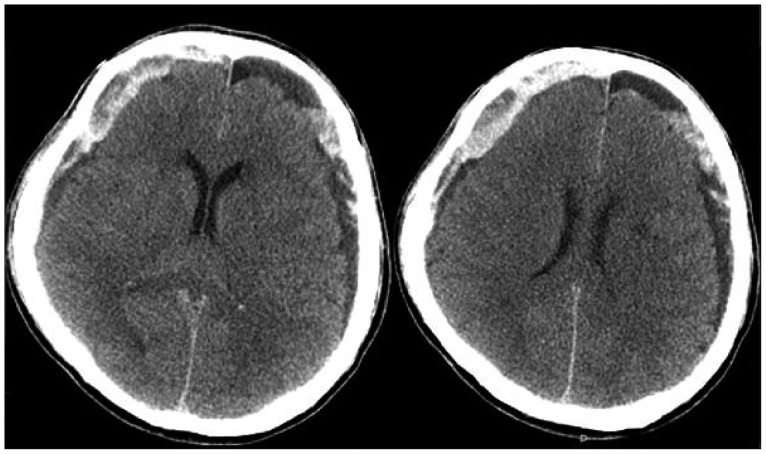
CT scans of Case 4. There are bilateral subdural hematomas.
Case 5
This 82-year-old male patient transferred to our hospital with comatose mentality. He suffered from hypertension and diabetes. His GCS was 4 (E1, VT, M2). Pupils were both dilated. CT scan revealed a huge subdural hematoma (Fig. 3). The IPMc, IPUc, IPMt, and IPUt were 91, 84, 98, and 96, respectively. His family refused surgical treatment. On the 3rd HD, his motor response became 4. We suggested an endoscopic burr-hole evacuation under local anesthesia. After surgery, the degree of midline shift was much improved (Fig. 3). However, his pupils were dilated and the motor score remained unchanged. His family refused any further treatment unless surgeons guaranteed his recovery. He was transferred to a nursing home in the vegetative state on the 8th HD.

CT scans of Case 5. Acute subdural hematoma was removed by endoscopic evacuation under local anesthesia.
Case 6
This 63-year-old male patient visited our ER with comatose mentality. He slipped down after drinking. His GCS was 4 (E1, V1, M2). Pupils were non-reactive on both sides. CT scan revealed an acute subdural hematoma (Fig. 4). The IPMc, IPUc, IPMt, and IPUt were 75, 90, 77, and 91, respectively. Decompressive craniectomy was performed (Fig. 4). He was discharged with a severe disability on the 17th HD.

CT scans of Case 6. Acute subdural hematoma was evacuated by decompressive craniectomy.
DISCUSSION
The most common surgical lesion was acute subdural hematoma in this study. Subdural hematomas became more frequent than epidural hematomas after the age of 50 years23). Since patients having any mass lesion with significant mass effect should be treated operatively, types of the mass lesion did not affect the surgical decision making in both groups. Although none of the motor score of 1 underwent surgery, motor score 2 or 3 did not preclude surgery. Contrary to the motor score, all patients with reactive pupils underwent surgery. Abnormalities in pupillary reactivity indicate brainstem compression and are strongly associated with poorer outcome3,14). Pupillary reactivity is a more stable variable in the early phase after injury than is the GCS, because it is less prone to influences of sedation and paralysis14). Even in patients with dilated pupils and GCS of 3, there is a chance of good outcome3). However, aggressive treatment is highly demanding and increases suffering for patients and their families and adds unnecessary medical burden4). The outcome was unfavorable in all five patients underwent surgery despite of dilated pupils, in this study. Pupillary response was a major factor of decision making. There is no age-dependent cut-off in brain injured patients. Most studies analyzed the association between age and outcome by use of threshold values, varying from 30 to 60 years of age14). Relatively high mortality begins from the age of 5513), 7012,24), 759,18), or 8019). Outcome following TBI in "younger elderly" (those less than 75 years old) can be comparable with younger adults with acceptable outcome15). It would be better that the life-saving, but not restorative, surgery is reserved for the so-called younger elderly patients with dilated pupils and GCS of 3.
All patients in the group A were expired. In case 4, a ventilator was applied before adequate discussion on the treatment with his family. In case 5, a decision was changed without any eventual benefit. A wrong decision may bring a long futile care. The decision is frequently made under pressure of time. Common reasons to justify withdrawal of life-sustaining therapy were a poor chance of survival, a prognosis incompatible with the patient's wishes and a poor long-term neurologic prognosis25). Some patients may consider death to be a preferable outcome to living in a permanent vegetative state or coma. In such situations, withdrawal of life-sustaining therapies may be the most acceptable option of care for families, relatives and medical teams according to patients' wishes and the philosophy of care25). If there is a prediction of an unfavorable outcome of >80%, a surviving patient is likely to remain severely disabled7). When the prediction of an unfavorable outcome is greater than 90%, we have an ethical obligation to at least enter into a discussion, not only regarding the likely outcome but also what would have been the patient's wishes9). Although removal of the ventilator can be ethically justified, it is hard to do. In Korea, the Supreme Court sentenced the doctor who permitted a moribund discharge to 1 year and 6 month in prison and 2 year probation6). Although the mean IPM and mean IPU of the group A were higher than those of the group B, the outcome was favorable in only 2 patients in the group B. A good decision may be more likely to lead to a better patient outcome, but outcome alone cannot measure the quality of a decision20).
Traumatic brain injury in the elderly has been and will be an important burden to the society with longer life expectancy and an aging population, with fall being the commonest cause. Increasing use of antiplatelet and anticoagulation medication is going to further complicate the condition16). In making the difficult decision about whether to proceed with a life-saving, but non-restorative procedure, surrogate decision-makers for the patients will need as much objective and reliable information as possible to make a truly informed decision8). Clear decisions can and should be made on the basis of straight and thoughtful communication between the senior staff member on call and the residents on duty21). Ethical training for neurosurgeons is to be encouraged21). To develop decision-making skills, there should be a supportive environment, with good supervision, mentoring, and role modeling20). Most medical problems can be treated in multiple different ways. Each treatment option offers different trade-offs in quality of life and mortality, and there is often no objective "best" treatment. Rather, a treatment choice should be made based on an individual's preferences and willingness to accept risk. The most consistent features about a surgical decision were that it was well informed and well considered20). A mathematical model22), while limited, does provide an accurate index of injury severity and may be useful in providing cause to pause and consider the long-term implications of life-saving but non-restorative surgical intervention8). Shared decision making, i.e., thorough discussion with predicted probability of unfavorable outcome is best used for problems involving medical uncertainty5).
CONCLUSION
Surgical decision making is difficult especially for the elderly patients with severe head injuries. Withholding a life-saving surgery was 15 times in 28 elderly patients with surgical lesions. There were wrong decisions, which brought futile cares. Ethical training and developing decision-making skills are necessary including shared decision making.