Neuroprotective Effects of Lacosamide in Experimental Peripheral Nerve Injury in Rats : A Prospective Randomized and Placebo-Controlled Trial
Article information

Abstract
Objective
To evaluate the neuroprotective effects of lacosamide after experimental peripheral nerve injury in rats.
Methods
A total of 28 male wistar albino rats weighing 300–350 g were divided into four groups. In group I, the sciatic nerve exposed and the surgical wound was closed without injury; in group II, peripheral nerve injuries (PNI) was performed after dissection of the nerve; in group III, PNI was performed after dissection and lacosamide was administered, and in group IV, PNI was performed after dissection and physiological saline solution was administered. At 7 days after the injury all animals were sacrificed after walking track analysis. A 5 mL blood sample was drawn for biochemical analysis, and sciatic nerve tissues were removed for histopathological examination.
Results
There is low tissue damage in lacosamide treated group and antioxidant anzymes and malondialdehyde levels were higher than non-treated and placebo treated group. However there was no improvement on clinical assessment.
Conclusion
The biochemical and histological analyses revealed that lacosamide has neuroprotective effect in PNI in rats. This neuroprotective capacity depends on its scavenger role for free oxygen radicals by increasing antioxidant enzyme activity.
INTRODUCTION
Peripheral nerve injuries (PNI) can occur due to mechanical, chemical, and thermal reasons. Trauma is the most common reason and it is known that PNI occurs in 2.8% of trauma patients [19]. Although there are several drugs, steroids and hormones, whose positive effects have been reported clinically and experimentally, recovery after PNI is still a clinical challenge [2,14,21,24,29]. However, unlike in the central nervous system, regeneration in the peripheral nervous system is possible but full functional recovery is often poor [9].
It is known that crush in peripheral nervous system results in damage of intraneural microcirculation by direct mechanical injury [16,31]. An inflammatory response strats and levels of free oxygen radicals increase which leads to further tissue damage. Lipid peroxidation and the level of tissue malondialdehyde (MDA) also increases which is a toxic process after PNI [12].
Therefore, several chemical agents with antioxidant and antiinflammatory effect have been evaluated for their ability to inhibit this cascade [3-5,11] Methylprednisolone and gabapentin are the reference agents and have shown beneficial effects in the literature [26]. But, although they have beneficial effects on parenchymal damage, there is no significant improvement on functional recovery and there are several side effects associated with their use [7].
Lacosamide may be another pharmaceutical candidate for treatment after PNI. Although it is an antiepileptic drug in clinical use, it has been shown to protect neurological tissue and have ameliorative effect on peripheral neuropathy. Several studies have reported that it exhibits antioxidant, anti-inflammatory and lipid peroxidation inhibiting effect which are the main scope of the treatment strategy for neural damage after PNI [1,13,22]. We have also reported in our previous study that lacosamide has neuroprotective effects after spinal cord injury [8]. So, when consider the anti-inflammatory, antioxidant, and inhibiting lipid peroxidation properties and protective effects of lacosamide on neural tissue after experimental spinal cord injury, we hypothesized that it may provide neuroprotective effects after traumatic PNI.
To the best of our knowledge, no study has reported on the use of lacosamide in an experimental PNI model. The purpose of this study was to investigate the effects of lacosamide after experimental sciatic nerve crush injury in rats using histopathological, biochemical and clinical methods.
MATERIALS AND METHODS
All the experimental procedures performed were approved by the Ethics Committee of Bingol University (date and serial number : 12.01.2017-796). A total of 28 male wistar albino rats weighing 300–350 g were divided into four groups of seven rats each. In group I (sham), the sciatic nerve exposed and the surgical wound was closed without injury; in group II, PNI was performed after dissection of the nerve; in group III, PNI was performed after dissection and lacosamide was administered, and, in group IV, PNI was performed after dissection and physiological saline solution was administered.
All rats were kept under environmentally controlled conditions and housed in separate cages during the test and were fed standard rodent food and water. They were anesthetized by intraperitoneal injection of 10 mg/kg of xylazine (Alfazyne, Egevet, İzmir, Turkey) and 50 mg/kg of ketamine (Ketalar, Parke-Davis, Eczacıbaşı, Turkey). The rats were placed in the prone position, and the surgical field cleaned with povidone iodine (Bathicon; Adeka, Samsun, Turkey). A skin incision was made on the left hip of the rats and the sciatic nerve within the gluteal muscle exposed. The surgical wound was closed without PNI in group I. After the same procedure for approach to the sciatic nerve, a vascular clip (Vascu-Statt®; Scanlan, St. Paul, MN, USA) with 40 g closing force was applied to the sciatic nerve for 1 minute which was sufficient to cause mild to severe damage and the crush injury achieved in group II (Fig. 1), and then the wound was closed [17]. Lacosamide was administered intraperitoneally at a dose of 30 mg/kg by 8 hours intervals after PNI in group III. The first dose of drug administered immediately after closing the skin and the last dose administered 8 hours before the sacrification and, serum physiologic was administered at the same dose and the same interval in group IV after PNI.
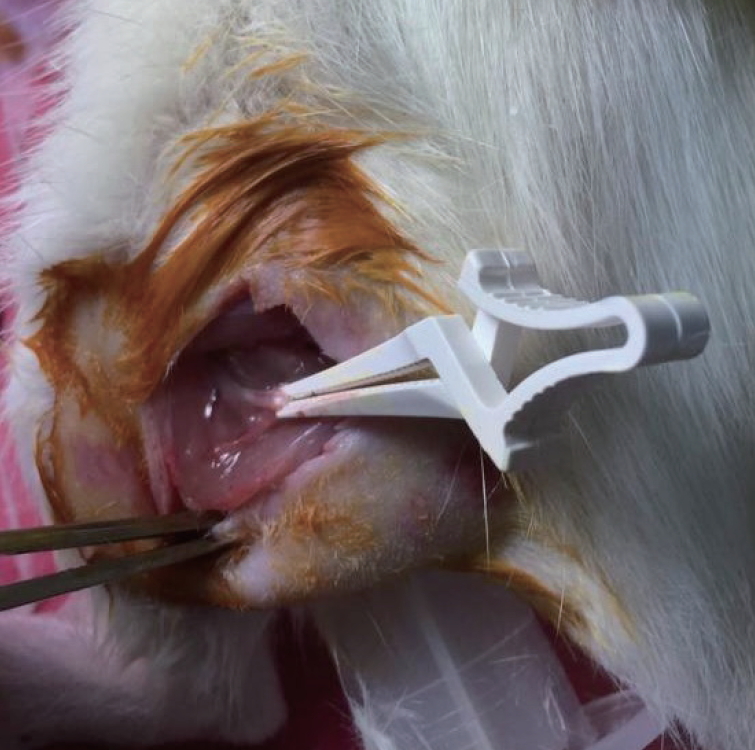
Compression of the sciatic nerve with a clamp with 40 g closing force.
At 7 days after the injury all animals were sacrificed after walking track analysis by decapitation under deep anesthesia and autopsy performed according to the Virchow technique. A 5 mL blood sample was drawn for biochemical analysis, and sciatic nerve tissues were removed for histopathological examination. Blood samples were centrifuged at 1500 rpm for 15 minutes to obtain serum, and serum samples were stored at -40°C before analysis of the glutathione peroxidase (GPX), superoxide dismutase (SOD), catalase, and MDA levels by using a commercial enzyme-linked immunosorbent assay kit (SunRed, catalog numbers SOD : 201-11-0169, GPX : 201-11-5104, catalase : 201-11-5106, MDA : 201-11-0157).
The sciatic nerve tissues were fixed in 10% neutral-buffered formalin for 48 hours, immediately upon removal. The tissue samples were processed as routine protocol of dehydrated in ascending grades of ethanol (50%, 70%, 96%, and 100%), cleared in xylene and then embedded in paraffin. Paraffin embedded tissue samples sectioned at 5 µm thickness by rotary microtome. The slides were stained with hematoxylin & eosin and Masson Trichrome (with aniline blue) kit (Bio-Optica, Milano, Italy) for histological examination. Finally the slides were examined and photographed by using light microscope with imaging system (DM2500/DFC295; Leica, Wetzlar, Germany). The histopathological findings and classifications of nerve tissue injury examined by using light microscopy and were scored according to the classification of nerve injury by Seddon [25] and Sunderland [27] and were assessed in a blinded analysis technique by a pathologist (Table 1). The classifications of sciatic nerve tissue injury were determined and scored by microscopically examination of neurapraxia, axonotmesis and neurotmesis in the distal segment of the injured sciatic nerve tissue area with 20 and 40× objectives.

The classification of nerve injury by Seddon and Sunderland
Walking track analyses were performed before the sacrification using stamp and paper method. The lengths of the third toe to heel (PL), first to fifth toe (TS), and second toe to fourth toe (IT) were measured on experimental (E) and normal sides (N) and sciatic function index (SFI) was calculated by using the following formula :
SFI = −38.3 × (EPL − NPL) / NPL + 109.5 × (ETS − NTS) / NTS + 13.3 × (EIT − NIT) / NIT − 8.8
SFI score 0 represents normal nerve function and −100 total dysfunction [20,23].
All data were analysed using the SPSS ver. 20.0 software package (SPSS Inc., Chicago, IL, USA). The Mann-Whitney U test was used to compare the descriptive statistical measurements (mean, standard deviation, minimum and maximum) and the two groups of parameters that did not show a normal distribution in the quantitative data comparison. One-way analysis of variance was applied to assess the differences among the groups. Significance was evaluated at p<0.05.
RESULTS
The PNI and SFI scores and the serum GPX, SOD, catalase, and MDA levels are shown in Table 1. PNI score was similar in group II and group IV, and PNI score in group III was lower than group II and group IV and the difference was statistically significant (p<0.05).
The MDA levels, which is also indicator of tissue damage, were parallel to the PNI score. It was minimum in group I and maximum in group II and there is a statistically significant difference between group III and all other groups (p<0.05).
All of the antioxidant enzyme levels, catalase, GPX and SOD, were also parallel to the each other. They were higher in group III than all other groups and, group II and group IV have similar results. The differences were statistically significant between group III and all other groups (p<0.05).
The SFI score, which is a clinical assessment, was lower in group I than the other groups and similar in groups II, III, and IV (p>0.05).
When we look at the histopathological results, in group I (sham); in the evaluated sciatic nerve tissues, no significant histopathological differences were noted and the sciatic nerve tissues were showed normal histological structure (Fig. 2A and B). It has been observed that In the group II, common lesions in the distal segment of injured sciatic nerve tissues are as the following; diffuse and severe spongious appearance (axonal demyelination), axons and endoneurial tubes discontinuity, perineurium and fascicular arrangement preserved (axonotmesis-third degree) was monitored in nerve fibrils, and congestion of blood vessels in perineurium and epineurium. Diffuse Schwann cell proliferation which digested myelin, infiltration and increasing of phagocytic cells in the perineurium and between the nerve fibers were seen. Increase of the number of Schmidt-Lanterman incisures was remarkable in the some myelin sheaths (Fig. 2C and D). Axonotmesis (2nd and 3rd degree) findings related to peripheral nerve injury were also detected in the group-III (Fig. 2E and F) and group IV (Fig. 2G and H) and these findings were similar to the findings in the group II, except the detected finding that regenerative changes (inflammatory cell infiltration in epineurium) and Schwann cell activation in group-III were observed more intense. The histopathological changes detected in the sciatic nerve scored according to the groups are given in the Table 2.
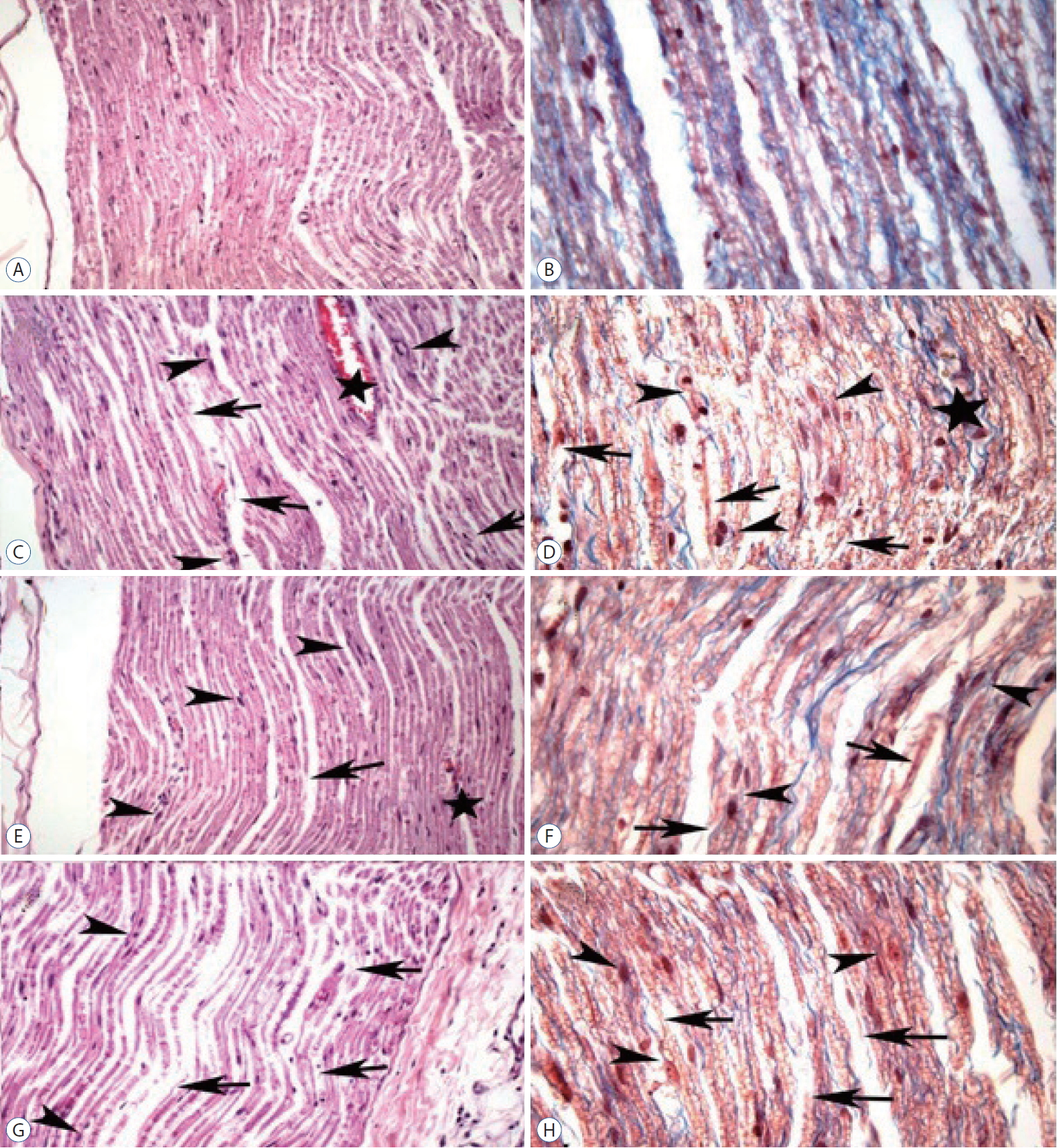
Histopathology of sciatic nerve tissues; H&E staining with 20× (A, C, E, and G) and MT staining with 40× magnification (B, D, F, and H). A and B : Normal histological structure of sciatic nerve in group I. C and D : Proliferated and activated Schwann cells (arrowheads), segmental demyelinated nerve fibers (arrows) in group II. Proliferated and activated Schwann cells (arrowheads), axonal demyelination, axonal and endoneurial discontinuity (arrows), congestion of blood vessel in perineurium (star) in group III (E and F) and in group IV (G and H).

Biochemical result and pathological and clinical scores relevant to the groups
DISCUSSION
In the current study, we had similar results to our previous study (lacosamide treatment after spinal cord injury) [8]. Histopathological results represented that there is lower damage in group III which was treated with lacosamide when compared with the others. Furthermore, the lipid peroxidation endproduct MDA levels were lowest and the antioxidant enzymes catalase, SOD, and GPX levels were highest as a result of lacosamide treatment which also explain the reason of low damage. Different from the study on spinal cord injury, there is a clinical evaluation in the current study which showed similar results in all groups.
Peripheral nerve injury may results from compression, focal contusion, traction or transection of the nerve. After first trauma, it is followed by ischemic injury, inflammation, oxidative stress and then nerve injury occurs [10]. Free oxygen radicals which are produced during this period reponsible from oxidative stress and lipid peroxidation so responsible from tissue injury. Therfore, prevention of inflammation and protection against free radical-mediated oxidative stress and lipid peroxidation are the main therapeutic strategies for the treatment. For example, the neuroprotective effect of methylprednisolone, which is a reference drug for the treatment of PNI, depends on its scavenger role for free oxygen radicals and its ability to inhibit lipid peroxidation and inflammation.
The balance between oxidants and antioxidants is critical to maintain normal cellular functions. If the oxidative stress outweighs the cellular antioxidant activity, it results in tissue injury [30]. GPX, SOD, and catalase are some of the antioxidant enzymes that protect against oxidative stress by inhibiting the production of free oxygen radicals. SODs catalyse the breakdown of the superoxide anion into oxygen and hydrogen peroxide. GPX reduces hydrogen peroxide and lipid peroxide to water and lipid alcohols. Catalases are also enzymes that catalyse the conversion of hydrogen peroxide to water and oxygen. If the activity of these enzymes is decreased, the amount of free oxygen radicals increases or vice versa. So, after trauma, these enzymes are expected to increase to protect the body. Choi et al. [6] reported increases of catalase and GPX expression after lacosamide pretreatment in experimentally induced transient cerebral ischaemia in gerbils and emphasised the neuroprotective effect by this increased antioxidant activity. In current study, there was also an increase in GPX, SOD and catalase in group III (Table 2). These results indicate the neuroprotective effect of lacosamide resulting from increased antioxidant enzyme activity.
Lipid peroxidation is another crucial step in the tissue injury after trauma [13,15]. Free oxygen radicals damage membrane lipids and alter membrane fluidity and permeability which results in cellular dysfunction [30]. MDA is the final product of these reactions and widely used as a marker of tissue injury. Solmaz et al. reported the potential lipid peroxidation-inhibiting effect of lacosamide on rats in a study on sepsis-induced critical illness polyneuropathy [28]. Although sepsis and trauma are two different conditions, lipid peroxidation plays an important role in the ethiopathogenesis of both. Therefore, we suggest that lacosamide, which reduces lipid peroxidation, also has a protective effect in SCI. Consequently, the decrease in MDA serum levels was an expected result in group III and supports our hypothesis of a neuroprotective effect of lacosamide in PNI.
In clinical assessment according to the walking track analysis in groups II, III, and IV, all rats had similar SFI scores. There was no effect of lacozamide in functional recovery. We think that one week follow-up, which can be a limitation for this study, may not be enough for the assesment of clinical effectiveness. Ozbek et al. [18] observed significant motor improvement at 4 weeks after treatment after experimental peripheral nerve injury in rats.
CONCLUSION
In conclusion, this is the first study to investigate the neuroprotective effects of lacosamide after PNI. The biochemical and histological analyses revealed that lacosamide has neuroprotective effect and may be useful in the treatment of PNI. However, studies with long follow-up are needed to clinical assessment.
Notes
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization : SD
Data curation : SD, KU
Formal analysis : ASB, AU
Funding acquisition : SD, SE
Methodology : SD, KU
Project administration : SD, SE
Visualization : YA, AC
Writing - original draft : SD, KU
Writing - review & editing : SD