INTRODUCTION
Carpal tunnel syndrome (CTS) is a clinical condition by the compression of median nerve in the carpal tunnel. Not only CTS has various etiologies, but it is the most common in the compressive entrapment neuropathy, and dominant in women (5.8%) than in men (0.6%), especially in the middle-aged housewives12,17). Its symptoms are sensory dominant, including pain and tingling sensation in the thumb, index, and middle finger or hand stiffness at night primarily, tingling sensation of finger tips, not entire hand. Atrophy in the thenar muscle also can be seen in some cases17,18). The diagnosis of carpal tunnel syndrome is based on clinical criteria such as history taking and physical examination and then followed by electrodiagnostic evaluation such as nerve conduction study (NCS) and electromyography (EMG), and sonography of carpal tunnel to confirm diagnosis. Previous physical examinations such as Tinel's test, Phalen's test, and carpal compression test need skillful examiners to reproduce CTS symptoms, the result of those tests can be variable according to skills of examiners not only sonography and electrodiagnostic evaluation are expensive initial tools of diagnosis for CTS, but also those diagnostic tools need more skillful examiners and the latter is invasive test to patients. Therefore the test we need is, easy to perform, reproducible, not invasive, and having high sensitivity and specificity. This study was carried out to establish the utility of hand elevation test as most accurate, easy to perform, reproducible, cost effective and not invasive test to diagnose the CTS.
MATERIALS AND METHODS
We prospectively studied 45 hands of 38 patients diagnosed with CTS between April 2005 and February 2009. Control group was set 45 hands of 45 asymptomatic persons. The American Academy of Neurology clinical diagnostic criteria was the basis of diagnosing the CTS13,21). Detailed history taking was performed to each patient with same questionnaire, followed by provocation tests. Each test was performed in the same physical sign with two minutes interval. The order was hand elevation test followed by Tinel's test, Phalen's test, and carpal compression test. The hand elevation test was performed by just elevating both hands above the head and maintaining in position until patient felt paraesthesia, numbness and dull pain in the median nerve territory. Test result was positive if symptoms occurred in 2 minutes. Tinel's test was performed by tapping the median nerve at the wrist, and this was repeated four to six times. The presence or absence of radiating pain or paraesthesia in the median nerve distribution was recorded. Phalen's test was executed by asking each subject to hold hand with the wrist in complete palmar flexion with elbow extended and forearm pronated. The test was considered positive if symptoms were reproduced in 1 minute. Carpal tunnel compression test was conducted by the examiner compressing between thenar and hypothenar eminence for 30 seconds with the patient's arm supinated. The test was considered positive if symptoms were reproduced in thirty seconds. After four provocation tests, NCS, EMG and ultrasonography were used as the absolute diagnosis. Chi-square test statistics was used to compare the sensitivity and specificity between hand elevation test and the three other test.
RESULTS
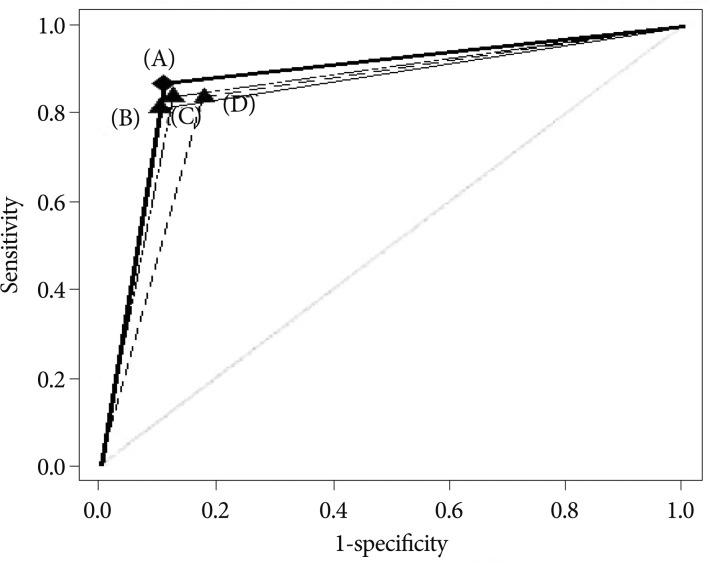
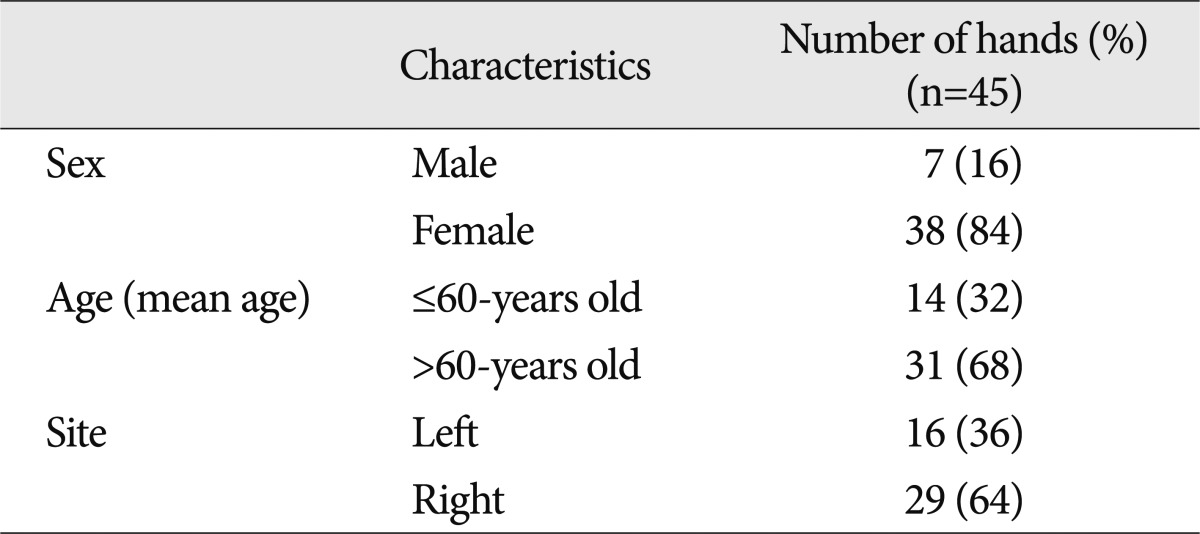
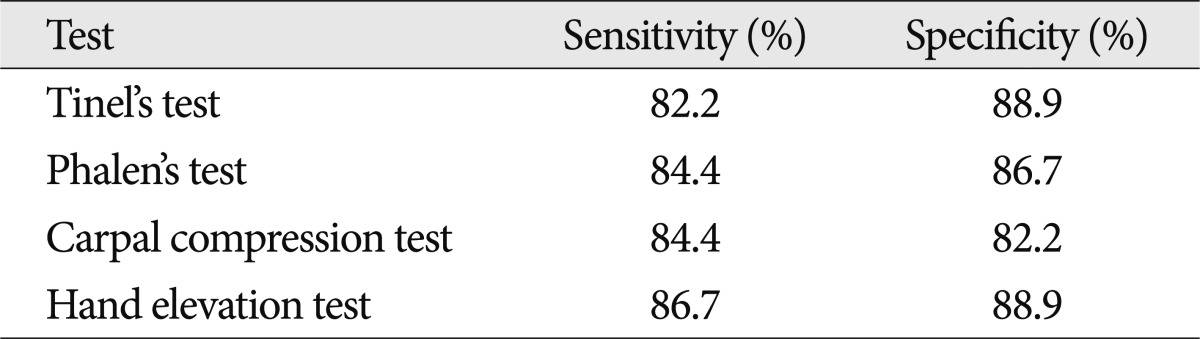
In the experimental group, their mean age was 56.9 (range 48-64) years old. Seven (15.5%) hands were hands of male and thirty eight (84.5%) hands were hands of female. Sixteen hands were left side and twenty nine hands were right side (Table 1). In the control group, mean age was 56.8 (range 48-64) years old. Seven (15.5%) hands were hands of male and thirty eight (84.5%) hands were female. Sixteen hands were left side and twenty nine hands were right side. The sensitivity and specificity of the hand elevation test was 86.7% and 88.9% each. Tinel's test had sensitivity of 82.2% and specificity of 88.9%. Phalen's test had sensitivity of 84.4% and specificity of 86.7%. Carpal compression test had sensitivity of 84.4% and specificity of 82.2% (Table 2). The difference of sensitivities of the hand elevation test, Tinel's test, Phalen's test, and carpal compression test was not significant (Table 3, 4, 5). It means no significant difference in sensitivity between hand elevation test, the three other tests. The difference of specificities of the hand elevation test and the three other tests was not significant (Table 6, 7, 8). It suggests no significant difference in specificities between hand elevation test and Tinel's test, Phalen's test, and carpal compression test. To compare the diagnostic accuracies of each test, the area under the non-parametric receiver operating character (ROC) curve was applied. ROC analysis is a method to compare the results of various tests and to evaluate the diagnostic accuracy of a test for the same outcome. ROC curve is a plot of the sensitivity (true-positive) against 1-specificity (false-positive) over all values available. So it can evaluate the balance between sensitivity and specificity of a diagnostic test over a variety of cutpoints. Simply, larger area under curve indicates high accuracy2,20). Hand elevation test had 0.878 area under the ROC curve (95% CI 0.792-0.937). Tinel's test had 0.856 area under the ROC curve (95% CI 0.766-0.921), Phalen's test had 0.856 area under the ROC curve (95% CI 0.766-0.921). Carpal compression test had 0.833 area under the ROC curve (95% CI 0.740-0.904) (Fig. 1). Although there are no significant differences in sensitivity and specificity between hand elevation test and the three other tests, hand elevation test is not less significant compared with Tinel's test, Phalen's test and carpal compression test, as hand elevation diagtest has higher sensitivity and specificity at least.
DISCUSSION
Carpal tunnel syndrome is most common peripheral compressive entrapment neuropathy occurred by the compression of median nerve in the carpal tunnel, and its incidence is 1% of the population and is on an increasing trend in especially workplace6,12,15). The pathophysiology of carpal tunnel syndrome is not clear. There is a hypothesis that entrapped carpal tunnel increase nerve compression pressure and may cause ischemia of microcirculation of the nerve by compressing the vessel in perineurium4,8,14). CTS is considered as sensory disorder mainly, because the sensory fibers can be affected than the motor fibers9). So patients with CTS complain of sensory symptoms such as dull pain and tingling sensation in the thumb, index, and middle finger or paraesthesia and stiffness of hand at night primarily, tingling sensation of finger tips, not entire hand. Atrophy in the thenar muscle, weakness or clumsiness of hand, dry skin, swelling or color change in the hand also can be seen in some cases17,18,21). And if there is mitigating factors such as changes in hand posture or shaking the affected hand to relief pain, they result in contracture and degeneration of the epineurium and endoneurium of the median nerve19). If the hypothesis of ischemic attack to median nerve is related to pathophysiology of CTS, hand elevation above the shoulder may be the cause of ischemia of median nerve. But, literally, CTS is syndrome, not single disease. Many conditions are associated with CTS and that is why there is no single gold standard test22). The diagnosis of CTS is very difficult and can be controversial. CTS can be diagnosed by history, clinical physical examination and confirmatory studies. Confirmatory studies such as EMG and NCS can be helpful in diagnosis of CTS but they are expensive, invasive and can't be conducted in all local medical center. To date, Phalen's test, Tinel's test have been used as diagnostic criteria in physical exam21). However, the result of each test depends on physician's examination skill. And confirmatory studies such as EMG and NCS have low sensitivity and specificity to diagnose the CTS1,3,5,11). Recently, carpal compression test has been used to diagnose the CTS. There were many evaluations of sensitivity and specificity of carpal compression test. To make matters worse, the sensitivity and specificity of the carpal compression test depends on physician's examination skill, too1,7,10,16,23,24). Therefore simple to perform, reproducible, cost effective, sensitive and specific physical examination to diagnose the CTS is in need. Hand elevation test has several advantages to diagnose the CTS. First, physician's examination skill is not needed to perform hand elevation test. Secondly, it is very simple, just hand elevating above the shoulder in the air freely and waiting for the occurrence of symptoms of CTS is the demand. And finally, it is cost effective, and can be performed within two minutes of short examination time. Post operation patients checking needs only hand elevation, actively or passively. Even if there is no statistically significant differences in sensitivity and specificity between hand elevation test and the three other tests, but it is still showing more sensitivity and specificity than the three other tests according to the study.
CONCLUSION
The hand elevation test can be performed by just elevating patient's both hands above the shoulder in the air freely. It is simple, reproducible, cost effective, sensitive and specific to diagnose the CTS. It can be used to physical examination of choice, and can be employed first order provocation test instead of Tinel's test, Phalen's test, and carpal compression test.