INTRODUCTION
Major postoperative complications in intracranial lesions have greatly reduced with the introduction of modern neurosurgical devices and microsurgical techniques. However, cerebrospinal fluid (CSF) leakage after craniotomy occurs not infrequently and has continued to be the significant cause of minor postoperative complications such as wound dehiscence, local infection and meningitis. Most of the complications are well cured but in some cases, failure in infection control not only leads to prolonged hospitalization but also affects the patient's quality of life. To prevent these complications, various techniques such as the use of fibrin glue, preparation of galeal or pericranial flaps and prophylactic lumbar drain have been described3,11,16,17). In this study, we introduce a surgical technique, so called "galeal tack-up suture" for the prevention of CSF collection in subgaleal space.
MATERIALS AND METHODS
This study included 87 patients who underwent craniotomy for various lesions such as brain tumor, vascular and traumatic lesions from December 2012 to May 2013. The patients were randomly allocated to either one of the two groups, the wound closure with "galeal tack-up suture" (group A) or routine wound closure (group B). There were 32 patients in group A and 55 patients in group B. We prospectively compared the frequency of postoperative subgaleal CSF collection in two groups until the wound has been stitched out. All minor subgaleal CSF collections which could be easily cured by compression with elastic bandage were also included.
Surgical technique of galeal tack-up suture
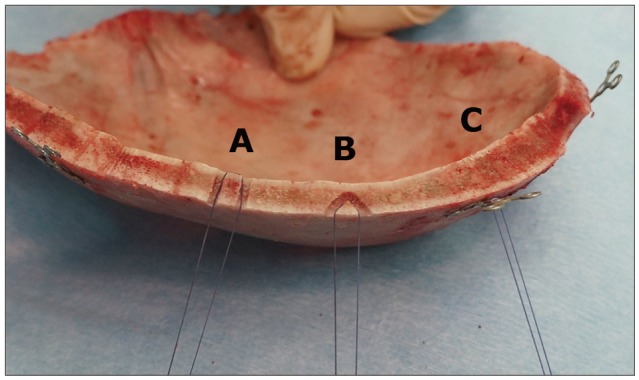
In all patients, dural closure was done by interlocking or continuous suture method. Routine dural tack-up sutures are placed at the craniotomy margin to hold the dura against the bone edge in attempt to prevent postoperative epidural hematoma. Dural CSF leak was checked with intraoperative Valsalva maneuver in all cases to ensure the water-tight dural closure. After the bone flap has been fixed with cranial plate, central dural tenting suture passing through the small holes burred previously was made, to fix the dural flap to the bone flap. Upon closing the scalp, one of the three methods of "galeal tack-up suture" was used (Fig. 1).
First method of "galeal tack-up suture" utilizes the pairs of small hole burred for central dural tenting suture. 4-0 vicryl attached to curved needle is passed through the hole from external side of bone flap to internal side, and then passed to external side again through the adjacent hole. For second method, pairs of V-shaped holes are burred on the surface of bone flap but not piercing through it. Third method utilizes the cranial plate used to fix the bone flap. Single piece of straight titanium plate can be installed independently to be used as an anchor. This anchor is especially useful in cases of suboccipital craniotomy or foramen magnum decompression where making of holes directly (straight or V-shaped) is difficult.
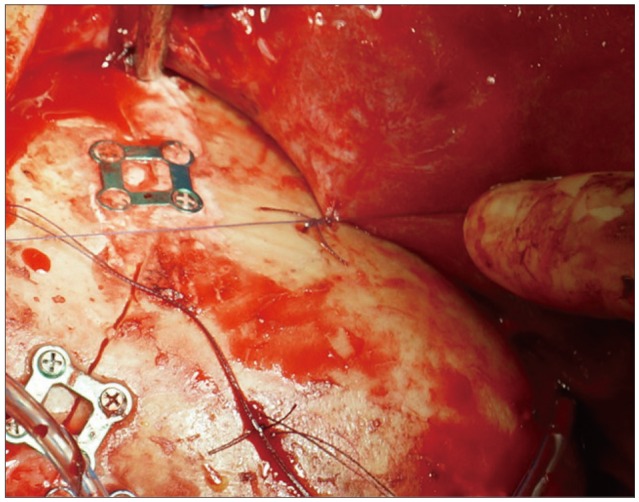
Three to five suture materials are prepared depending on the size of the bone flap. While closing the scalp in layer by layer fashion, galea aponeurotica is sutured with the bone flap using the previously prepared sutures (Fig. 2).
RESULTS
A total of 87 cases of craniotomy for intradural lesions were done in 75 patients. Six patients underwent repeated surgery for brain tumor, one of them for three times. Two patients underwent revision surgery for persistent CSF leakage, 1 patient underwent revision surgery for subdural empyema, and 2 patients underwent cranioplasty for craniectomy state in which dural tearing occurred while dissecting due to dura-galeal adhesion. There were 35 males and 40 females with mean age of 49 years old (range : 1-82). Intradural lesions included 32 cases of vascular lesion, 36 cases of brain tumor, 13 cases of trauma, 3 cases of congenital lesion, and 3 cases of infection (Table 1). Galeal tack-up suture was performed in 32 cases and routine wound closure without galeal tack-up was done in 55 cases. The three different galeal tack-up suture techniques were applied according to the size, location, and shape of the bone flap where it is appropriate.
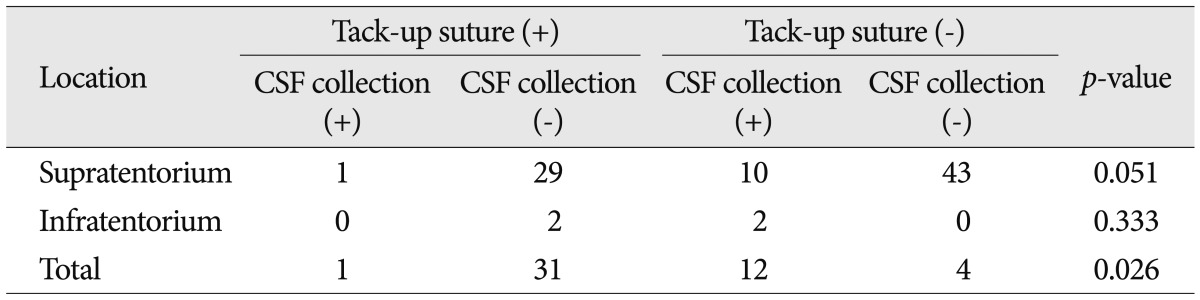
Subgaleal CSF collection occurred in 13 (15%) of 87 cases. The frequency of subgaleal CSF collection was higher in infratentorial lesions (50%). Twelve cases occurred in group B patients where only routine wound closure was done and there was 1 case of postoperative CSF collection in group A patients with galeal tack-up suture. In supratentorial lesions, galeal tack-up suture tended to be effective (p=0.051) but was not proven statistically significant. However, galeal tack-up suture applied in total sum of cases showed significant value statistically (p=0.026) (Table 2). Among 13 patients with subgaleal CSF collection, 8 patients were treated with percutaneous aspiration followed by compression with elastic bandage and 1 patient with lumbar drain. In 4 patients, routine treatment has failed to stop subgaleal CSF collection so revision surgery had to be done. There was no statistical significance between age (p=0.401), sex (p=0.154) and the incidence of subgaleal CSF collection.
DISCUSSION
Postoperative CSF leakage frequently results in CSF pooling in subgaleal space. CSF collected in subgaleal space can be diagnosed by several methods such as brain computed tomography, magnetic resonance imaging but it can also be detected by simply touching the operation site which feels like water-filled balloon8). It is usually considered one of the minor postoperative complications but if left untreated, it can cause severe brain infection such as meningitis14). It also results in prolonged hospital stay, increased treatment costs, and revision surgery in some cases12,14). Several methods have been reported for the treatment of CSF collection. Usually, it can be treated by bed rest with head elevation, percutaneous aspiration followed by compression with elastic bandage, and installation of lumbar drain but sometimes requires repeated surgery for CSF fistula6,9,14). Percutaneous aspiration and lumbar drain can also result in intracranial infection. It has been accepted that careful watertight dural closure is imperative procedure for prevention of postoperative CSF leakage after the operation for intradural lesion1,2,13). Application of fbrin glue on the dural suture line has also been known to be effective measure for prevention of postoperative CSF leakage10,15,17). But even with all the preventive measures, some cases of CSF leakage incurs in the operation for intradural lesions. Grotenhuis5) reported that in the series of 412 patients of nontraumatic neurosurgical cases, postoperative CSF leakage occurred in 44 (10.7%) patients including self-limiting subcutaneous minor CSF collection. Kwon et al.7) reported that in the series of 47 cases which underwent orbital roof craniotomy and superolateral orbital craniotomy, 13 (27.6%) cases of periorbital CSF collection had occurred.
CSF leaks through the dural suture lines and defects which were failed to close properly during the operation. Leaked CSF is pooled in epidural and subgaleal spaces and disrupts the adhesion between galea and cranial vault by creating dead space filled with CSF. Routine dural tenting suture are performed to prevent epidural hemorrhage. It can also prevent leaked CSF to pool in the epidural space. By performing galeal tack-up suture, single large subgaleal space is removed and divided into small multiple subgaleal spaces and galea becomes tightly adhered to the cranial vault which prevents CSF to pool. Goel4) previously described 'Tenting' stitches for the scalp can effectively reduce subgaleal collection of CSF in 1991. They utilized pericranium-galeal tenting but we did not use it since the technique is more difficult than galeal-cranium tenting and also the suture strength is weak. Kato et al. reported a CSF leak rate of 0.5% by using galea-cranium suture method in their technical note in 1999. They utilized v-shape holes and plate but the clinical data was not suggested. Among the surgical techniques suggested in the two technical reports, we chose the appropriate methods to apply in clinical setting and the results were statistically analyzed. Our study indicated that galeal tack-up suture is an effective and easy-to-perform technique for prevention of postoperative subgaleal CSF collection which does not require additional costs.
All three techniques are essentially the same that aims to attach galea to the cranium and remove the space for CSF to pool. These different techniques can be chosen and applied in most of the craniotomies with different size, shape, and location of bone flaps where it is appropriate.