INTRODUCTION
Autonomic dysreflexia (AD) is a well known condition of an uncontrolled sympathetic output, that generally occurs in patients with spinal cord injury (SCI) who have a lesion above T6 spinal level1). AD is caused by spinal reflex mechanisms that remain intact despite the injury of the spinal cord. In SCI patients, blood pressure levels can fluctuate easily. Orthostatic hypotension and hypertensive attacks influence greatly the quality of life of these patients. In addition, the hypertensive attacts can be life-threatening by causing end organ damage14). Central nervous system complications are uncommon but it may be the most common reason of morbidity and mortality. AD is an important clinical diagnosis that requires prompt recognition and treatment in order to avoid this devastating complications.
AD is often triggered by noxious stimulus below the level of the SCI. Most important aspect of the management of AD is prevention, early recognition and removing of the triggering factors. In particular, the urinary tract obstruction and fecal impaction, which are the most common triggers of AD, must be checked out urgently and regularly.
Here, we report a SCI patient who had a rare hypertensive cerebral hemorrhage complication during an AD episode and we discuss the pathophysiology and the treatment methodes of the AD.
CASE REPORT
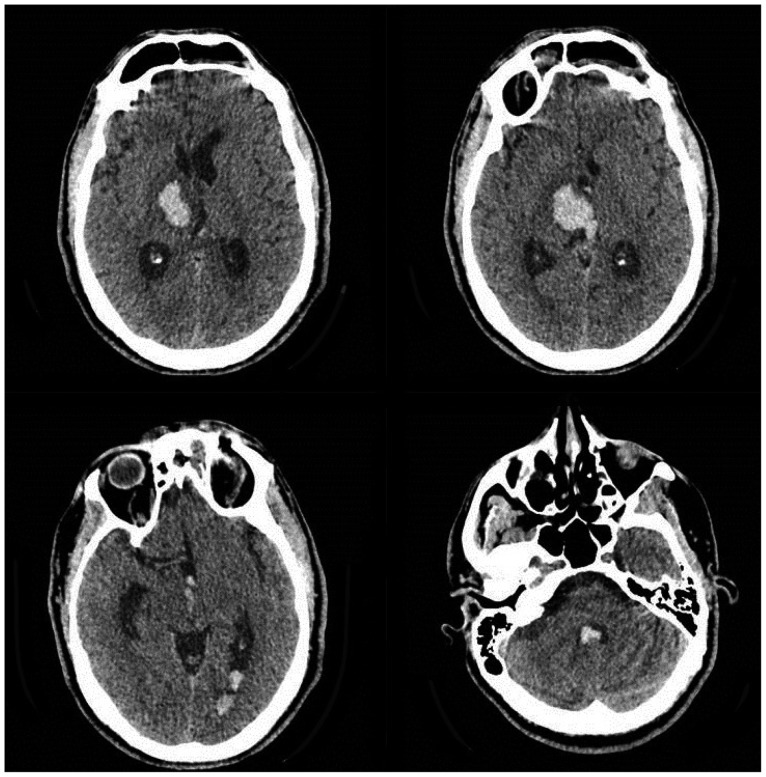
The patient was a 43-year-old man who had a American Spinal Injury Association Impairment Scale-B (ASIA-B) type incomplet SCI at level C6 secondary to a traffic accident for three years (Fig. 1). He was under a physiotherapy programme for his quadriparesis. He had been diagnosed with autonomic dysreflexia due to the hypertensive attacks which were followed with hypotension and bradicardia. His neurogenic bladder was initially managed with an indwelling foley catheter and then clean intermittent catheterisation for two years. Because of persistant attacks, suprapubic catheterization with cystofix has been performed one year ago. The patient admited to our emergency department with letargy, left sided facial paresis and worsening in his paresis in the left upper extremity. His family described the history of cystofix dysfunction with abdominal distention and increasing in blood pressure up to 220/100 mm Hg right before these symptoms. His cranial CT revealed right thalamic and inraventricular hematoma with 21 mm3 in volume (Fig. 2). He has been followed-up with medical treatment and his cystofix catheter had been replaced with a wider one. Afterward, there were no additional AD attackd. He became alert and his nascent motor defisit on his upper extremity improved completely.
DISCUSSION
AD is a common complication of high level spinal cord injury. Although it is common in SCI, non-traumatic diseases such as multiple sclerosis and spinal cord tumor can also be the cause of AD2). AD mainly occurs in chronic stage of disease both in the complete and the incomplete injury group1).
The pathophysiology of AD is related with the disconnection of the spinal sympathetic centers from supraspinal control. Normal regulation of sympathetic output from the spinal cord is modulated by input from the higher centers. After SCI, this system is no longer retain by descending control1). The development of AD after injury is a multifactorial complex issue. Degenerative and plastic changes within the injured cord play the main roles. These changes are thought to occur because of the synaptic re-organisation and reduction in gliosis around the pre-synaptic sympathetic neurones2,5,14). As a result of this process, exaggerated reaction occurs within the sympathetic pre-ganglionic neurones as a response to the afferent stimulus. The reason that AD is a feature of lesions at or above the T6 level is related with splanchnic circulation response to this sympathetic overactivity. Overactivity below the injury level results with splanchnic and peripheral vasoconstriction and causes hypertension. The excessive parasympathetic output (and lack of sympathetic tone) above the level of the lesion results with peripheral vasodilation. Hence, patients experience sweating, nasal congestion, flushing and bradicardia. In brief, AD result from the parasympathetic excitation above the level of injury, and sympathetic excitation below the level of injury and clinically it is characterized by an acute increase in blood pressure, headache, sweating, facial flushing and bradicardia1,2,5,11). We must always be aware of and search these features during the SCI patients follow up.
This AD crisis may lead to injuries in cardiac, pulmonary, retinal and renal tissues16). Uncommonly, this hypertansive crises may also effect central nervous system by causing cerebral hemorrhage10,12,13,14,15,16) and more rarely posterior reversible enchephalopathy syndrome (PRES) or reversible cerebral vasoconstriction syndrome3,7,13). Central nervous system involvement is very rare and if occurs, it is most commonly asymptomatic. But, it can also result in altered mental status, local neurologic deficits and seizures4,16). Intracranial hemorraghe is an uncommon complication of AD but fatal cases with massive bleeding have also been reported6,8,10,13,17). Here, we report a rare sypmtomatic cerebral hemorrahge which is result from an AD attack.
Physicians should repeatedly check and note the neurologic status of every SCI patient even during chronic stage because it may be difficult to distinguish the new neurologic findings in this tetraparetic or tetraplegic high level SCI patients.
The main triggering factor of AD is related with the urinary tract. Blocked or kinked indwelling urinary catheters are one of the most common causes. Choosing the safest and appropriate method for the patients and family education for controlling the function of the catheter are the important issues. The goal in all bladder treatment is the creation of a balanced bladder, with low intravesical pressure that is drained totally at regular intervals and is free of urinary tract infections. In patients with SCI, clean intermittent catheterization has been recommended rather than indwelling urinary catheters if the patient and family can adjust9).
There are also many other urological causes for AD like bladder distension, urinary tract infection, bladder or kidney stones, urologic procedures, detrusor sphincter dysinergia, epididymitis or scrotal compression. The second most common causes of AD due to SCI are gastrointestinal problems, including faecal impaction and rectal distension also anorectal conditions like haemorrhoids and fissures. Orthopedic conditions such as fractures, dislocation, heterotopic ossification and general surgical conditions of the abdominal organs, such as appendicitis, gastro-oesophageal reflux, and peptic ulceration may presipitate the AD. Bed wounds, skin ulceration or ingrowing toenails may be the dermathologic triggering factors. Female patients also have higher risk for developing AD during pregnancy and labour1,2,5). All of these triggering factors must be kept in mind during evaluation of a patient with AD.
The first step of the treatment of AD, regardless of the cause, is to make patient sit in an upright position to maintain an orthostatic decrease in the blood pressure. Main treatment is removal of the triggering factors. Antihypertansive drugs are rarely needed. If needed, the calcium antagonists or adrenoceptor blockers may be beneficial in the treatment of AD1,2,5).
This life-threatening complication should be kept in mind in the patients, especially with upper SCI. The medical team who are dealing with SCI patients as well as the SCI patients themselves and their relatives should be aware of this disorder and apropriate bladder care, bowel exercises and skin care should be provided.
CONCLUSION
This case has been reported to emphasises the rare hypertensive cerebral hemorrhage complication during common AD episodes in SCI. Clinicians should always closely monitore the patients with SCI, especially those in the high spinal levels. These patients can easily develop AD which is triggered by the stimulation of lower parts of the body. Our patient had a common triggering factor; urinary drainage malfunction. Prompt removal of the triggers and choosing the safest urinary drainage method are very important to save the patients from the complications of AD.