INTRODUCTION
After craniotomy for aneurysmal clipping, the intracranial vessels are examined for any residual neck, parent artery compromise, vasospasm, or aneurysmal regrowth. As the standard tool for intracranial vascular examination, digital subtraction angiography is a time-consuming method that carries risks of thromboembolic and puncture-site complications. In comparison, computerized tomographic angiography (CTA) has several advantages, including low-contrast dose, low radiation exposure, short acquisition time, and low invasiveness. Moreover, CTA can be used to obtain parenchymal structural information that cannot be determined by catheter angiography. These advantages make CTA an attractive alternative to catheter angiography, and its diagnostic use has increased with improvements in multidetector computerized angiography (CT) techniques4,9,12).
However, clip artifacts limit the visualization of the vessels in the vicinity of the clip, particularly in patients in whom cobalt alloy clips have been used11-13,16). Several CT acquisition settings and modes have been proposed to reduce clip artifacts5,6,7,12). However, from a clinical perspective, switching to an artifact-reducing acquisition mode might not always be possible because aneurysmal clipping is frequently performed on an emergent basis.
In our daily clinical practice, we have observed that clip artifacts vary, even under the same imaging acquisition settings, according to clip orientation. These findings have been verified by van der Schaaf et al.12) and Pechlivanis et al.10) using CT scans in a phantom model. Those studies were performed in vitro using discrete numeric variables. To substantiate the effect of clip orientation and other factors on the degree of clip artifacts in vivo, we applied mathematical analysis using continuous numeric variables to retrospectively analyze the quantitative relationship between clip artifacts and related factors in real patients with cobalt alloy clips.
MATERIALS AND METHODS
Patients and image acquisition
Postoperative CT images of 60 patients who had undergone aneurysmal clipping surgery with a single straight cobalt alloy clip (Sugita Clip, Mizuho Ikakogyo Co., Tokyo, Japan) were retrospectively reviewed. The clipped aneurysms included 15 anterior cerebral artery aneurysms (anterior communicating artery, n=10; pericallosal artery, n=3; A2, n=1; and A1, n=1), 21 middle cerebral artery aneurysms (middle cerebral artery bifurcation, n=17; M1, n=2; and M2, n=2), 22 internal carotid artery aneurysms (posterior communicating artery, n=11; anterior choroidal artery, n=8; and internal carotid artery bifurcation, n=3), and 2 posterior circulation aneurysms (posterior cerebral artery, n=1; and basilar artery, n=1).
All patients underwent routine postoperative axial CT imaging. Of the 60 patients, 39 also underwent CTA by helical scan. All CT images were acquired using a 64-detector Lightspeed volume multidetector CT (GE Healthcare, Milwaukee, WI, USA). The CT image acquisition protocol was as follows : for axial scans (n=60), 120 kilovoltage peak (kVp), 200 mA, 5-mm section; for helical scans (n=39), 120 kVp, 300 mA, 0.625-mm section collimation, 0.96 pitch, and 0.4-second rotation speed.
Measurement and analysis of clip artifacts
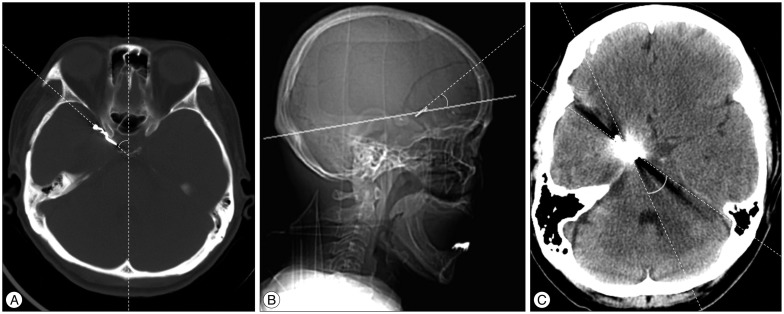
To determine the degree of clip artifacts, various factors were measured from the CT images. Independent variables for the degree of clip artifacts included the clip blade length and clip orientation. The clip blade length was determined as the total length of the clip minus the length of the clip spring portion. The clip orientation was determined as : 1) the lateral inclination of the clip blade to axial images (angle a), and 2) the gradient of the clip blade to the scan gantry angle on lateral scout images (angle b). The degree of lateral inclination of the clip blade to the CT axial scan (angle a) was measured as the angle between the clip blade and an imaginary midline from forehead to inion. Each angle was measured on the basis of minor and acute angles rather than major and obtuse angles from each fiducial line. Fig. 1 illustrates the detailed measurement methods, marking minor and acute angles in each image. The dependent variables were the maximal diameter (dmax) of white artifacts and the number and angle of visible streak artifacts on axial CT images, and the dmax of artifacts around the clip on three-dimensional (3-D) volume-rendered images in CTA. White artifacts were defined as white round artifacts around the clip in axial images. Streak artifacts were defined as black straight lines radiating from each side of the clip. The angle of visible streak artifacts on the axial CT images was the sum of each angle between the measured streak artifacts.
CTA images were reconstructed manually at the workstation from source images obtained from a helical scan. The amount of clip artifacts in 3-D volume-rendered images was measured as the dmax of clip artifacts in the vicinity of the clip in a 360В° rotational view. All measurements were made at the same window length/width/z-value setting (axial scan : 40/100/133.40%, volume- rendered scan : 127/255/96.06%). One author manually measured the artifacts and the other author performed the statistical analysis.
Initially, descriptive statistics were used to calculate the means and standard deviations of the clip blade length, angle degree to the CT scan according to clip orientation, and the dmax of each type of clip artifact. A correlation analysis using Pearson's correlation coefficients was performed between the independent variables and the degree of each type of artifact. Subsequently, all of the variables were assessed by univariate analysis with regression methods. For multiple linear regression analysis, backward-selection model buildup was used to determine which factor was more predictive of clip artifacts. A value of p<0.05 was considered significant for all analyses. Statistical analyses were performed with SPSS (SPSS Version 19.0 for Windows, SPSS Inc., Chicago, IL, USA).
RESULTS
The mean (Вұstandard deviation, range) of the clip blade length was 10.79 mm (Вұ2.41, 5-16). The means of angles a and b were 41.65В° (Вұ19.83, 0-90) and 19.75В° (Вұ21.62, 0-80), respectively. The average dmax value of the white artifacts was 13.2 mm (Вұ5.47, 1-29). The average angle and number of streak artifacts were 73.92В° (Вұ89.99, 5-360) and 3.83 (Вұ2.39, 2-12), respectively. The average dmax of the artifacts in 3-D volume-rendered images was 15.80 mm (Вұ13.14, 0-44).
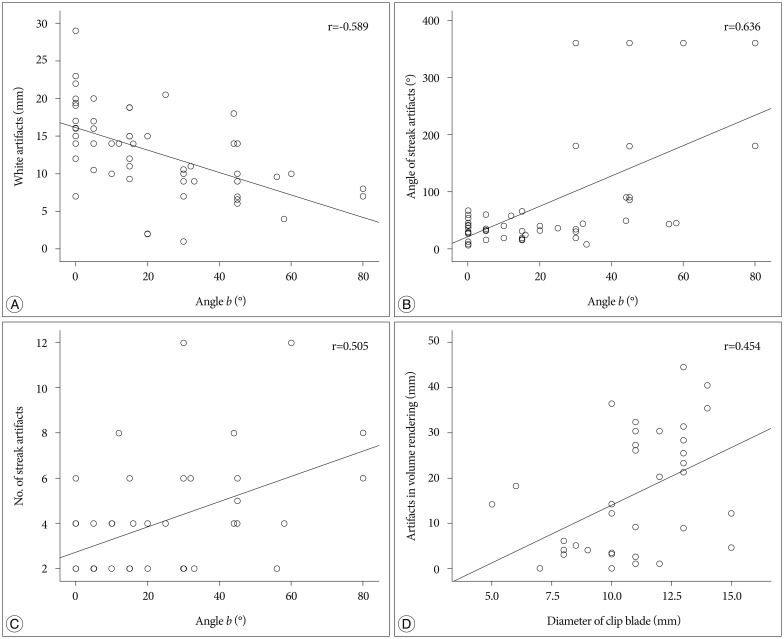
In correlation analysis, angle b was negatively correlated with the dmax of the white artifacts (r=-0.589, p<0.001) and positively correlated with the angle (r=0.636, p<0.001) and number of streak artifacts (r=0.505, p<0.001). The clip blade length was positively correlated with the diameter of clip artifacts in the 3-D volume-rendered images (r=0.454, p=0.004) (Fig. 2). Angle a had no statistically significant relationship with the clip artifacts (data not shown).
Linear regression analysis revealed that angle b was positively correlated to the dmax of the white artifacts (Гҹ=-0.108, p=0.005), the angle of the streak artifacts (Гҹ=2.745, p<0.001) and the number of streak artifacts (Гҹ=0.070, p<0.001). The clip blade length was linearly associated with the number of artifacts in the 3-D volume-rendered images (Гҹ=1.918, p=0.033) (Table 1). In the multiple linear regression analysis, both angle b and the clip blade length were positive predictors of the degree of each clip artifact in the axial scan (white artifacts, and angle and number of streak artifacts) and in the 3-D volume-rendered images, respectively (Table 2).
DISCUSSION
Since 1937 when Dandy2) first introduced the V-shaped silver clip, various materials have been used for intracranial aneurysmal clips. However, cranial metallic implants, particularly cobalt alloy clips, interfere with CT evaluation in the same anatomic location due to clip-induced artifacts. Since the introduction of titanium alloy clips, the occurrence of metallic artifacts adjacent to the clip has greatly decreased, resulting in widespread usage of titanium alloy clips. Although clips made from titanium alloy permit better visualization in the clip vicinity than those made from cobalt alloy3,11,12,14,16), the latter still play a large clinical role due to several advantages, including high tensile strength, high closing force, and extra-large and variously fenestrated clip profiles8). Therefore, we wanted to determine whether there were factors other than the clip property itself influencing the cobalt clip artifacts that could be easily managed.
Previous researchers have investigated various approaches for minimizing clip artifacts in post-aneurysmal clipping CT scans from patients. Some authors have proposed the use of ideal image acquisition parameters, such as pitch, kVp, reconstruction algorithm, and type or concentration of contrast material6,12,13). Others have suggested the use of ideal acquisition modes, including nonhelical6,7), gated multidetector CT5), and the orbital synchronized helical scan technique15). These previous studies have several limitations. For example, many were performed in phantom models6,7). The environment in the human brain after aneurysmal clipping is significantly different from the phantom environment due to the presence of bony structures, blood, brain, and soft tissues adjacent to the clip. Finally, the studies that have analyzed clip artifacts in patients had very small sample sizes1,5) or were not quantitative1,11,12,16). In 1999, Brown et al.1) first reported the effect of clip orientation on the number of clip artifacts. In their report on four patients, they proposed that lateral tilting of the head during CT acquisition could reduce the number of clip artifacts by projecting the aneurysm clip away from the remainder of the circle of Willis. In 2006, van der Schaaf et al.12) used a phantom model to evaluate different clip orientations and their effect on artifact volume, showing that positioning of the clip perpendicular to the scan plane led to significantly fewer artifacts. Those findings were quite in agreement with the findings of the present study, although the previous study dealt with the observation regarding clip orientation in a comparatively simpler fashion with selected clip-gantry angles of 0 degree, 45 degrees, and 90 degrees. To the best our knowledge, this study is the first to demonstrate a clear linear relationship between clip artifacts and the CT scan gantry angle in vivo. In addition to clip orientation, the authors attempted to use statistical analyses of clip blade length as a variable for clip artifacts based on the hypothesis that the amount of metallic component might influence the amount of clip artifacts. The study by van der Schaaf et al.12) dealt with the correlation between clip artifacts and kVp/pitch and proposed that 140 kVp and less than 0.6 pitch was an ideal setting for the reduction of metallic artifacts. Our study was conducted in a fixed setting of 120 kVp and 0.96 pitch, focusing on the clip orientation and clip property itself.
In summary, all clip artifacts that could be measured in a routine axial scan (white artifacts, and the angle and number of streak artifacts) were linearly correlated with the degree of angle b, whereas the artifacts in 3-D volume-rendered images were influenced by the clip blade length.
Of these factors, the scanning gantry angle is the only factor that can be modified during postoperative scanning. Indeed, the physician and technician could easily modulate this angle by altering the patient's head positioning (i.e., through head flexion or extension), or by altering the scan angle according to the CT lateral scout view in which the clip orientation is clearly visible. White artifacts interfere with the visualization of adjacent structures more than streak artifacts. The diameter of white artifacts in the CT scan could be reduced by changing the patient's head position or the gantry angle, with the clip blade being placed as perpendicularly as possible to the scan plane on the lateral scout view
This study has several limitations. Unfortunately, the correlation between the clip artifacts and clip orientation in the frontal scout view could not be analyzed because of the limitation of this retrospective analysis. Although the clip orientation on the lateral view is the most important contributing factor for the degree of clip artifacts in axial CT images, this is not the case with CTA reconstruction images. Three dimensional CTA might be associated with various technical factors, including patient motion and timing of contrast injection, thus it might be difficult to determine the mechanism underlying the amount of clip artifacts in these images. Compared with measuring artifacts in axial CT conducted under a constant two-dimensional field, measuring artifacts in CTA is more inconstant in 3-D space. Moreover, artifacts in 3-D CTA with a large dmax but small volume might be oversized in the measurements, because the artifacts are measured by diameter rather than volume. Because the use of a complex clip type, including a fenestrated or angled blade, might interfere with the results, we attempted to avoid this issue by including only cases with a straight clip blade. In spite of this effort, there is still a possibility that the clip spring portion might influence the pattern or amount of clip artifacts. Multiple clips or those with a complex shape preclude the clinical implication of artifact-reducing strategies based on clip orientation.
CONCLUSION
Clip artifacts generated by a cobalt alloy clip in a 64-channel CT scan may be influenced by the clip length and the angle between the clip and the scan plane. The number of white artifacts increased when the orientation of the angle between the clip blade and the scan plane was parallel. These findings suggest that clip artifacts after aneurysmal clipping could be minimized by simple maneuvers, such as minimal changes in the scan gantry angle on the lateral scout view if the clip blade is located parallel to the scan plane.