INTRODUCTION
Brain metastases (BMs) have been reported in up to 40% of patients with systemic cancer21), and the incidence of BMs is increasing due to the routine brain magnetic resonance imaging (MRI) screening and an improved outcome of systemic therapy against primary cancers. Management of BMs depends on their size, number, and location together with patient factors such as age, performance status, and primary disease status12).
Stereotactic radiosurgery (SRS), typically delivered in a single fraction, has been shown to be effective and safe in treating BMs and, is generally indicated for a single or oligometastases <3 cm in diameter. However, the toxicity of SRS given in a single fraction is considered to outweigh the benefits of local tumor control (LTC) for large BMs >3 cm and leads to increased risks of neurological morbidity from radiation necrosis (RN)3,1823). Although large lesions are often amenable to microsurgical resection, surgery is infeasible in cases of critical location and/or poor patient medical status.
Recently, the concept of fractionated stereotactic radiosurgery (FSRS) has emerged, and it is reportedly an effective and safe way to treat BMs, especially large lesions. Since June 2011, we adopted this approach in treating large BMs. Treatment outcomes were evaluated by the objective tumor response on MRI, patient survival and functional improvement, and radiation necrosis. Prognostic factors were also analyzed.
MATERIALS AND METHODS
Eligibility
This study was approved by the institutional review board of the Asan Medical Center. Between June 2011 and December 2013, a total of 37 patients with large BMs were enrolled according to the inclusion and exclusion criteria indicated below.
Inclusion criteria
1) Age of Ōēź18 years, with histologically proven solid cancer and fewer than 6 brain metastases, one of which is >3 cm in maximum diameter
2) Intact cognitive function; able to understand and sign a written informed consent
3) Life expectancy >3 months, as indicated by the medical oncologist
4) Karnofsky performance status (KPS) score Ōēź70, or 50-60 with focal neurological deficits
Exclusion criteria
1) Suffering from significant mass effect or raised intracranial pressure for which surgical decompression is indicated
2) Received any form of prior cranial irradiation
3) Received prior surgical resection of the targeted lesion
4) Primary hematologic malignancy, such as lymphoma or leukemia
5) Pregnant or breast-feeding patients
Demographic data
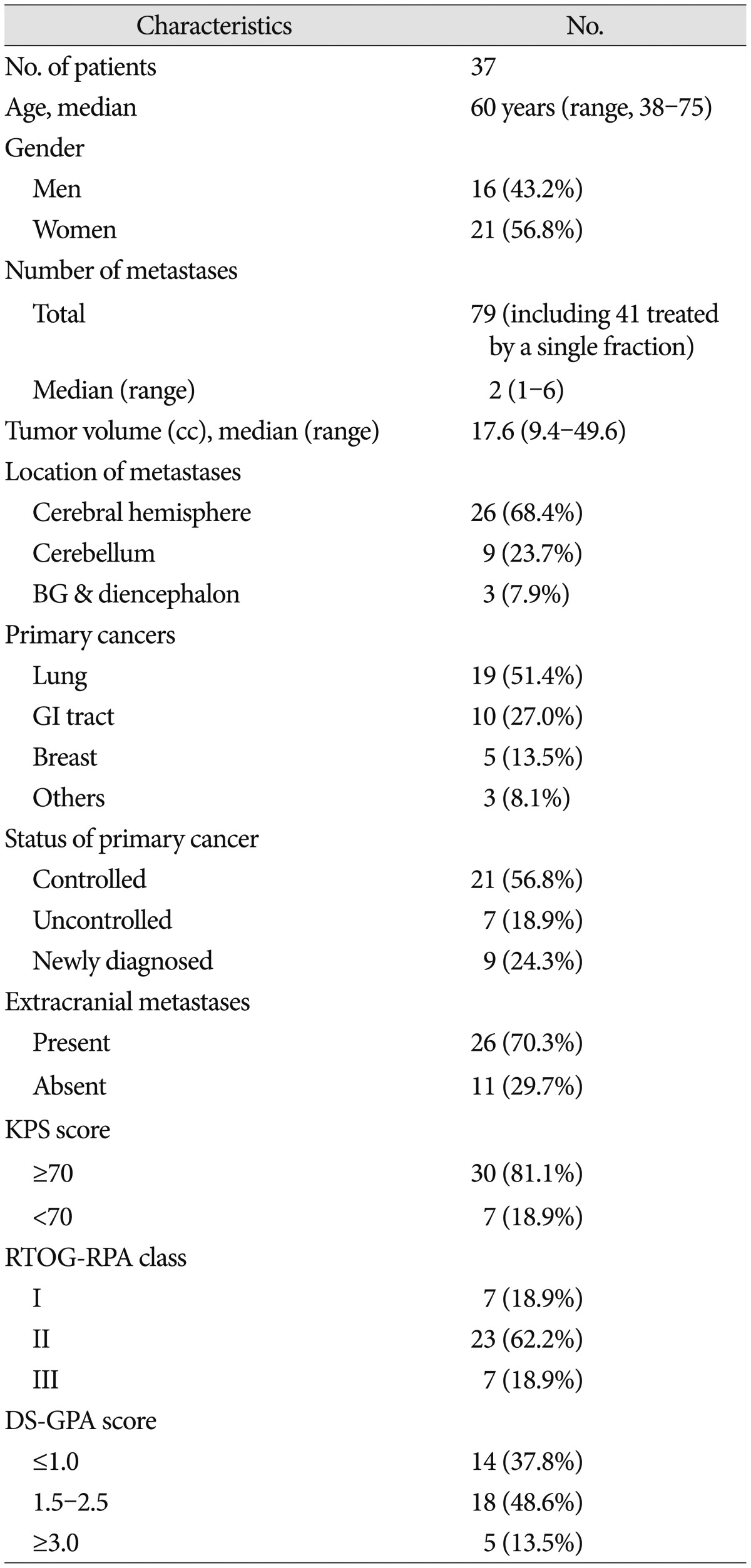
The baseline characteristics of the study patients are summarized in Table 1. Of the 37 patients included in the analyses, 16 were men (43.2%) and 21 were women. The median age was 60 years (range, 38-75 years). BMs originated from the lung (n=19, 51.4%), gastrointestinal tract (n=10, 27.0%), breast (n=5, 13.5%), and other tissues (n=3, 8.1%). At the time of FSRS, the primary cancer was under control in 21 patients (56.8%), and metastases to organs other than the brain were present in 26 patients (70.3%). The KPS score was Ōēź70 in 30 patients (81.1%), and focal neurologic deficits were present in 17 patients (45.9%). There were 7 patients (18.9%) of Radiation Therapy Oncology Group-recursive partitioning analysis (RTOG-RPA) class I, 23 (62.2%) of class II, and 7 (18.9%) of class III. The diagnosis-specific graded prognostic assessment (DS-GPA) score was Ōēż1 in 14 patients (37.8%), 1.5-2.5 in 18 patients (48.6%), and Ōēź3 in 5 patients (13.5%).
Tumor variables
Of 79 BMs in 37 patients, 38 lesions were >3 cm in diameter and were treated with FSRS. Lesions <3 cm were treated with single-fraction SRS and were not included in our analysis. The median tumor volume was 17.6 cc (range 9.4-49.7 cc). BMs were located in the cerebral hemisphere in 26 lesions (68.4%), the cerebellum in 9 lesions (23.7%), and the basal ganglia or the diencephalon in 3 lesions (7.9%) (Table 1).
Fractionated stereotactic radiosurgery
All patients were treated using the Cyberknife radiosurgery system (Accuray Inc., Sunnyvale, CA, USA). Patients were immobilized using a thermoplastic mash mask. Treatment planning CT images were acquired with a 1.25 mm slice thickness. MR images including axial/sagittal/coronal T2-weighted sequences (2 mm slices) and 3D-T1-weighted gadolinium enhanced sequences (2 mm slices) were also obtained. The MRIs were registered and manually fused with the planning CT images in the Accuray MultiPlan treatment-planning system (version 4.5) to facilitate the delineation of the gross tumor volume (GTV; equal to the planning target volume) and the critical organ structures including the brainstem, the eyes, and the optic apparatus. Additional hollow structures (shells) 3 mm and 30 mm away from the GTV were generated to optimize the conformity and dose compactness. A sequential optimization method was used along with the dose objectives to optimize minimum GTV dose and coverage. A ray-tracing algorithm was used for dose calculation. The prescription isodose percentage was applied to approximately 80% of the maximum dose with a conformity index (CI, defined as the prescribed isodose volume divided by the volume of tumor encompassed by the prescription isodose volume) <1.2 and GTV coverage >99%. The median prescription dose was 35 Gy (range, 30-41 Gy). Doses were administered in 3 to 5 daily fractions depending on the size of lesions; lesions <3.5 cm were treated in 3 fractions and lesions Ōēź3.5 cm in 5 fractions.
Follow-up, outcome measures, and statistics
Follow-up clinical examination and MRI were performed at 3-month intervals after treatment.
Tumor size was defined as the largest cross-sectional area at follow-up MRI. Each lesion was measured to evaluate local tumor response and graded using the MacDonald criteria29). Complete response was indicated by a complete disappearance of all enhancing lesions on MRI, no corticosteroid use, and clinical stability or improvement. Partial response was indicated by >50% decrease from the baseline in perpendicular diameter product sums of all measurable enhancing lesions on MRI, elimination or reduction in corticosteroid dose, and clinical stability or improvement. Progressive disease was indicated by >25% increase in perpendicular diameter product sums of enhancing lesions on MRI, appearance of a new lesion, or clinical deterioration. Patients were considered to have stable disease if they did not meet the qualifications for complete response, partial response, or progression. LTC was defined as complete response, partial response, or stable disease. Local failure was defined as radiographic progression at the treatment site. Distant failure was defined by the development of new BMs outside the treatment site.
RN was assessed objectively using MRI or confirmed pathologically after surgical resection. The following criteria were considered for RN : 1) increased T1 contrast enhancement located in the irradiated area with central hypointensity and increased peripheral edema, 2) substantial regression or stability (for at least 3 months) of enhancing areas on serial follow-up MRIs without additional treatment, or 3) absence of perfusion within the contrast-enhancing lesion on dynamic susceptibility contrast perfusion MRI19). All radiation toxicities were graded using National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE Version 4.0).
LTC, overall survival (OS), progression-free survival (PFS), and RN were estimated using the Kaplan-Meier method calculated from the treatment start date to the date of events or the last follow-up. Factors possibly affecting the outcome were tested using the log-rank test for univariate analysis and the Cox proportional hazards models with variable selection, which included age (Ōēź65 years vs. <65 years), gender, primary cancer type, tumor location, tumor volume (<22 cc vs. Ōēź22 cc), single vs. multiple BMs, status of primary cancer, presence of extracranial metastases, pretreatment KPS score (Ōēź70 vs. <70), ROTG-RPA class, DS-GPA score, and prescription dose. All statistical tests were conducted using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at p<0.05.
RESULTS
Objective tumor response and local tumor control
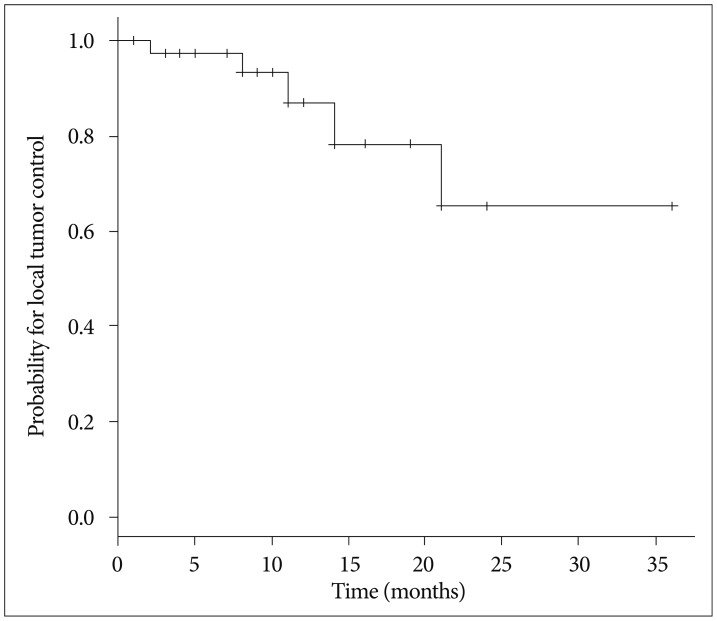
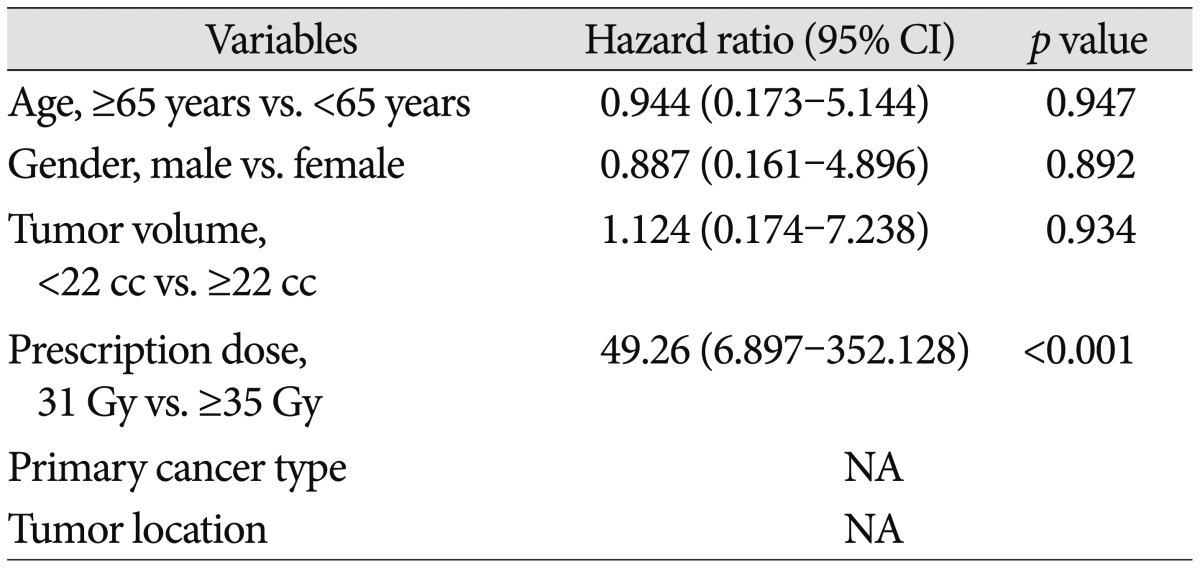
The maximum tumor response was evaluated for 36 lesions after exclusion of two lesions for which no follow-up images were available. The rates of complete response, partial response, stable disease, and progressive disease were 11.1%, 44.4%, 30.6%, and 13.9%, respectively. With a median follow-up of 10 months (range, 1-37 months), the crude LTC rate was 86.8% and the estimated LTC rates at 12 and 24 months were 87.0% and 65.2%, respectively (Fig. 1). Prescription dose was the only factor affecting the LTC on univariate and multivariate analysis. Both of the lesions treated with a prescription dose of 31 Gy developed local failure, whereas only 3 of 36 lesions with a prescription dose of Ōēź35 Gy developed local failure (hazard ratio, 49.26; 95% confidence interval, 6.897-352.128; p<0.001) (Table 2).
Survival
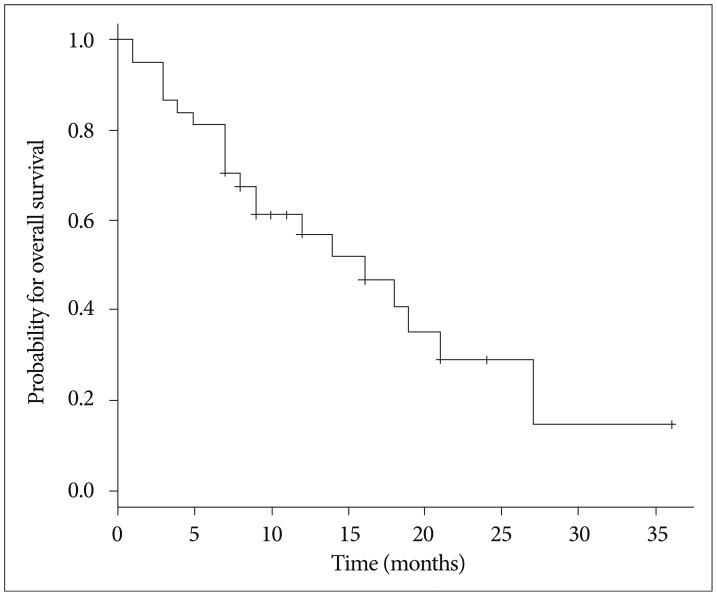
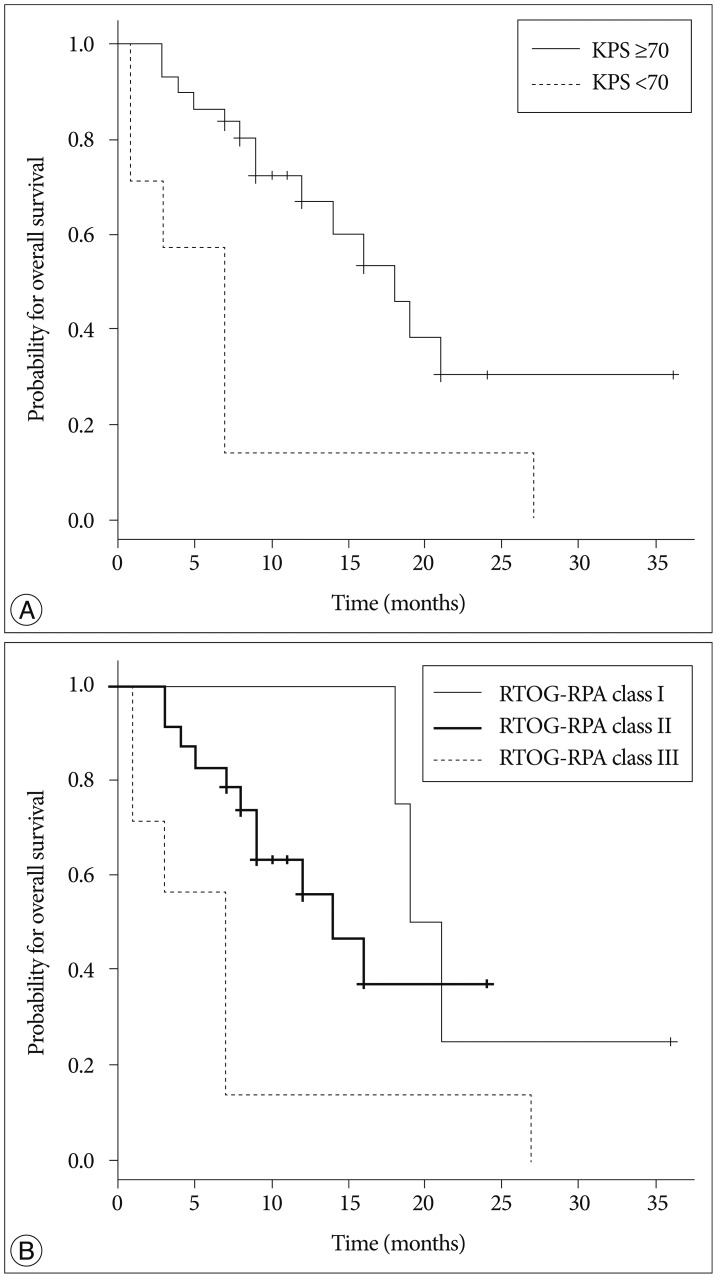
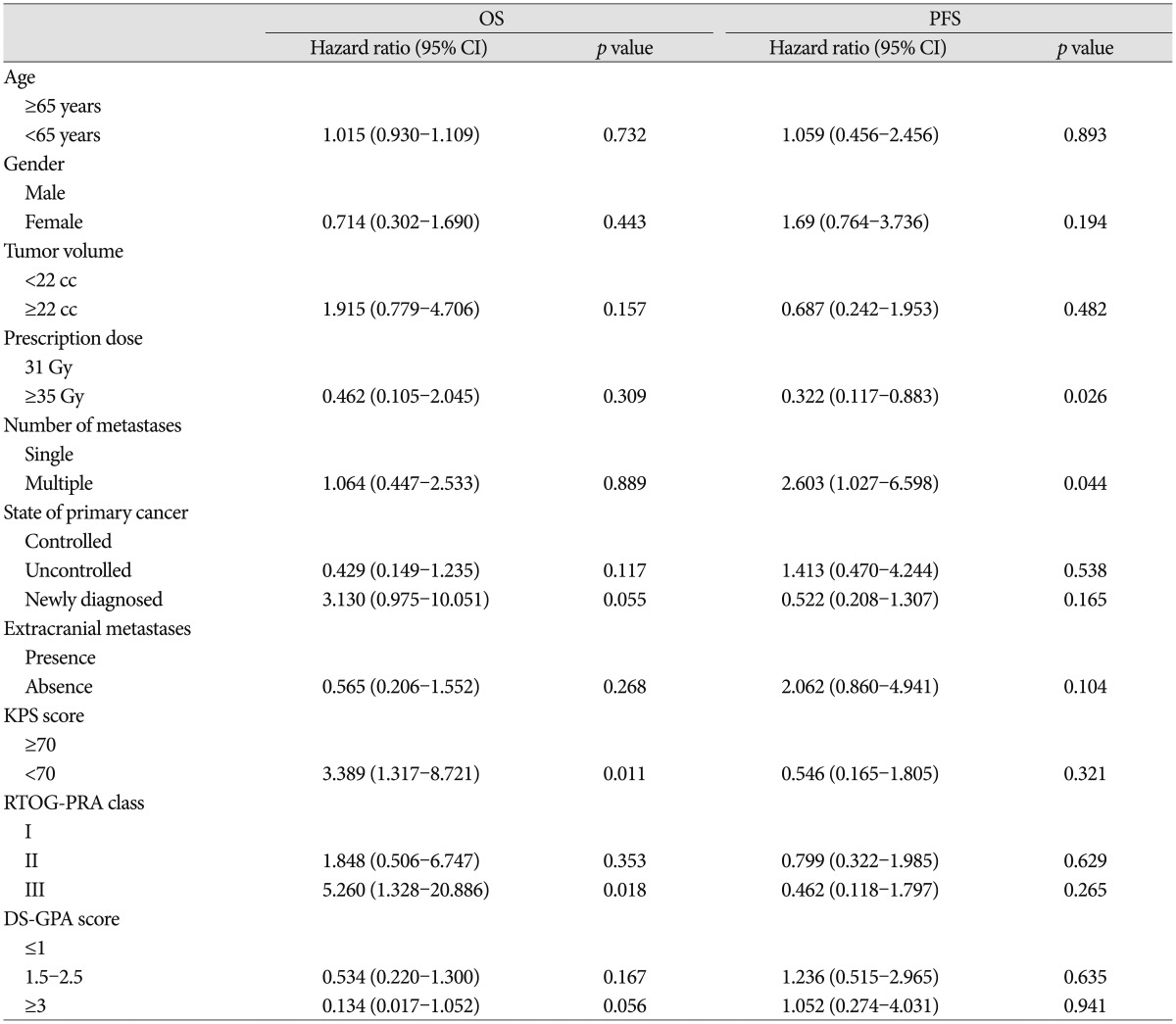
The Kaplan-Meier curve for OS is shown in Fig. 2. The median OS was 16 months, and the estimated OS rates at 6, 12 and 18 months were 81.1%, 56.8%, and 40.7%, respectively. Of 21 patients who died, 10 (47.6%) died from the progression of extracranial disease, 6 (28.6%) from brain failure, and 5 (23.8%) from unknown causes. On univariate analysis, KPS score <70 (hazard ratio, 3.389; 95% confidence interval, 1.317-8.721; p=0.011) and RTOG-RPA class III (hazard ratio, 5.26; 95% confidence interval, 1.328-20.886; p=0.018) indicated poor patient survival (Table 3, Fig. 3), although only RTOG-RPA class remained significant on multivariate analysis.
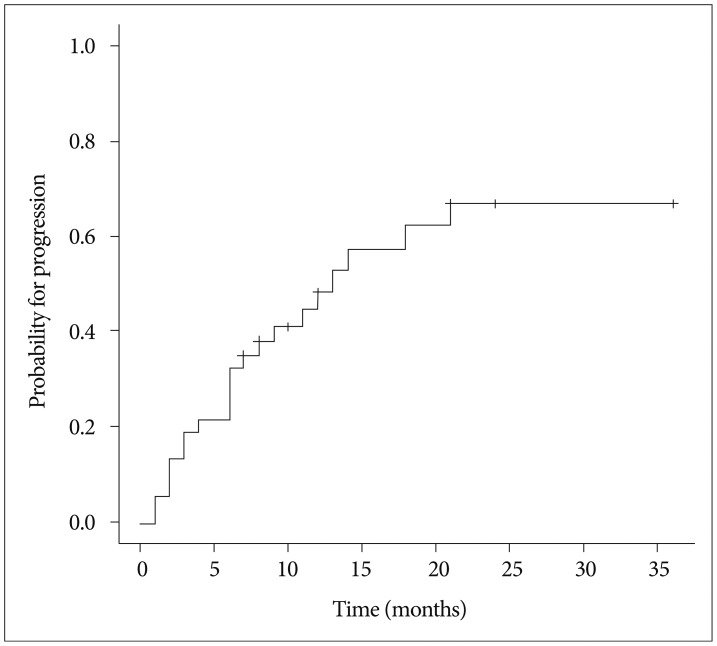
Twenty-one patients (56.8%) showed progression including distant failure in 20 patients, local failure in 5 patients, and both distant and local failure in 4 patients. The median PFS was 11 months and the estimated PFS rates at 6, 12, and 18 months were 65.5%, 44.9%, and 25.7%, respectively. The cumulative incidence function (CIF) for progression is shown in Fig. 4. Multiple BMs were associated with poor PFS (hazard ratio, 2.603; 95% confidence interval, 1.027-6.598; p=0.044) (Table 3), as 14 of 19 patients (73.7%) with multiple BMs developed progression vs. 7 of 18 (38.8%) with a single BM.
Neurological and functional outcomes
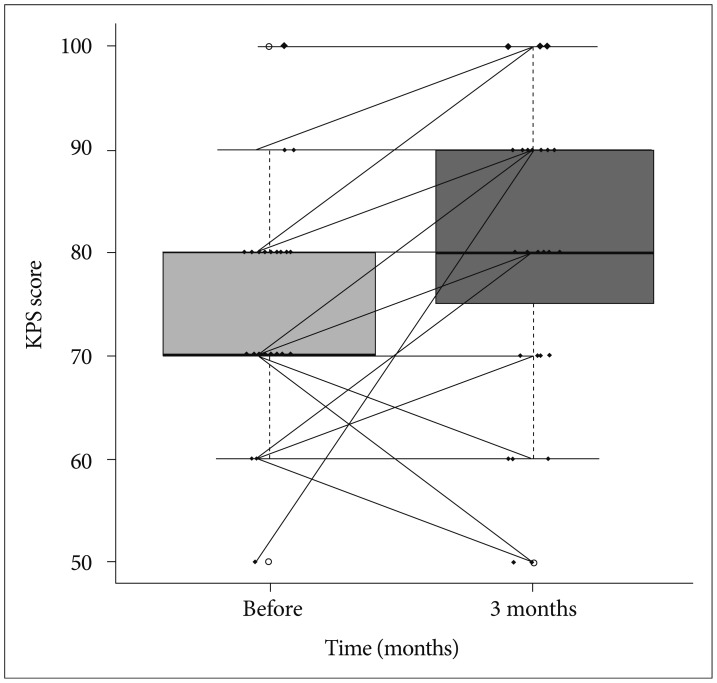
Preoperative focal neurologic deficits such as motor weakness and cerebellar dysfunction, improved in 12 of 17 patients (70.6%) 3 months after treatment. The KPS score improved in 20 of 35 patients (57.1%), with a mean preoperative KPS score of 74 (median, 70; range, 50-100) vs. a mean KPS score of 80.6 (median, 80; range, 50-100) 3 months after treatment (p=0.001) (Fig. 5).
Radiation necrosis
RN occurred in 6 of 38 lesions (15.8%). CIF for RN is shown in Fig. 6. The median time to RN was 10.5 months (range, 6-18 months). Five patients with RN of toxicity grade 2 were controlled with corticosteroid medication and 1 patient with toxicity grade 3 was salvaged by surgery. No factors were identified that affected the occurrence of RN.
DISCUSSION
Although SRS typically delivered in a single fraction has been proven to be effective and safe in treating BMs, it is not feasible for large lesions, especially those >3.0 cm, due to increased toxicity and local treatment failure3,1823,24). Microsurgical resection is usually indicated for large BMs, immediately decompressing the mass effect and alleviating neurological symptoms. However, not all patients with large BMs are eligible for surgery when considering surgical accessibility, the number of lesions, and patient medical status17,33). Moreover, systemic therapy against primary cancers should be withheld during perioperative periods, which can be further confounded by surgical morbidity in certain cases. Alternatively, whole-brain radiotherapy (WBRT) remains palliative in nature and may influence cognitive function. Currently, the first-line treatment for large BMs has not been established and is usually determined by considering various factors, including tumor volume, number, location, and overall condition of patient12).
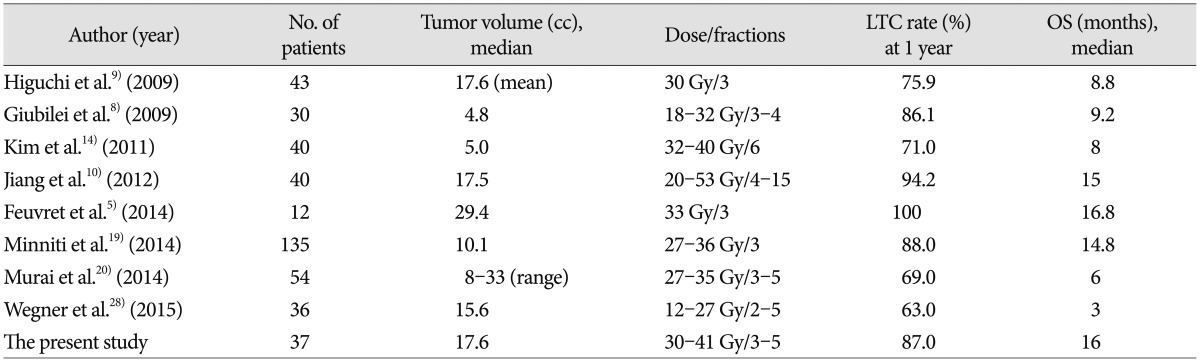
Theoretically, fractionated administration of radiation dose potentially minimizes toxicity to late-responding healthy tissues, with a low ╬▒/╬▓ ratio compared to a single acute dose of radiation for a given level of tumor damage, according to the linear quadratic model of cellular survival8,26). In addition, reoxygenation and redistribution of the cell cycle between dose fractions renders hypoxic tumor cells, which are abundant in large BMs compared to small tumors, more radiosensitive6,1422,25). As expected, recently published studies on FSRS for large BMs have demonstrated high LTC rates, ranging from 63-100%, at 1 year follow-up, with acceptable risks of toxicity1,410,1415,31) (Table 4). Consistent with these results, our present LTC rates were 87.0% and 65.2% at 1- and 2-years follow-up, respectively, and the median OS was 16 months, which also compares well with the outcomes of single-fraction SRS for small BMs2,1113,16). Furthermore, patient performance status and neurological function improved significantly, presumably benefitting the quality of life in these cases.
The optimal dose fractionation protocol for FSRS in BMs has not yet been established. In a recent systematic review on stereotactic radiotherapy dose and LTC probability, Wiggenraad et al.30) reported that a biological effective dose, using an ╬▒/╬▓ ratio of 12 (BED12), of at least 40 Gy, which correspond to a single fraction dose of 20 Gy, was associated with a 1-year LTC rate of 70% or more. The high LTC rate at 1-year follow-up in our present study appears to accord with this observation. Lower LTC rates have been also associated with large BMs27,32). Vogelbaum et al.27) reported a 1-year LTC rate of 45% for lesions of 3.1-4.0 cm in diameter vs. 85% for lesions Ōēż2.0 cm with a prescription dose of 15 Gy. In our present analyses, which included only large BMs, the overall LTC rates observed were comparable to historic single fraction SRS for small BMs.
The LTC rates of even larger lesions in our current series (Ōēź3.5 cm) treated with more fractions were not inferior to those of lesions <3.5 cm, indicating a promising role of FSRS in treating large BMs. Recently, Murai et al.20) reported that dose fractionation of 27-30 Gy in 3 fractions and 31-35 Gy in 5 fractions on consecutive days was tolerable and effective in treating large BMs. Further studies are needed to determine the optimal dose fractionation protocol, especially in relation to tumor size.
RN has been reported at a rate of 2-15% after FSRS1,410,1415,31). In our current study, RN occurred in 6 out of the 38 lesions we examined (15.8%), which falls at the upper margin of this range. This can be explained in part by a slightly higher prescription dose employed for our present cases and lack of uniform criteria for RN in different studies. Meanwhile, most of our patients with RN were controlled with corticosteroid medication, except for one instance salvaged by surgery. As the incidence of brain necrosis after SRS increases with the size of the target volume, the volume of normal brain receiving a certain threshold dose has been implicated in the development of RN3,1819,23), with smaller volumes having a lower risk of RN.
In line with previous studies, our multivariate analysis showed that good patient performance (KPS score Ōēź70) and lower RTOG-RPA class significantly predicted a better survival outcome. Gaspar et al.7) reported that RTOG-RPA class I cases had the best survival outcomes (median 7.1 months), whereas those of ROTG-RPA class III had the poorest survival results (median 2.3 months). Kim et al.14) reported that good KPS (Ōēź70), controlled primary cancer, no extracranial metastases, lower RTOG-RPA class, higher DS-GPA score, single brain metastasis, and absence of previous WBRT were significant predictors of longer survival, Of these variables, only the number of extracranial metastatic organs was found to be a only significant predictor in our multivariate analysis. Minniti et al.19) reported previously that stable extracranial disease and a good KPS (>70) were associated with the most significant survival benefit.
FSRS is now emerging, yet controversial and not a current standard of practice in treating large BMs. This study presents additional clinical data that support the application of this approach as valid modality in terms of efficacy and safety.