INTRODUCTION
Postmenopausal osteoporosis is a disease characterized by low bone mass and depleted bony microarchitecture because of increasing bone turnover induced by estrogen deficiency [15,33]. Implant insertion is very important in the surgical treatment of bone fracture for patients with osteoporosis. The reduction in bone mass lessens the capacity of bone to support an orthopedic implant [6,15]. Consequences can include screw loosening or pull out, and delayed deformity of adjacent structures.
MATERIALS AND METHODS
Animals
This study was approved by the Institutional Animal Care and Use Committee of Asan Institute for Life Sciences, Seoul, Republic of Korea. Twenty-four female Wistar rats (250-300 g, 12 weeks of age) were divided into four groups : sham (control, sham-operated) group, ovariectomy (OVX)-induced osteoporosis group, OVX and biodegradable screw (OVX with screw) group, and OVX and BMP-2 containing biodegradable screw (OVX with screw BMP) group.
Ovariectomy
Rats were anesthetized with 5% isoflurane. Each received a 4 cm bilateral dorsal skin incision. Dissection was done to the retroperitoneal space to reveal the ovary surrounded by a whitish fat tissue. After ligation of the blood vessels, the connection between the fallopian tube and the uterine horn was severed. Each rat received an intra-muscular injection of antibiotic (cefazole 10 mg/kg, ketoprofen 5 mg/kg) daily for 3 days postoperatively. Body weight was measured once each 2 week for 16 weeks. Body weight was measured once per week for 16 weeks during the experimental period to ensure that animal models remain stable.
Screw modification
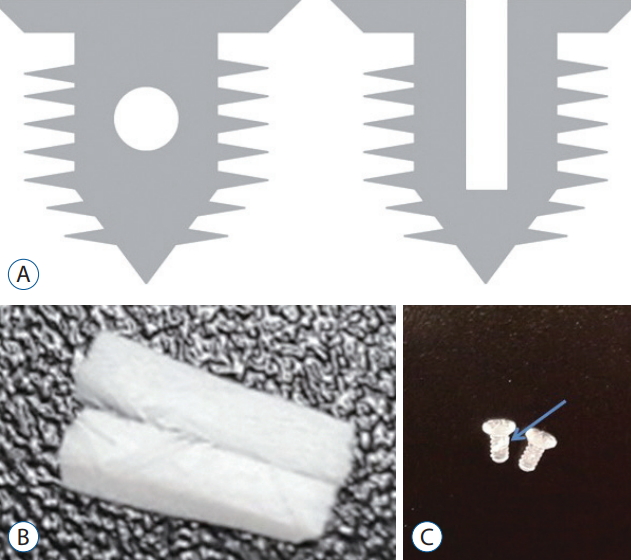
The Inion CPSŌōć L-lactide biodegradable screws (Inion, Tampere, Finland) were 2 mm in outer diameter and 5 mm in length. Two 0.5 mm sized perpendicularly crossed holes were made (Fig. 1A). An absorbable collagen sponge (CollatapeŌōć; Zimmer Dental, Carlsbad, CA, USA) was used as a carrier for retention and delivery of recombinant human BMP-2 (rhBMP-2; Sigma-Aldrich, St. Louis, MO, USA) at the implantation site (Fig. 1B and C) A piece of CollatapeŌōć (1├Ś5 mm) was inserted into the hole. Sterile water solution alone or containing 0.5 mg BMP-2 was applied to a collagen sponge, resulting in a final implant BMP-2 concentration of 4 ug/mL of BMP-2.
Implantation
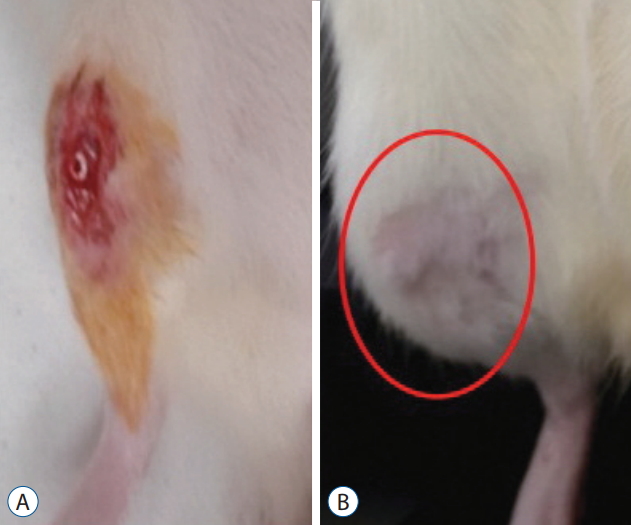
Implantation in the ovariectomized rats was delayed by 4 weeks following the procedure to allow osteoporotic changes to occur. On the first day of week 5, each rate received a 5-6 mm longitudinal skin incision along the tibia. After soft tissue dissection, a hole was drilled using a 1.4-mm electronic drill 5 mm distal from the proximal tibial growth plate. A screw was inserted in the hole (Fig. 2A). The soft tissue was sutured and each rat received an intra-muscular injection of aforementioned antibiotic for the next 3 days.
Micro-computed tomography (micro-CT) evaluation
Sixteen weeks after OVX, tibiae were extracted and surface soft tissues were removed prior to structural and functional measurements. The samples were scanned by high-resolution micro-CT using a Skyscan 1176 micro-CT apparatus (Skyscan NV, Kontich, Belgium). The volume of interest (VOI) was defined distal from the growth plate and extending towards the diaphysis for 7.1 mm at a distance of 1.0 mm (340 slices). In each transverse slice of the VOI, the region of interest was defined as the entire trabeculae around the implants including the near implant area. The acquisition settings were as follows : X-ray source voltage 49 kV and current 200 ╬╝A. A 0.5 mm-thick aluminum filter was used to reduce bean hardening artifacts. The pixel size was 8.7 mm in a 4000├Ś2096 charge-coupled device (CCD) detector array. The exposure time was 670 ms using a stepwise and rotation of 0.4┬░ with complete rotation achieved. Image reconstruction and analysis were performed using Skyscan software. The parameters evaluated included trabecular bone volume (BV/TV; %), trabecular number (Tb.N;/mm), trabecular separation (Tb.Sp; mm), trabecular thickness (Tb.Th; mm) and bone mineral density (BMD; g/cm2).
Hematoxylin and Eosin (H&E) staining
After decalcification, the tibia samples were fixed in paraffin and cut longitudinally at a thickness of 3 ╬╝m using a model RM2255 microtome (Leica Microsystems, Wetzlar, Germany). Each section was mounted on a slide and put in a 55oC. The sections were de-paraffinized in three 5-minute changes of xylene and dehydrated in three 5-minute changes in sequentially increasing alcohol solutions (70%, 80%, 90%, and 100%). The slides were rinsed in flowing distilled water for 1 minute and immersed in Harris Hematoxylin-I (YD-Diagnostics.com, Yongin, Korea) for 5 minutes, followed by a 1-minute wash in flowing tap water. The sections were then dehydrated from 70% to 100% ethanol and stained with Eosin Y (Sigma-Aldrich) for 30 seconds. Residual stain was washed off in a flow of distilled water. Each section was mounted (Shandon Synthetic Mountant; Thermo Fisher Scientific, Waltham, MA, USA).
MassonŌĆÖs trichrome staining
After staining of nuclei using an iron-hematoxylin kit (VWR International GmbH, Lerzenstrasse, Switzerland), samples were stained for 15 minutes using azophloxin. Samples were washed using 1% acetic acid, placed it in acid Orange G (Sigma, St. Louis, MO, USA) solution until collagen decolorixed and rinse with 1% acetic acid repeatedly for 30 seconds each time. Samples were stained with Light Green (Sigma) for 5 minutes and rinsed in 1% acetic acid repeatedly for 5 minutes.
Statistical analyses
Data were represented as means┬▒standard deviations. According to the result of normality test, two-way repeated measures analysis of variance was applied to compare the change of body weight per group. Post hoc comparison was conducted at each time point which showed statisticially significant difference with studentŌĆÖs t-test and BonferroniŌĆÖs correction. Comparing micro-CT measurements among groups, Kruskal-Wallis test was performed and post hoc comparison was done at each value with Mann-Whitney U test and BonferroniŌĆÖs correction. A two-tailed p<0.05 was considered as statistically significant. All statistical analyses were performed using R (version 3.3.2; The R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
All animals tolerated the procedure well and rats could walk on all four legs immediately postoperatively. Most of the rats in the OVX with screw BMP group experienced mild swelling at implantation sited for 3 to 7 days after implantation. There were no cases of infection or wound dehiscence, and no complications related to screw implantation during the experimental period (Fig. 2B). No animals died or had to be euthanized.
In vitro observations
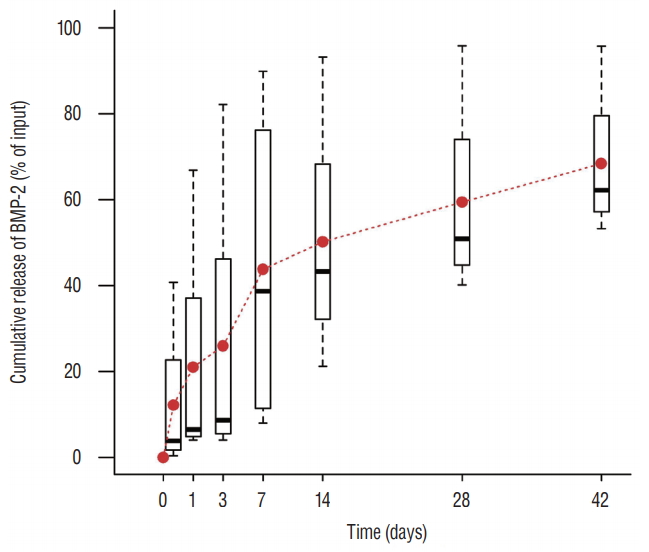
An initial burst (about 50%) in BMP-2 release occurred within the first 7 hours after contact with phosphate-buffered saline, followed by a steady release of 0.1 to 0.4% per day thereafter (Fig. 3).
Body weight
There was no significant difference in the body weight between the four groups at baseline. Body weight in the rats that underwent ovariectomy (OVX, OVX with screw, and OVX with screw BMP group) were higher than the control group. Total body weight differed significantly between the control and the other groups (p<0.05) (Fig. 4).
Micro-CT
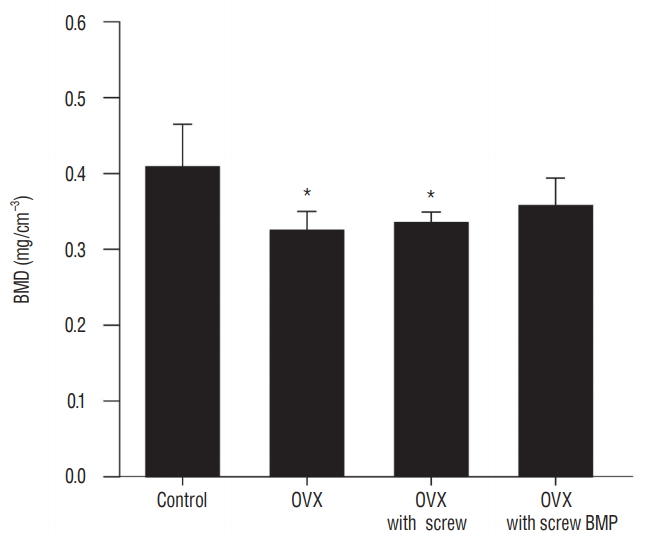
Representative micro-CT images shown in Fig. 5 illustrate the osteoporotic changes of bone in OVX, OVX with screw, and OVX with screw BMP groups after ovariectomy. New trabecular formation near the site of screw insertion was evident only in the OVX with screw BMP group (Fig. 5). BMD (Fig. 6) and BV/TV (Fig. 7A) of the control group were highest of all four groups, with a significant difference between the control and OVX and OVX with screw groups (p<0.05), No significant difference was evident between the control and OVX with screw BMP group (p>0.05). Tb.N displayed the same trend (Fig. 7B). However, there was a significant difference between the control group and the other groups (p<0.05). Tb.Sp of the control group was lowest among all the groups (Fig. 7D). There was a significant difference between the control and OVX and OVX with screw groups (p<0.05), but there was no statistically significant difference between the control and OVX with screw BMP groups (p>0.05). A significant difference was also apparent in the OVX and OVX with screw BMP groups (p<0.05) (Fig. 7).
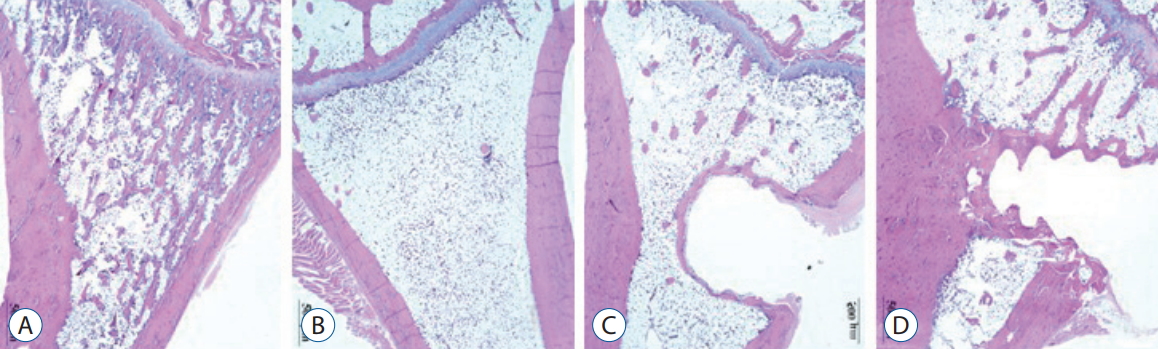
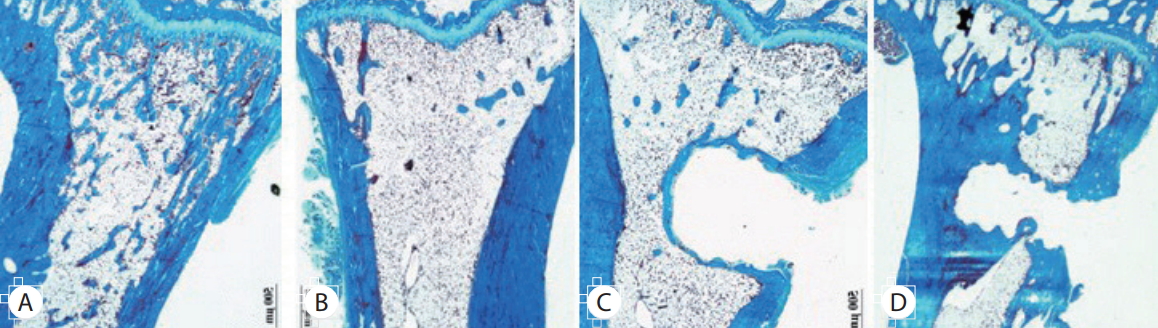
Histology
Over the 16 weeks after ovariectomy, histologic findings of H&E and MassonŌĆÖs trichrome staining revealed no inflammation or negative host response in any sample. There was less granulation tissue and more organized bone formation (Figs. 8 and 9). Histology of tibia revealed decreasing bony trabeculae and increased proportion of adipose tissue in the bone marrow in the OVX, OVX with screw and OVX with screw BMP groups compared with the control group (Figs. 8 and 9). The OVX with screw BMP group showed better findings than the OVX and OVX with screw groups, although not to the level of the control group. Thicker trabecular bone was observed in the bone lamellae of the direct contact area with the screw in the OVX with screw BMP group better than the OVX with screw group. In comparison with the OVX with screw group, mineralized collagen around the screw contact area appeared greatest and most organized in the OVX with screw BMP group (Fig. 9).
DISCUSSION
Orthopedic implant insertion is an accepted treatment of skeletal disease [1,16]. Various systemic conditions including postmenopausal osteoporosis affect host bone structure and can diminish the long-term success of implants [9,16,18,19]. The increased bone turnover that occurs with estrogen deficiency causes postmenopausal osteoporosis, which is low bone mass and worsening of bone microarchitecture [15,33]. This can decrease in support of an orthopedic implant [6,15]. Without appropriate treatment for osteoporosis, orthopedic implant fixation can be delayed and the procedure can ultimately fail [15,17,30]. Bone grafting is a typical conventional procedure to enhance the osteointegration between host bone and orthopedic implant. Complications include infection, donor-site morbidity and prolonged rehabilitation [2,12].
BMP first identified by Urist [27] as a signal transduction material belonging to transforming growth factor-beta is capable of osteoinduction-inducing osteogenesis from mesodermal cells [2,32]. BMP-2 helps promote cell growth and differentiation [2,14,31], and acts directly on the induction and differentiation of osteoblasts, which participate in fracture healing and the regeneration of damaged bone tissue [2,14]. The advent of rhBMP manufacture has allowed the mass production of BMP. The safety and excellence of rhBMP-2 has been demonstrated [14,32]. However, problems associated with BMP that remain include immune response, high cost, stimulation of unwanted ectopic bone formation and tumor formation [4,14]. Furthermore, BMP is typically supplied as a liquid, which complicated its use during surgery. It is difficult to induce ideal bone formation because BMP diffuses and is absorbed at a very high rate at the injection site [14,29]. Establishing a suitable scaffold system to deliver the appropriate dose of BMP is an important clinical goal.
The ideal delivery system of BMP in the orthopedic implant provides sufficient space for bone growth, mechanical strength as a structural support, excellent biocompatibility, allows the constant release of an appropriate quantity of the material [14], maximizes bone formation, has a porous structure that induces cell attachment and cell infiltration [28] and is safely degraded and reabsorbed [10,13,14,29]. A suitable biocompatible system for the delivery of BMP to maximize bone regeneration remains a challenge [28]. In previous study described the use of a collagen sponge to release rhBMP-2 as a means of rapidly inducing osteogenesis by osteoprogenitor cells [3,8]. Because of this fast release, rhBMP rapidly diffuses to the fracture site before reaching a critical density for the new infiltration of cells [8]. Another study reported that prior to new bone formation in the metaphyseal defects, fast release of rhBMP produces osteoclast-mediated resorption [3,8,26]. While the limitations of the collagen sponge have been well documented, there is a lack of evidence demonstrating superior release kinetics of other delivery systems. Hence, we chose the collagen sponge as the delivery system in this study. Collatape can absorb BMP quickly, has excellent biocompatibility and a rapid biodegradable rate. However, Collatape lacks sufficient mechanical strength and early bone resorption of BMP can occur; both can induce bone weakness [28]. We used a modified biodegradable screw as the structural support. The modified screw that featured a central canal that housed the BMP-2 soaked collatape proved to be a good system for the delivery of BMP for the induction of osteogenesis. Therefore, micro-CT scans revealed trabecular formation near the screw insertion site only in the OVX with screw BMP group (Fig. 5). Measurements of BMD and BV/TV indicated the efficacy of the screw system.
The dose of BMP used in bone healing treatment is a crucial safety concern. The dose must be high enough to control the biological regulation of osteoblastic and osteoclastic factors [22,28] and involves an amount of progenitor cells that is sufficient to form new bone [23,28]. However, very high BMP dose leads to excessive edema and inflammation, as well as formation of cystic change of the bone, or ectopic bone formation [15,20,24]. The appropriate dose of BMP remains contentious, with different effective concentrations claimed based on different animal models and study environments [15]. A bone defect rat model reported that the minimum amount to achieve femoral defect filling using a non-glycosylated BMP-2 with a fibrin matrix was 5 ╬╝g/mL [21,28]. Another study reported doses less than 5 ╬╝g of non-glycosylated BMP-2 was not sufficient to achieve vertical bone regeneration using a collagen/hydroxyapartite/synthetic polyethylene glycol-hydrogel scaffold/titanium implant combination in a rat mandible model [28]. It should be noted that the 5 ╬╝g dose was the lowest and most effective dose in the latter study. Another study of rat calvarial defect model reported that 5 ╬╝g of BMP was too low, although more than 90% of rat calvarial defects were regenerated during 12 weeks, the new bone was only 65% of the density of the native bone under this density of BMP [5,28]. In the present study, the model was not bone defect model. We used 4 ╬╝g/mL, which is relatively lower dose to the lower limit of the osteogenic threshold. In this study, there was thicker trabecular bone was observed in the bone lamellae of direct contact area with the screw in the OVX with screw BMP group better than OVX with screw group, although not to the level of the control group. In comparison with the OVX with screw group, mineralized collagen around the contact area of the screw appears greatest and most organized in the OVX with screw BMP group (Fig. 9). Furthermore, because of the safety concern, a low dose of BMP is better, in terms of minimizing complications like severe swelling and osteoclastic bone changes.
In this study, most of the rats of the OVX with screw BMP group exhibited mild swelling for 3 to 7 days after implantation. However, none had issues of infection or wound dehiscence, and there were no complications concerned with implantation of the screws in experimental period (Fig. 2). Histologic findings of H&E and MassonŌĆÖs trichrome staining showed no inflammation or negative host response in any sample. There was also less granulation tissue and more organized bone formation (Figs. 8 and 9).