INTRODUCTION
Petrous apex meningiomas have puzzled neurosurgeons for decades due to their deep location and surrounding structures, namely carotid canal, Dorello canal, internal acoustic canal, subarcuate canal, and MeckelвҖҷs cave [1]. Permanent neural morbidity was reported up to 39.9% after resection of these rare tumors [4]. In recent years, extensive surgical approach was introduced to this area, such as transpetrosal, transcochlear, translabyrinthine, and suboccipital retrosigmoid approach [12,15,18,19]. Among these surgical approaches mentioned above, the suboccipital retrosigmoid approach is popular and offer a wide range to achieve total removal. However, due to operation space is as narrow as 3 mm and operation distance is as deep as 10 cm, the suboccipital retrosigmoid approach isnвҖҷt suitable to remove meningioma hidden before brainstem.
Transpetrosectomy approach which gave neurosurgeons a more anterior view compared to the the suboccipital retrosigmoid approaches and enabled neurosurgeons to operate before cranial nerves VII-XII rather than behind, was first described by Bochenek and Kukwa [2] in 1975. In 1991, Kawase et al. [9] modified this approach to operate on petroclival meningiomas by extradural drilling of the Kawase triangle. However, Xiao et al. [24] proposed that this extradural approach could cause postoperative cerebrospinal fluid leakage. Meanwhile, most tumor bases of petrous apex meningioma are located below trigeminal nerve, therefore neurosurgeons have to remove part of petrous bone to expose the tumor base in a risk of damaging carotid canal [3]. With usage of the intradural approach, neurosurgeons could remove less petrous bone than the extradural approach based on the location of the tumor base with a direct view [6]. Thus, the authors present the intradural modification of Kawase approach for petrous apex meningioma that have been performed from February 2012 to May 2017, and an analysis of the surgical results.
MATERIALS AND METHODS
General case information
From February 2012 to May 2017, we performed a retrospective analysis of 16 patients with petrous apex meningiomas who underwent the intradural transpetrosectomy practiced by the senior author in the department of neurosurgery at Renji Hospital. All procedures performed in the study involving human participants were in accordance with the ethical standards of Renji Hospital. And Institutional Review Board approval of Renj Hospital was obtained for this study. The case series consisted of six males and 10 females with a mean age of 43.5 years (range, 30-76). A summary of the clinical findings and signs were listed in Table 1. The mean duration of symptoms was 8.2 months (2-120 months). Of the 16 cases, seven were located in the left side and the remaining were located in the right side.
Imaging manifestations
Contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI) have been obtained in all patients (Fig. 1A-C). Contrast-enhanced T1-weighted MRI gave the most accurate information for planning the surgical approach, including the dural attachment zone, maximal dimensions of the tumor, displacement of the brainstem, displacement or engulfment of the basilar arteries and invasion of the cavernous sinus. The maximal tumor dimensions ranged from 21 to 42 mm. Posterior cavernous sinus extension in six cases, displacement of basilar arteries in 10 cases and compression of the brainstem in 13 of the 16 cases were noted. T2-weighted MRI depicted the interface between the tumor and the brainstem, such as hyper-intensive signal within the brain parenchyma indicated disruption of the blood-brain barrier and difficulties in resecting the tumor from the brainstem might be anticipated. Tumor remnant was left in six patients due to these situations.
Surgical technique
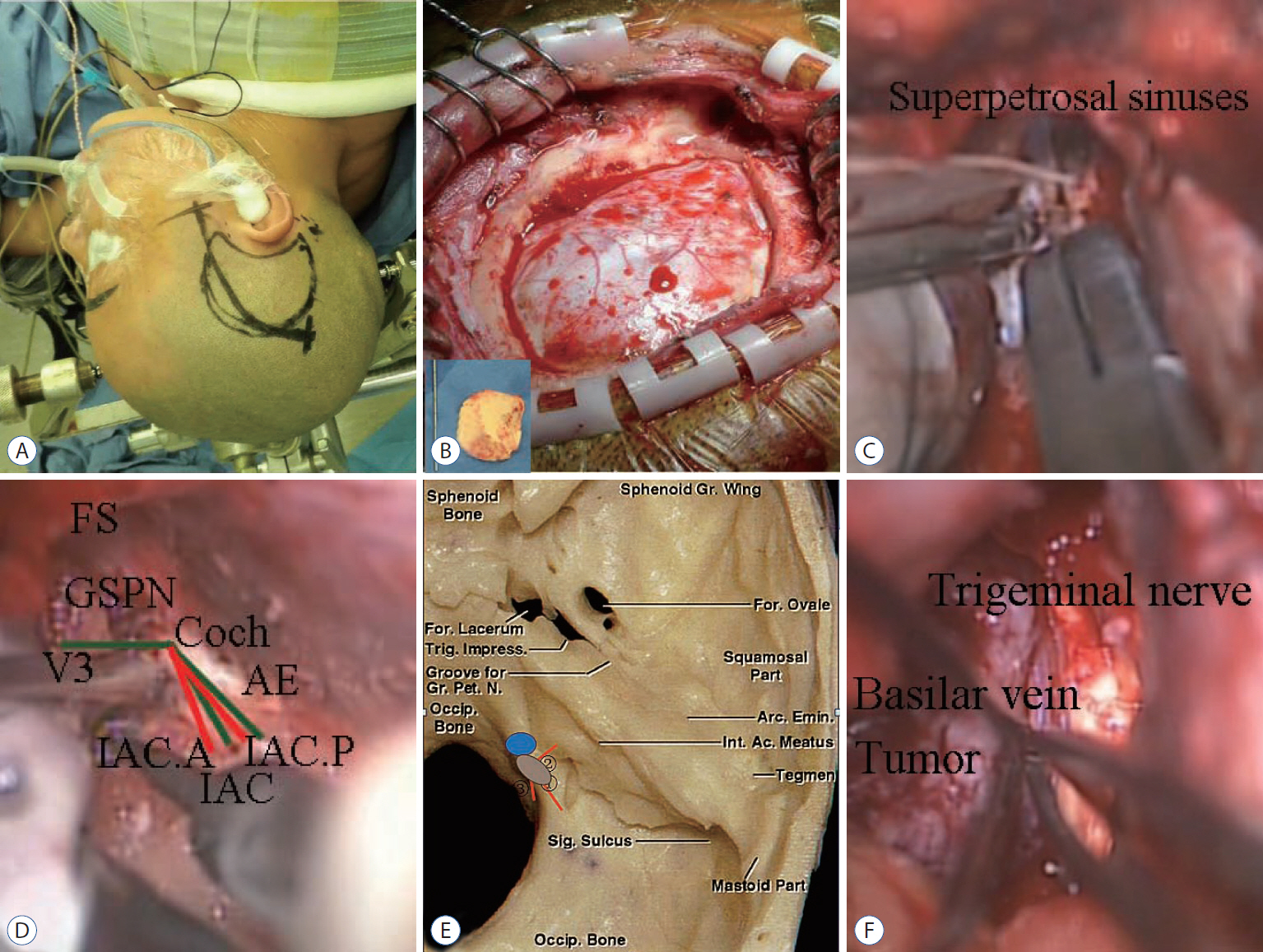
The patient was placed in the lateral decubitus position with the ipsilateral shoulder slightly elevated (Fig. 2A). The skin incision began 0.5 cm below the zygomatic arch, 1 cm anterior to superficial temporal artery, and extended 9 to 11 cm superoposteriorly based on the location of tumor. Then superficial and deep temporalis fascia and temporalis muscle was incised and elevated with a self-retaining retractor.
Root of zygoma and suprameatal ridge were drilled separately. Next, bone flap was removed with rongeurs as needed to middle point of zygomatic arch anteriorly, intersection point of suprameatal ridge and extended line of zygomatic arch posteriorly, superior temporal line superiorly and zygomatic arch inferiorly, until bony opening was nearly flush with the floor of the middle cranial fossa (Fig. 2B). Then, dura was open curvely and bottom of temporal lobe was elevated to expose tentorium. Dissected the arachnoid membranes of cistern ambiens and released cerebrospinal fluid. Incised tentorium behind the entrance of trochlear nerve. Freed superior petrosal sinus from superior petrosal sinus groove to clip it with titanium clips and ligated it later (Fig. 2C). During surgery, we utilized technique of Garcia-Ibanez with the bisection of the angle between the GSPN and arcuate eminence to identify the direction of the internal acoustic canal (Fig. 2D). To expose the tumor base, we have to removal part of petrous bone from the trigeminal nerve pressure trace to the internal auditory canal, not exceeding 1.5 cm laterally, from the petrous edge to the petrous section of internal carotid artery, not exceeding 2 cm anteriorly, and from the petrous tip to the petrosal sinus, not exceeding 1 cm inferiorly (Fig. 2E).
Tumor base of petrous apex meningioma was often found at the bottom dura of MeckelвҖҷs cave near superior petrous sinus, which should be coagulated before internal decompression was performed. Incised MeckelвҖҷs cave to resect residue tumor inside. Oculomoter nerve, trochlear nerve, abducens nerve, trigeminal nerve and facial nerve were often adhered to tumor (Fig. 2F). Tumor was debulked with microscissor and aspirator by a piecemeal technique. After meticulous bleeding control, closure was performed in layers.
RESULTS
The intradural transpetrosectomy was performed in all 16 cases with brainstem auditory evoked potentials monitoring. In all patients, tumor removal was classified based on postoperative contrast-enhanced MRI (Fig. 1D-F), and gross total resection was considered to be achieved if there was no enhancement present. According to Simpson grading system, grade I resection (tumor, dura, and bone) was achieved in four cases (25%). Grade II resection (tumor and dura) was achieved in six cases (37.5%) and there was no recurrence in this two group. Grade III resection (tumor) was achieved in six cases (37.5%) due to firm consistency and carvernous sinus invasion or brainstem adherence. Among this group, two patients experienced regrowth of the tumor which have been confirmed by the pathological results (Fig. 3) and underwent a second operation. The postoperative complications improved during a mean follow-up period of 34.4 months (range, 6-66). The mean KPS improved from 85.6 preoperatively to 91.9 postoperatively, and all data was handled by SPSS version 20.0 for stastical analysis (SPSS Inc., Chicago, IL, USA). Using Wilcoxon rank testing indicated, the difference between preoperative and postoperative KPS score was statistically significant (p=0.039).
DISCUSSION
The advantages of intradural transpetrosectomy approach compared to conventional Kawase approach are 1) an arc incision begins from 1 cm anterior to superficial temporal artery and stops above the auricle in intradural transpetrosectomy with a nicer appearance and shorter operation time, compared with a rectilinear incision around the ear in conventional Kawase approach. 2) Temporalis muscle is retracted bilaterally in intradural transpetrosectomy approach which can better neurosurgeonвҖҷs vision of middle fossa, compared with temporalis muscle reflected inferiorly in conventional Kawase approach. And 3) middle meningeal artery and dorsal meningeal artery are exposed better and earlier. After obstructing the blood supply of petrous apex meningiomas, tumor will be easily resectable and surrounding structures can be protected during the process.
In this intradural transpetrosectomy, there is still debates regarding several steps and willed be discussed as followed. First, could superior petrous vein (SPV) be sacrificed? Superior petrous vein normally works as the drainage route from anterior cerebellar and brainstem venous system, which has four tribulates including anterior pontomesencephalic group, posterior mesencephalic group, tentorial group and petrosal group. If there is not enough space for operation, neurosurgeons should sacrifice veins after assessing the size of the veins [4]. Zhong et al. [26] claimed that veins with a diameter less than 2 mm could be coagulated and cut without risk. The vein of the cerebellopontine fissure, which has a diameter of 2.6 cm as the largest common stem of SPVs in the petrosal group, is often found coursing along the posterior surface of petrous apex meningiomas and should not be sacrificed. Conversely, the tributaries of the tentorial group or the posterior mesencephalic group could be sacrificed [13]. Besides, the superior petrosal vein is either displaced or compressed by meningioma, resulting in the formation of collateral veins, and therefore superior petrosal vein can be safely sacrificed in such cases [17,20]. No patient in this study developed a severe ipsilateral cerebellar edema or brainstem shift due to occlusion of the superior petrous vein.
Second, how to dissect greater superficial petrosal nerve? Back-to-front or front-to-back? Greater superficial petrosal nerve (GSPN) is an important landmark for identifying internal acoustics canal and drilling petrous bone. GSPN are prone to injuries during drilling as it courses to the geniculate ganglion, which could cause facial nerve palsy. Traditional surgical literature recommends to dissect GSPN from back-to-front, but it is infeasible to control traction forces on the proximal portion of the GSPN, including the geniculate ganglion [23,25]. On the other hand, front-to-back dissection has some advantages. At foramen ovale which is easily identified, it is simple to dissect the cleavage plane between the meningeal dura and the outer dura. Following trigeminal nerve from foramen ovale, the dura portion of the GSPN is located 7.5 mm medially and outer dural layer can be readily elevated from GSPN. Neural tissue is protected because front-to-back dissection leaves a defined endosteum coving the GSPN [8].
Third, should meningioma inside cavernous sinus or adhered to brainstem be totally removed? Most neurosurgeons worried that removing tumors in these places would cause paralysis of cranial nerves, especially glossopharyngeal nerve and vagus nerve [16]. Besides, neurosurgeons even like Sammi believed few patients with a efficacious subtotal removel had clinical progression and death [19]. However, a study lasting more than 4 years indicated that overal growth rates of petroclival menigiomas in patients managed conservatively were 0.81 mm/year in diameter [14]. In addition, meningioma in cavernous sinus and brainstem isnвҖҷt often adhered tightly to the surrounding tissues and solid in consistency, so the preferred choice is complete resection of meningioma. Meanwhile, radiotherapy for meningioma could induce intratumoral necrosis, peritumoral edema and second malignancy, so the preferred choice is complete resection of meningioma [10,11].
Intradural transpetrosectomy is ideal for petrous apex meningioma, especially for those with a predominant middle fossa extension, which can save much time to expose tumors and provide more surgical freedom when dealing with trigeminal nerve as compared with standard retrosigmoid approach [21]. But this approach is not ideal for tumors at the posterior fossa, because bone window is relatively small to provide space as a corridor to the posterior fossa [7,22]. Furthermore, it is not ideal for tumors at sella region and cerebellopontine angle due to the vein of Labbe on the dominant side being at high risk of injury, which is the main reason for temporal edema and postsurgical bleeding.
CONCLUSION
The intradural transpetrosectomy is an intradural modification of the conventional Kawase approach with less complications and better visions compared with the conventional Kawase approach, which is ideal for petrous apex meningioma. During this approach, superior petrous vein could be sacrificed except the vein of the cerebellopontine fissure and the common stem. Dissecting greater superficial petrosal nerve by front-to-back is recommended with less traction injuries. Meanwhile, most meningioma inside cavernous sinus or adhered to brainstem could be totally removed.