INTRODUCTION
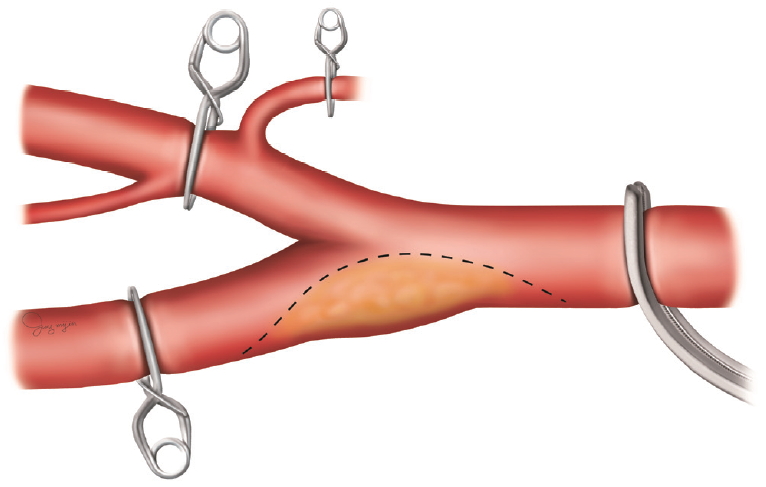
Carotid endarterectomy (CEA) is an effective surgical procedure for preventing ischemic stroke in selected patients with symptomatic or asymptomatic carotid stenosis [2,16,17]. But CEA has the risk of perioperative ischemic complications due to deliberate artery occlusion during clamping of the internal carotid artery (ICA) and thrombosis due to distal low flow [12,15]. To maintain cerebral blood flow during carotid clamping, some neurosurgeons routinely use a shunt, while others use a shunt selectively based on transcranial Doppler, electro encephalography, carotid stump back pressure, or neurological changes under local anesthesia [1]. However, the shunt procedure also leads to complications such as distal embolic events during shunt placement, arterial dissection, acute occlusion, and difficult exposure of the distal end of a high plaque [1,4,14]. Overall, the use of shunt is still controversial, and some neurosurgeons do not use a shunt at all [9]. At our institution, we used two modified closure methods of incision on the carotid artery instead of using a shunt to reduce the cerebral ischemic period during CEA. In conventional CEA, the ICA, the common carotid artery (CCA) and the external carotid artery (ECA) are clamped in that order. And then the entire process of endarterectomy is performed in the condition that the ICA, CCA and ECA are clamped. After complete closure of the endarterectomy site, the clamps are removed in the reverse order of clamping (Fig. 1). At our institution, we are exploring ways to reduce the carotid artery clamping time by removing the clamp of the ICA or ECA before finishing the complete suture of the arteriotomy site. In this paper, we introduce two methods with cases.
MATERIALS AND METHODS
This study design was approved by the Institutional Review Board of Chonnam National University Hospital (CNUH-2020-038) and fulfilled all of the requirements for patient anonymity. We retrospectively reviewed total 55 cases who underwent modified suture techniques during CEA at our institution between June 2018 and November 2019. We used two modified closure methods of incision on the carotid artery and each method is described below with a case.
Surgical technique 1 with a case
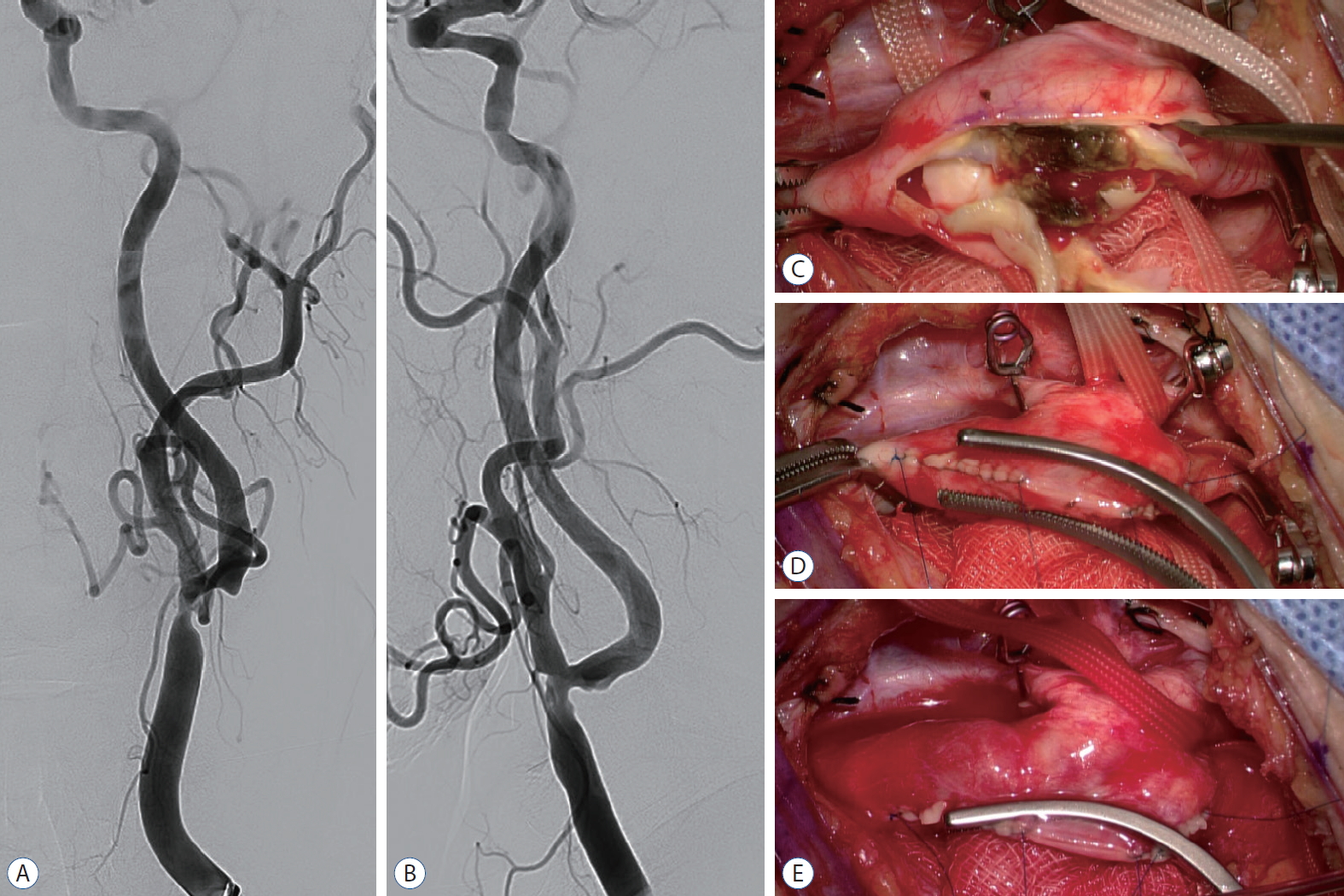
A 79-year-old man presented with recurrent syncope. He had a history of hypertension and diabetes mellitus. His neurologic examination revealed no deficit. There was no sign of acute cerebral infarction on the magnetic resonance imaging (MRI). However, the magnetic resonance angiography (MRA) demonstrated severe stenosis of the left CCA and ICA. Cerebral angiography revealed 55% segmental moderate stenosis (The North American Symptomatic Carotid Endarterectomy Trial, NASCET) in the left distal CCA, including the left ICA origin site (Fig. 2A and B). The plaque appeared unstable because of accompanying luminal irregularity, which led to our decision to perform a CEA.
Under general anesthesia, the patient was placed in the supine position. Intraoperative monitoring devices were used to check the motor evoked potential (MEP) and regional oxygen saturation (rSO2). The patientвҖҷs head was placed on a gel doughnut, and slightly extended and turned 15 degrees to the right. A curvilinear incision was made along the anterior border of the sternocleidomastoid muscle. And then the dissection was performed toward the carotid artery. After identification of the ICA, CCA, and ECA, the clamps were placed. The ICA and ECA were closed with Sugita clips, and CCA was occluded with a Satinsky clamp. The arteriotomy was performed on the atheroma and extended to ICA and CCA side, until normal lumens were identified at both sides. Intraoperative findings of the atheroma indicated an unstable plaque. The atheroma had a necrotic core (Fig. 2C), and careful endarterectomy was performed. ICA stump back pressure after ECA and CCA clamping was low at 12/11 mmHg. The baseline rSO2 was 57% before ICA clamping and decreased to 46% immediately after the ICA clamping. During endarterectomy, systolic blood pressure increased to over 150 mmHg; however, the rSO2 was still remained near the high 40%. To prevent ischemic complications, we had to open the ICA as soon as possible as a shunt was not used. After removing the residual debris and irrigating the endarterectomy surface, the primary closure was started. A continuous locking suture was begun at the distal end of the arteriotomy and advanced to distal a third. Another suture was started at the proximal end of the arteriotomy and ran to the proximal a third in the same manner. The remaining middle third was not sutured. The ICA was opened briefly to allow backflow and to wash out debris. The same procedure was performed for the ECA and then for the CCA. Afterward, the unsutured middle third was isolated from the arterial lumen by placing curved a Satinsky clamp (Fig. 2D). The clamps on the ECA, CCA, and ICA were removed in this order (Fig. 2E). By isolating the unsutured arteriotomy site with the Satinsky clamp, we were able to open the ICA before finishing the primary closure, and the rSO2 immediately recovered to 64%. The surgery was completed uneventfully. During the entire CEA, the MEP was maintained in the normal range, and there was no complication after the surgery.
Surgical technique 2 with a case
A 74-year-old man with intermittent headache and dizziness underwent a brain MRI, MRA, and neck computed tomography angiography (CTA). The MRA and CTA revealed severe stenosis of the proximal cervical ICA (NASCET 80 %) with calcification and ulceration (Fig. 3A and B). The stenosis was severe, and ulceration was present. Therefore, we decided to perform a CEA.
Under general anesthesia, preoperative preparation was carried out in the same way as in the above-described case. Intraoperative monitoring devices for MEP and rSO2 were used, and the operation was performed on the patientвҖҷs left neck. After identification of the ICA, ECA, and CCA, clamps were placed on the ECA and CCA. The ICA stump back pressure was 60/37 mmHg. After clamping of ICA, a conventional endarterectomy was performed, which revealed that the plaque was unstable (Fig. 3C). After removing the atheroma and the residual debris and irrigating of endarterectomy surface, primary closure was initiated. In this case, a continuous locking suture was started at the proximal end of the arteriotomy and advanced distally. When the suture reached around the carotid bifurcation, the ICA, ECA and CCA were opened for a few seconds to wash out debris. Then, the ICA and the unsutured site were isolated from the CCA and ECA by placing a curved Satinsky clamp crossing from the sutured site to the carotid bifurcation (Fig. 3D). The next step was opening the CCA and ECA (Fig. 3E). As the ECA has multiple anastomoses with the ICA and its branches, the ischemic risk could be reduced by opening the CCA and ECA early. Following this, the suturing was continued. The rSO2 was 60% just prior to the ICA clamping, decreased to 56% after ICA clamping, maintained around 55% during the procedure, and increased to 60% after opening the CCA and ECA. The ICA stump back pressure measured before the last suture also increased to 82/48 mmHg. The surgery was completed uneventfully without any postoperative complications. The MEP was maintained within the normal range during the entire procedure.
RESULTS
In our institution, technique 1 was applied to 10 patients and technique 2 was applied to 45 patients from June 2018 to November 2019. There was only one case of perioperative complication. The patient was 80-year-old man and underwent CEA using technique 2 on right carotid artery without a shunt. After the surgery, he presented left hemiplegia. However, there was no acute infarction or hemorrhage in brain MRI and CTA. We assumed that the symptom was caused by hyper-perfusion. After rehabilitation, the patient recovered to motor grade IV.
DISCUSSION
CEA is an effective surgery for primary or secondary prevention of ischemic stroke in selected patients with symptomatic or asymptomatic carotid stenosis. The benefits of CEA have been demonstrated in major trials [2,16,17]. The benefit of the CEA procedure relies on the low perioperative stroke rates [6,8,16]. According to Riles et al. [10], among 3062 primary carotid endarterectomies, perioperative stroke occurred in 66 cases (2.2%). Ten of these cases were related to ischemia during carotid artery clamping [10]. Carotid occlusion during clamping in CEA could cause cerebral hypoperfusion or intraoperative thrombosis; both mechanisms are related to perioperative strokes [15]. As the efficacy of CEA is determined by the minimization of perioperative stroke rate [5], it is important for surgeons to reduce the cerebral ischemic time during CEA. Many neurosurgeons use a shunt to prevent cerebral ischemic complications. However, by placing a shunt, potential problems, such as dissection of the arterial wall, difficulty of securing a shunt, or dislodgement of the shunt, may arise [10]. The use of shunting may also cause air embolism at shunt introduction [15]. Therefore, the use of shunting is still controversial. Some neurosurgeons do not use a shunt at all and have reported good results without a shunt [3,9,11,15]. In our institution, we do not use a shunt, but aim to reduce the carotid clamping time to prevent cerebral ischemia. To achieve this, we have used two types of modified suture techniques for arteriotomy to reduce the cerebral ischemic time.
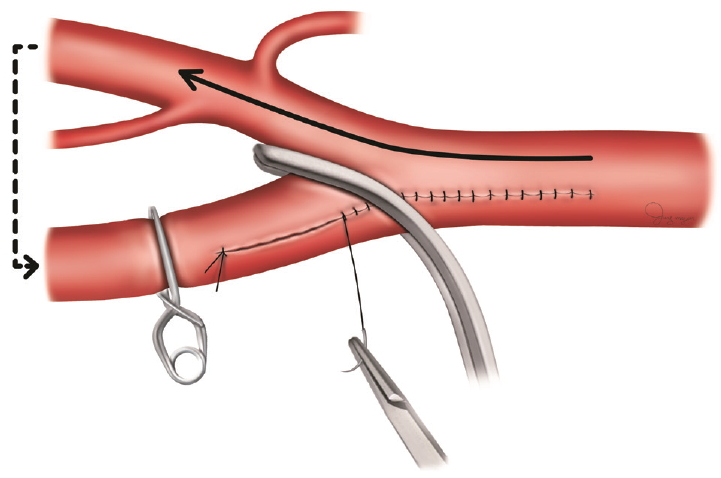
Technique 1 is the early opening of ICA using a Satinsky clamp before finishing the suture of the arteriotomy. The method is as follows : 1) after removing the plaque, the suture starts at the distal end of the arteriotomy and advances to the distal third of arteriotomy with a continuous locking suture. 2) Another suture starts at the proximal end of the arteriotomy and proceeds to proximal third with a continuous locking suture. 3) Open the ICA clamp temporarily to wash out debris and then sequentially open the ECA, CCA clamp for a short time. 4) Isolate the unsutured middle third with a curved Satinsky clamp from the carotid artery lumen. 5) Open the ECA, CCA, and ICA clamp in that order. And 6) finish the suture at the middle third and then open the Satinsky clamp. To enable a smooth blood flow from the CCA to the ICA, the curved Satinsky clamp should be applied at the CCA. If the Satinsky clamp is applied at the ICA, the ICA would collapse because of its small lumen. Technique 1 is applicable to cases where the atheroma plaque is extended to the CCA site (Fig. 4). In case 1, ICA clamping time was 22 minutes and 55 seconds. It took an additional four minutes and 53 seconds from the ICA unclamping to the removal of the curved Satinsky clamp for finishing the remnant suture. We could reduce the cerebral ischemic time by approximately 5 minutes before finishing the arteriotomy suture, which is a reduction of 18.7%. Futhermore, the rSO2 was also improved. After ICA clamping, rSO2 dropped from 57% to 46% and immediately rose to 64% after applying the curved Satinsky clamp and unclamping of the ICA.
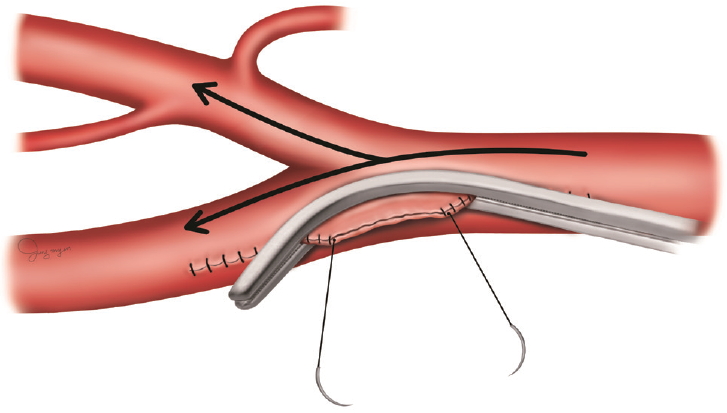
Technique 2 uses the anastomoses between the ICA and the ECA. The ipsilateral ECA has multiple anastomoses with the ipsilateral ICA, which can be an important collateral in cases of ipsilateral ICA occlusion [7,13]. In technique 2, by opening the ECA clamp before finishing the arteriotomy suture, blood flow via ECA-ICA anastomoses could reduce brain ischemia. The method works as follows : 1) after removing the plaque, the suture starts at the proximal end of the arteriotomy and advances distally to around the CCA bifurcation with a continuous locking suture. 2) Open the ICA clamp temporarily to wash out debris and then sequentially open the ECA and CCA clamp for a short time. 3) Isolate the unsutured site at the ICA with a curved Satinsky clamp from the CCA and ECA. 4) Open the ECA and CCA clamp and allow blood flow to the ECA. And 5) finish the suture at the ICA and then open the ICA clamp and the Satinsky clamp. Technique 2 is applicable to cases when the arteriotomy is not extended far to the CCA because the plaque is located mainly at the ICA. The shorter the incision on the CCA, the faster the Satinsky clamp can be applied. In case 2, the total clamping time was 26 minutes with six minutes from the unclamping the ECA and CCA to finishing suture and unclamping the ICA. We could supply blood flow via the ECA collaterals 6 minutes before finishing the complete closure of the arteriotomy site. The rSO2 decreased from 60% to 56% immediately after the ICA clamping, but rose back to 60% after ECA unclamping. ICA stump back pressure improved from 60/37 mmHg after ICA clamping to 82/48 mmHg after ECA unclamping. In case 2, in our opinion, the collateral flow via ECA and the increased systolic blood pressure from 120 mmHg to more than 160 mmHg after ICA clamping could have affected the result of equal or more improved rSO2 and ICA stump back pressure after opening the ECA only than the rSO2 and ICA stump back pressure before ICA clamping.
It is unclear whether the modified suture method alone can improve the functional outcome after the CEA because many other factors can affect the results, such as blood pressure and the flow from contralateral ICA. However, we think that the modified suture methods can reduce the cerebral ischemia directly (technique 1) or via using collaterals (technique 2), and it might reduce perioperative complications due to the ICA clamp. Finally, the modified arteriotomy suture techniques are simple, and do not need other devices such as a shunt. Thus, the modified arteriotomy suture techniques do not cause severe complications. These methods are applicable to almost all cases of CEA.
CONCLUSION
CEA is the golden standard treatment for symptomatic and asymptomatic patients with severe carotid stenosis. The efficacy of CEA is determined by the minimization of perioperative complications. The modified arteriotomy suture techniques are simple and easy and could help reduce the perioperative stroke rate by reducing the cerebral ischemic time.