INTRODUCTION
Spinal epidural abscess (SEA) is a potentially devastating infection [7,17,23,26,28], with an estimated mortality rate ranging from 1.8% to 25%, and 45% of patients suffer from long-term neurological dysfunction [17]. These abscesses occur within the epidural space between the spinal dura and vertebral periosteum and can subsequently result in spinal nerve compression and vascular damage [28]. Hematogenous spread is also known to be the main entrance to the epidural space in half of these cases [3,23,28].
The treatment of choice for SEA generally is surgical debridement in combination with intravenous (IV) antibiotics [3,9,10,23,28,29]. There is little debate regarding whether urgent surgery is required for SEA with acute or progressive neurological deficits [23,26,27]. However, the optimal duration of antibiotic treatment has not been specifically studied in a randomized clinical trial, although 4-8 weeks is generally advised [28]. Furthermore, there is little information about the optimal duration of antibiotic treatment for subgroups with preoperative bacteremia. Some reported that positive blood culture or bacteremia was a risk factor for failure of medical management in SEA [23], and for recurrent infection in pyogenic spondylodiscitis [20].
In this study, we present the clinical characteristics of SEA accompanied by bacteremia preoperatively. All patients underwent open surgery as well as weeks of perioperative antibiotic treatment based on their identified organisms. The objective of this study was to investigate the effect of preoperative bacteremia on the clinical characteristics and duration of antibiotic treatment in SEA patients.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of the Kangwon National University Hospital (KNUH-2020-07-021) and was conducted according to guidelines outlined in the Declaration of Helsinki. We retrospectively reviewed the medical records and radiological data of 23 patients with SEA who underwent open surgery at the Department of Neurosurgery from March 2010 to April 2020 in a single teaching hospital (over 700 beds). A diagnosis of SEA was confirmed radiologically using magnetic resonance imaging (MRI) and by intraoperative findings. All patients had bacteremia preoperatively and underwent several weeks of perioperative antibiotic treatments based on their identified organisms until all symptoms of infection disappeared. Bacteremia was confirmed by peripheral blood culture, which was routinely performed for febrile patients during admission. The exclusion criteria included isolated discitis, isolated osteomyelitis, spinal tuberculosis and tuberculous SEA. We reviewed medical records, radiological findings, laboratory and microbiological results and statistically analyzed various parameters, including the duration of antibiotic treatments.
We obtained information regarding patient demographics, initial symptoms, pre- and posttreatment neurological status, treatment details (surgical and medical), comorbidities, other concomitant infections and previous medical histories, including invasive spinal interventions. The neurological status was checked initially at admission, immediately preoperatively and finally at final follow-up and was described according to the modified Rankin scale (mRS). We excluded invasive spinal interventions performed within 1 week prior to admission because they are less likely to cause SEA, considering the incubation period of microorganisms. The mean follow-up duration after termination of antibiotic treatment was 35.2 months, excluding three mortality cases.
We analyzed the radiological information, including the location and size of the SEA, severity of thecal sac compression, presence of osteomyelitis and accompanying abscess in psoas or paraspinal muscle. The radiological findings were based on the MRI, which was available in all patients. The location of the SEA was based on the nearest vertebral segment and was classified as ventral, dorsal or both. The size was measured according to the number of adjacent vertebral bodies (VB). The severity of thecal sac compression was defined as mild (below one-third of the total area of the spinal canal), moderate (one-third to two-thirds) and severe (above two-thirds) at the maximal compression level on MRI.
All patients underwent microbiological studies for both peripheral blood and surgical specimens acquired intraoperatively. Peripheral blood culture was performed before initiation of the empirical antibiotic treatment in all but one patient (95.7%). One patient had a blood culture on the day after antibiotic treatment started. Although the causative organisms were identified in all patients from preoperative blood culture, we also performed intraoperative cultures for surgical specimens in all patients. The administration of antibiotics was not routinely delayed for intraoperative culture specimen acquisition because the causative organisms had already been identified preoperatively. Thus, we acquired surgical specimens before starting antibiotic treatment in only six patients (26.1%). This was mainly because delayed diagnosis of SEA and other concomitant infections require urgent antibiotic treatment. We also reviewed the microbiological results of all concomitant infections and their causative organisms. Urinary tract infection (UTI) was regarded as significant only if the identified pathogens were the same as those from blood culture and the specimens were acquired by aseptic catheterization to rule out contamination of the sample.
We routinely performed urgent/emergent surgery for patients with either neurological deficits or compression of neural tissue due to large SEA. The surgical decision and procedures were performed on a case-by-case basis by two neurosurgeons, and the mode of surgery was determined considering the location and the size of SEA in addition to the medical condition of each patient. Initial empirical antibiotics were modified according to the final microbiological reports of drug sensitivity for identified organisms. The choice, initiation and termination of antibiotics were informed by the infectious disease physician. The patients were typically treated with IV antibiotics, and eight patients (34.8%) used both IV and oral antibiotics. In case of adverse effects, we modified antibiotics according to the recommendations of the infectious disease physician. We continued antibiotic treatment until the pain and fever disappeared and the laboratory findings normalized. However, some patients showed incomplete recovery of laboratory findings, whereas their clinical symptoms totally improved. Although most of them maintained IV antibiotic treatment, three patients (13.0%) changed IV to oral antibiotics because they wanted to discharge.
Whereas some patients underwent surgery in an earlier stage and continued weeks of antibiotic treatment thereafter, others maintained preoperative antibiotic treatment because the SEA was benign without neurological deficit or its diagnosis was delayed because of other concomitant infections.
Statistical analysis was performed using IBM SPSS Statistics Subscription (IBM Corp., Armonk, NY, USA). The Mann-Whitney U-test was used to determine the difference between the patients with and without concomitant infection for the interval to diagnosis and the interval to surgery. It was also used for analysis of the duration of antibiotic treatment according to various predisposing conditions. An one-sample t-test was used to determine whether the total duration of antibiotic treatment exceeded the conventionally advised duration (4-8 weeks). A p-value <0.05 was considered to be statistically significant.
RESULTS
Twenty-three patients were included in the current study, and the male : female ratio was 15 : 8. The ages of the patients at admission ranged from 39 to 94 years (mean, 68.9 years). The most common initial symptom was axial and/or extremity pain, which was reported in 12 patients (52.2%). The next most common symptoms were fever and weakness in six (26.1%) and three patients (13.0%), respectively. The time interval from initial symptom onset to admission ranged from 0 to 120 days (mean, 10.3 days). Two patients (8.7%) presented with dyspnea and melena admitted to the Department of Internal Medicine, and their MRI revealed SEA after aggravation of fever and back pain after several days (Table 1). Overall, 11 patients (47.8%) experienced fever before or after admission, and 13 patients (56.5%) had neurological deficits on admission or preoperatively.
Twelve patients (52.2%) had hypertension, which was the most common comorbidity. Five patients (21.7%), including two patients who underwent open heart surgery, had heart problem. Three patients (13.0%), including one patient who had kidney transplantation, had chronic kidney disease (Tables 1 and 2). Twelve patients (52.2%) had concomitant infections, including UTI, scrotal abscess, scapular abscess, infectious endocarditis and arteriovenous graft abscess. Six patients (26.1%) had spinal injections or acupuncture more than 1 week prior to admission. One patient underwent six spinal surgeries, and the last was spinal fusion performed 1 month prior to admission. Another patient had vertebroplasty 3 months prior and had undergone occasional spinal injection thereafter (Tables 1 and 3).
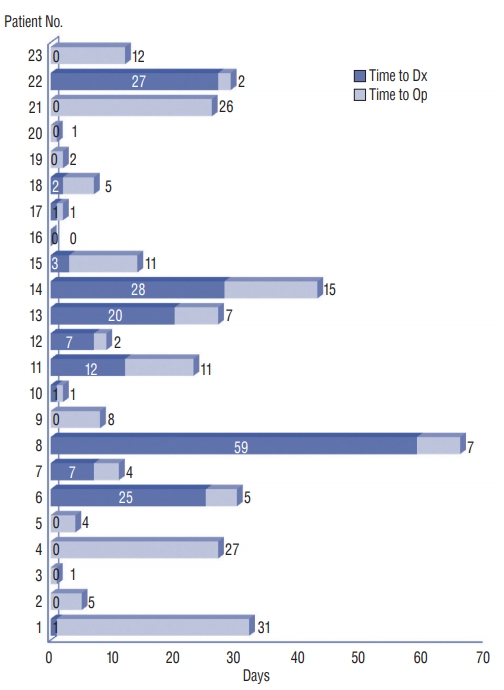
The SEA in our patients most commonly involved the lumbar spinal segment. Overall, seventeen patients (73.9%) had SEA in the lumbar, lumbosacral and thoracolumbar segment. The size of the SEA ranged from 1 to 6 VB (mean, 2.9 VB). MRI showed mild, moderate and severe compression of the thecal sac in five, 12, and six patients, respectively. More than half (60.9%) of the SEAs were located ventrally, and only 17.4% were located dorsally. Eighteen patients (78.3%) exhibited osteomyelitis along with SEA, and 15 patients (65.2%) presented with accompanying psoas or paraspinal abscess on MRI (Table 1). The time interval from admission to radiological diagnosis ranged from 0 to 59 days (mean, 8.4 days). Whereas 65.2% of SEA was diagnosed within 3 days, eight patients (34.8%) experienced delayed diagnoses (≥7 days), whose MRI was performed a mean of 23.1 days after admission (Table 2 and Fig. 1). Six of them had other concomitant infections, which masked SEA until further deterioration of pain or neurological deficits. The time interval from admission to radiological diagnosis was much longer in patients with concomitant infections than in patients without them (14.6±18.1 vs. 1.6±2.7 days). This difference was statistically significant (p=0.032).
The time interval from admission to surgery ranged from 0 to 66 days (mean, 16.6 days). Fourteen patients (60.9%) underwent delayed surgery more than 1 week after admission. These were due to delayed diagnosis and failed antibiotic treatment in eight and four patients, respectively. The time interval from admission to surgery was also longer in patients with concomitant infection than in patients without it (23.2± 18.6 vs. 9.4±10.7 days). And the difference was statistically significant (p=0.043). We also held early surgery because of poor general condition in another four patients, and two of them already experienced delayed diagnosis. Most patients (87.0%) underwent laminectomy and abscess removal via a posterior approach (Table 2). Two patients had additional surgery for spinal fusion in a few days, and another two patients had revision surgery due to wound infection and cerebrospinal fluid leakage. There was no perioperative morbidity or mortality.
Methicillin-sensitive Staphylococcus aureus was the most commonly identified organism in both peripheral blood (39.1%) and surgical specimen culture (30.4%). Methicillin-resistant S. aureus (MRSA) was the next most common organism, and more than one organism was identified in four patients (17.4%). Whereas all patients had bacteremia, no organism was isolated in surgical specimens from eight patients (34.8%) (Fig. 2). Isolated organisms from various concomitant infections were also compatible with the results from peripheral blood and/or surgical specimens in most patients (Table 3).
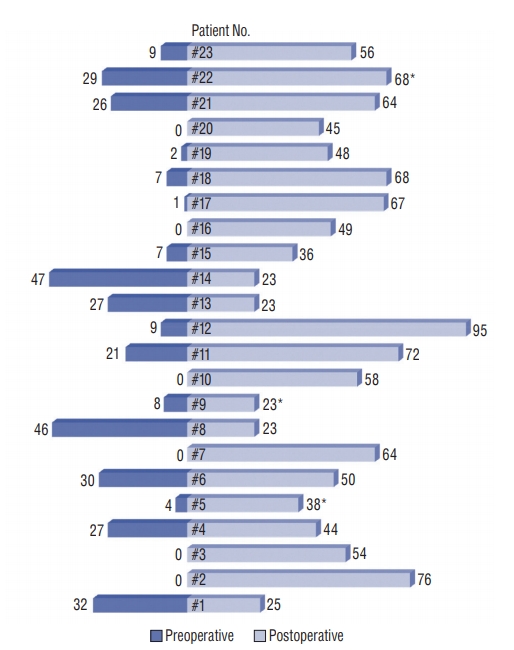
The duration of preoperative antibiotic treatment ranged from 0 to 47 days (mean, 14.4 days). While six patients (26.1%) did not receive antibiotic treatment until surgery, 12 patients (52.2%) received preoperative antibiotic treatment for more than 1 week, and their mean duration was 25.9 days. The duration of postoperative antibiotic treatment ranged from 23 to 95 days (mean, 50.8 days) (Table 2). The overall pre- and postoperative antibiotic treatment duration was 66.6±16.6 days, excluding three patients who died. This was longer than the conventionally advised period (4-8 weeks), which was statistically significant (p=0.010) (Fig. 3). Among various predisposing conditions, only psoas or paraspinal abscess was significantly related with prolonged duration of antibiotic treatment (p=0.038) (Table 4).
Nine patients (39.1%) maintained neurologically intact initial status (mRS score 0) until the final follow-up. Another nine patients (39.1%) showed neurological improvement, and eight of them completely recovered without any sequelae or recurrence (mRS score 0). However, two patients (8.7%) showed no neurological improvement until the final follow-up. Moreover, three patients died (mRS score 6); the causes of death were heart failure, subclavian aneurysm rupture and septic shock (Table 2).
DISCUSSION
We think that the negative culture result is mainly because of the low sensitivity of study or inadequate specimens, and it does not mean the absence of bacteria. Moreover, we also think that all patients with SEA have pathogens even though they are not identified in culture study. However, we are not sure that the patients with positive and with negative culture result should be treated in same manner. Otherwise, we are not sure they should be treated differently.
We were supposing that there may be some unknown factors which determine the positive or negative result in culture study. What we were interested in was them and their clinical significance, not whether the bacteria really exist or not.
The bacteremia can be an important sign because it may reflect the vigorous bacterial activity. Thus, we tried to find the significance of bacteremia especially in duration of antibiotic treatment. The primary purpose of this study is to investigate whether the bacteremia prolongs antibiotic treatment in surgical SEA group.
Bacteremia and SEA
The mechanism for SEA is most commonly hematogenous spread via bacteremia [28], although the majority of bacteria are cleared from the bloodstream without developing sepsis [21]. Spontaneous SEA is mostly a secondary complication of a primary spinal infection such as spondylodiscitis, spreading hematogenously via septic thrombosis of the epidural vein [19]. Of those with an unknown route of infection, some may have resulted from hematogenous seeding during a transient bacteremic episode [28]. We agree that the optimal duration of antibiotic treatment should be based on the patient’s risk of recurrence [22]. However, to our knowledge, it is unclear whether bacteremia is a risk factor for recurrence after antibiotic treatment in SEA patients.
Although Park et al. [22] found that bacteremia was not associated with recurrence after antibiotic treatment, almost half of their series were vertebral osteomyelitis without epidural involvement. Shah et al. [25] reported that bacteremia was not a risk factor for recurrence in 572 patients with SEA. However, more than 200 of them did not undergo surgery [25]. Kim et al. [18] showed that age older than 65 years, diabetes, MRSA infection, and neurological deficits were risk factors for failure of medical management in SEA. However, they did not mention bacteremia as a variable in their algorithm for the probability of failed antibiotic management of SEA. Although all patients in their study had SEA, none underwent surgical intervention. Thus, we believe that their results are difficult to apply directly to our SEA patients who underwent surgery because surgical debridement provides eradication of infectious tissues and shortens the duration of the antibiotic course [20,27].
In contrast, Patel et al. [23] and Lener et al. [19] documented bacteremia as a risk factor that predicts failure of medical treatment of SEA. However, Patel et al. [23] did not describe the details of antibiotic treatment, including the optimal treatment duration. Although our results provide little evidence regarding whether bacteremia is a risk factor for failure of antibiotic treatment, they demonstrate that bacteremia requires a significantly longer duration of treatment. However, we do not know clearly whether bacteremia itself is a direct cause of prolonged duration of antibiotic treatment or whether it is merely one coexisting sign of certain conditions that require prolonged treatment. Moreover, we do not completely understand whether bacteremia induces the deterioration of the general condition or vice versa. We believe additional studies need to be conducted to answer these questions.
Concomitant infection and delayed diagnosis
In our cohort, approximately one-third of patients experienced delayed diagnosis. We believe that this is mainly due to the presence of concomitant infections, which masked and distracted the awareness of SEA. The classic diagnostic triad of spine pain, fever, and neurological deficits defined as the initial descriptions of SEA are still considered the hallmarks of this disease [12]. Although the combination of pain near the spine with fever should be regarded as a warning sign of possible SEA [15,24], early identification is difficult given its infrequency and the nonspecific nature of early symptoms [12]. Moreover, the majority of our patients were elderly, whose initial symptoms and signs of SEA can be vague because of blunted immune responses [14]. Thus, we believe that the role of MRI should be emphasized and performed more readily to achieve early diagnosis. MRI is the most sensitive way to make the diagnosis [2,23], and especially in combination with gadolinium, now represents the method of first choice for diagnosis, making other diagnostic procedures essentially superfluous [24].
All delayed diagnoses resulted in delayed surgery in our patients, although another four and two patients also underwent delayed surgery due to failed antibiotic treatment and poor general conditions, respectively. The importance of early surgery has been supported by many studies over decades [4,10,11,15,23]. In contrast, Karikari et al. [16] explained that early surgery was unlikely to be related to better outcomes compared with conservative treatment. However, more than half of their patients presented with back pain alone and no objective motor weakness [16]. Although Adogwa et al. [1] also reported that early surgery was not associated with superior outcome when compared with IV antibiotic treatment alone, all their patients were over 50 years old and had multiple comorbidities and high perioperative risk.
Nine patients in our study received antibiotic treatments without initial recognition of the SEA, without close observation of neurological status as in other trials. One of them expired with irreversible neurological deterioration despite surgical decompression, which was performed after the SEA progressed. It is unclear whether concomitant infection is main cause of worse outcomes or, conversely, it is the results of poor general condition. However, accurate and timely diagnosis is paramount to the successful management and eventual resolution of SEA [10]. We strongly agree that a high index of suspicion is warranted in the diagnosis of SEA [5,14], and believe that this is especially the case for patients with concomitant infections.
Optimal duration of antibiotic treatment
Although there are some studies about the optimal duration of antibiotic treatment, they were mainly conducted in cases of vertebral osteomyelitis or spondylodiscitis, and information about SEA is very limited. A randomized controlled trial by Bernard et al. [8] showed that 6 weeks of antibiotic treatment was not inferior to 12 weeks of antibiotic treatment in patients with pyogenic vertebral osteomyelitis. Nevertheless, there is an overall lack of evidence-based data regarding the risk factors for recurrence [20]. Park et al. [22] found that MRSA infection, undrained paravertebral/psoas abscess, and end-stage renal disease were independent risk factors for recurrence in vertebral osteomyelitis. Thus, they suggested a shorter duration (6-8 weeks) of antibiotic therapy for patients without such risk factors, whereas prolonged duration (≥8 weeks) was recommended for patients with any of these risk factors [22]. However, only 38.2% and 51.3% of patients had epidural abscesses and underwent surgical intervention in their series, respectively [22]. Therefore, we believe that these results are difficult to apply directly to patients with SEA who underwent surgery as well as antibiotic treatment.
Although Lener et al. [19] also recommended that the duration of antibiotic treatment should never be less than 6 weeks in spinal infection, Li et al. [20] suggested that the duration of postoperative IV antibiotic treatment in spondylodiscitis could be reduced to 3 weeks. They also found that bacteremia and paraspinal abscess formation were the two independent risk factors for treatment failure. Whereas they recommended short-term (≤3 weeks) parenteral antibiotic treatment for patients without risk factors, the patients with bacteremia or paraspinal abscess were not indicative of short-term treatment [20]. Although only 37.3% of patients had epidural abscesses in their series [20], their risk factors were very similar to ours, which revealed bacteremia and psoas/paraspinal abscess required extended antibiotic treatment.
SEA and spinal infection
Although SEA is one subgroup of spinal infections, we believe that it should be managed differently because surgery is more frequently required in SEA and surgical intervention can affect postoperative antibiotic treatment and subsequent clinical outcomes [20]. Therefore, we believe that the information derived from vertebral osteomyelitis or spondylodiscitis should not be extrapolated directly to patients with SEA. There is a paucity of uniform recommendations about the optimal duration of antibiotic treatment, and it remains controversial with no prospective, randomized, double-blind clinical trials to date [13]. We think that it is difficult to establish standardized guidelines for antibiotic treatment in SEA, mainly because the SEA includes a very wide range of heterogeneous conditions in terms of size, severity and predisposing factors.
The incidence of SEAs was estimated to be 0.2-2.0 cases per 10000 hospital admissions [25,28], and it is increasing, having doubled in the last two decades [23,25]. Its increase is possibly due to IV drug abuse, long-term vascular access in conjunction with spinal instrumentation, increased use of epidural injections, an aging population with multiple comorbidities, and the availability of MRI [13,18,25,26,28]. We believe that the wide availability of MRI and the increased accessibility to the hospital facilitated the early diagnosis of SEA, which had been missed until the size and symptoms fully progressed. Although they resulted in early treatment and favorable outcomes, we believe they conversely increased the heterogeneity of the pretreatment condition.
Because of the wide range of pretreatment conditions, significant results might be diluted or masked if the patient groups are too heterogeneous. Thus, we believe that the patients should be selected meticulously based on their pretreatment conditions to minimize this selection bias. Otherwise, it would be unethical to perform a prospective or randomized controlled trial because of the significant morbidity [25]. We believe that our patients are homogeneous in that all of them had bacteremia and underwent open surgery.
Medical treatment in SEA
Medical therapy alone has been used in patients with very poor predictors, such as those unable to tolerate surgery owing to extremely poor medical condition or those with paralysis >48-72 hours if surgery is not needed for source control [28]. However, medical management for patients with SEA presenting without neurological deficits or spinal instability and with improving infection is a recent trend [6]. We think that these small and mild cases are likely to receive antibiotic treatment instead of surgery, which was increasingly found with the widespread use of MRI. Although the importance of early surgery remains unwavering [2,17], this once exclusively surgically managed entity is increasingly treated conservatively with antibiotics [7]. The notion that all patients with SEA require surgery has been recently challenged by reports of successful medical management of selected patients with SEA [18]. However, in conservative treatment, the opportunity to acquire abscess specimen is very limited and even if the abscess is acquired by aspiration biopsy, they are already likely to be influenced by previous antibiotic treatment. Therefore, we believe that the clinical information about bacteremia in SEA is more important than before because it is practically the only way to get fresh microbiological information in non-surgery group.
Although some authors have claimed good results after medical management in selected patients, progressive neurological deficits despite appropriate antibiotic treatment occurred in 19-23% of patients described in the literature [5]. Arko et al. [6] reported that medical management failed at rates ranging from 6-49%, possibly due to differences in patient selection. Patel et al. [23] described diabetes, leukocytosis, bacteremia and high C-reactive protein as risk factors for failure of medical management and reported an 8.3-76.9% failure rate. Moreover, those on medical treatment should be carefully monitored on a regular basis because they may develop rapid and irreversible neurological deterioration [6,14].
We provided scheduled antibiotic treatment preoperatively to four patients who eventually underwent surgery because their symptoms persisted or because the SEA progressed radiologically. One of them experienced neurological aggravation in the course of antibiotic treatment, which was detected immediately, and urgent surgery reversed the deficit. We agree that purely conservative treatment is an option for selected patients but is not indicated for the majority of cases [24].
Limitations
Our study has several limitations. First, this study included a small number of patients because of the rare incidence of SEA. Some significant findings might have been missed because the statistics were performed on a relatively small cohort, weakening the power of the conclusion. Considering its rare incidence, multi-center study can be an answer for additional large scale study. Second, there might have been some bias in the selection of patients, and some potentially important clinical information might have been neglected because of the retrospective nature of this study. Finally, the time of surgery and the duration of preoperative antibiotic treatment were different among patients, which might have resulted in bias. Some patients underwent surgery earlier, whereas others underwent surgery after weeks of antibiotic treatment. Nevertheless, our results strongly support the notion that the duration of antibiotic treatment should be prolonged in SEA patients with bacteremia, despite these limitations.
CONCLUSION
SEA accompanied by bacteremia required a longer duration (>8 weeks) of antibiotic treatment (p=0.010), and psoas or paraspinal abscess was related with prolonged antibiotic treatment (p=0.038). In addition, its diagnosis was more frequently delayed in patients with concomitant infections (p=0.032). We believe that the duration of antibiotic treatment should be prolonged for SEA with bacteremia and that a high index of suspicion is mandatory for early diagnosis, especially in patients with concomitant infections.