INTRODUCTION
Craniosynostosis is a condition of the premature fusion of one or more cranial sutures, which results in characteristic skull shape deformities and facial asymmetry accompanied by functional consequences such as increased intracranial pressure (ICP), visual impairment, deafness and cognitive deficits4,1112,1418). Craniosynostosis can occur primarily and secondarily. Premature fusion of one or more of the sutures is believed to be due to a developmental error during embryogenesis in primary craniosynostosis whereas secondary craniosynostosis is due to mechanical causes such as intrauterine compression of the fetal skull, metabolic causes, and the effect of teratogens. Approximately 85% of primary craniosynostosis cases occur as an isolated condition and the remaining 15% are a part of a multisystem syndrome10,13).
Imaging is essential for the accurate diagnosis, surgical planning, post-treatment evaluation and identification of coexisting anomalies and complications associated with craniosynostosis. Because of its superior bone depiction, computed tomography (CT) with three-dimensional (3-D) reconstruction is the primary imaging technique used in craniosynostosis. However, exposure to ionized radiation from CT scans, especially in infants, has led researchers to explore alternative imaging techniques and protocols for craniosynostosis including the use of ultrasonography, plain skull radiography and magnetic resonance imaging (MRI). Here we present imaging findings in patients with normal craniums, craniosynostosis and its mimics and discuss the optimal imaging technique for the diagnosis, treatment planning and follow-up of craniosynostosis.
REVIEW OF IMAGING FINDINGS OF NORMAL CRANIAL SUTURES AND CRANIOSYNOSTOSIS
Imaging findings of normal cranial sutures
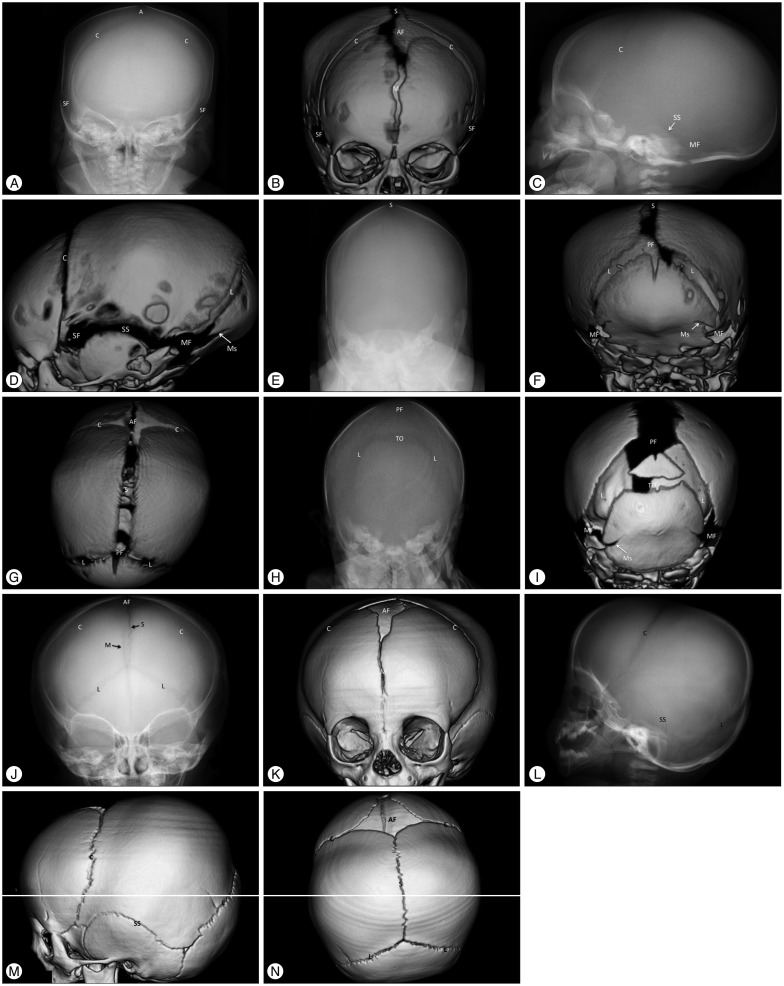
Cranial sutures exist along the margins of adjacent paired cranial bones, namely the frontal, parietal, temporal and occipital bones. Specifically, the metopic suture is between the frontal bones; the sagittal suture is between the parietal bones; the coronal sutures are between the frontal and parietal bones; the lambdoid sutures are between the parietal and occipital bones; and the squamosal sutures are between the parietal and temporal bones. Furthermore, the transverse occipital suture is between the squamous and supraoccipital segments of the occipital bone, which fuses in its midportion and forms the paired lateral mendosal sutures (Fig. 1)1). The fontanels are formed at the junctional boundaries of the cranial sutures. The cranial sutures in neonates appear wide open and fuse with age from back to front and lateral to medial with the exception of the metopic suture, which fuses from front to back. Normally the metopic suture fuses between 9 months and 2 years of age, followed by the coronal, lambdoid and then the sagittal sutures. These sutures fuse and disappear between 30 and 40 years of age as the growth of the cranial bones at the sagittal, coronal and lambdoid sutures ceases early in the second decade of life. The anterior fontanel fuses at approximately 18 months of age, and the posterior fontanel fuses between 3-6 months of age1,210,13).
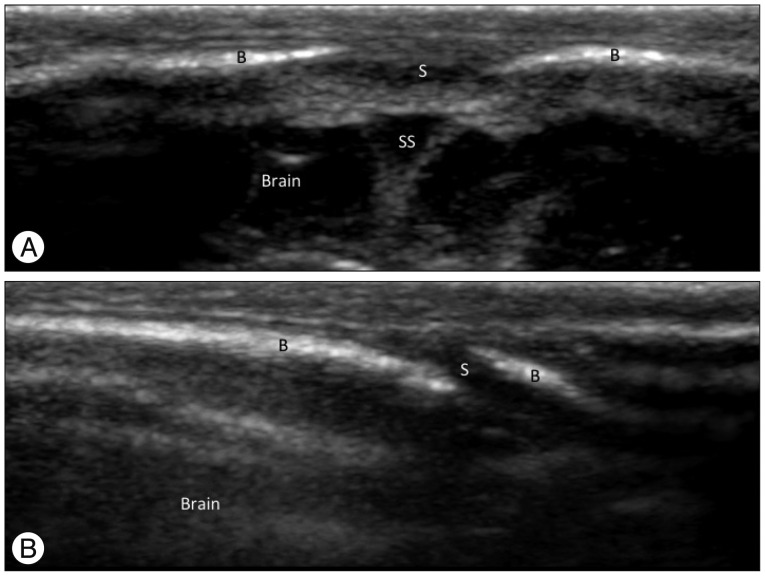
Normal skulls of children show variable appearances in the initial days and months after birth because brain growth accompanied with changes in the cranial bones and sutures is explosive during the first 2 years of life (Fig. 1). A normal patent suture is demonstrated as a radiolucent, serrated and nonlinear line on plain skull radiography and 3-D CT images (Fig. 1)1,210,13). Ultrasonography shows a normal patent suture as an uninterrupted hypoechoic fibrous gap between hyperechoic cranial bones with an end-to-end appearance on a transverse scan of the sagittal sinus and a beveled appearance on a transverse scan of the coronal and lambdoid sutures (Fig. 2)15,1920). Conventional MRI has typically been unreliable in identifying sutures individually. However, recently Eley et al.6) described a novel gradient echo MRI sequence ("Black Bone") that minimizes soft tissue contrast to enhance the bone-soft tissue boundaries and can demonstrate normal patent cranial sutures as hyperintensity distinguished from the signal void of the cranial bones (Fig. 3A).
Imaging findings of craniosynostosis
Premature fusion of the cranial sutures restricts cranial growth perpendicular to the affected suture with compensatory overgrowth along the other patent sutures. This results in the characteristic skull shape deformities noted in craniosynostosis. Diagnostic imaging is necessary to confirm the fused suture and to assess the accompanying skull deformities, intracranial pathology and other complications. A prematurely fused suture shows perisutural sclerosis, linearity, reduced serration, bony bridging or the absence of the suture on a plain skull radiography or CT image. Secondary signs of increased ICP, such as a "copper-beaten" appearance, are also observed in severe cases. Soboleski et al.20) reported the ultrasonographic findings of craniosynostosis as follows : 1) the loss of the hypoechoic fibrous gap between hyperechoic body plates; 2) an irregular, thickened inner sutural margin; 3) the loss of a beveled edge; and 4) asymmetric fontanels. On "Black Bone" MRI, the affected fused sutures are demonstrated as absence of suture (Fig. 3B)6).
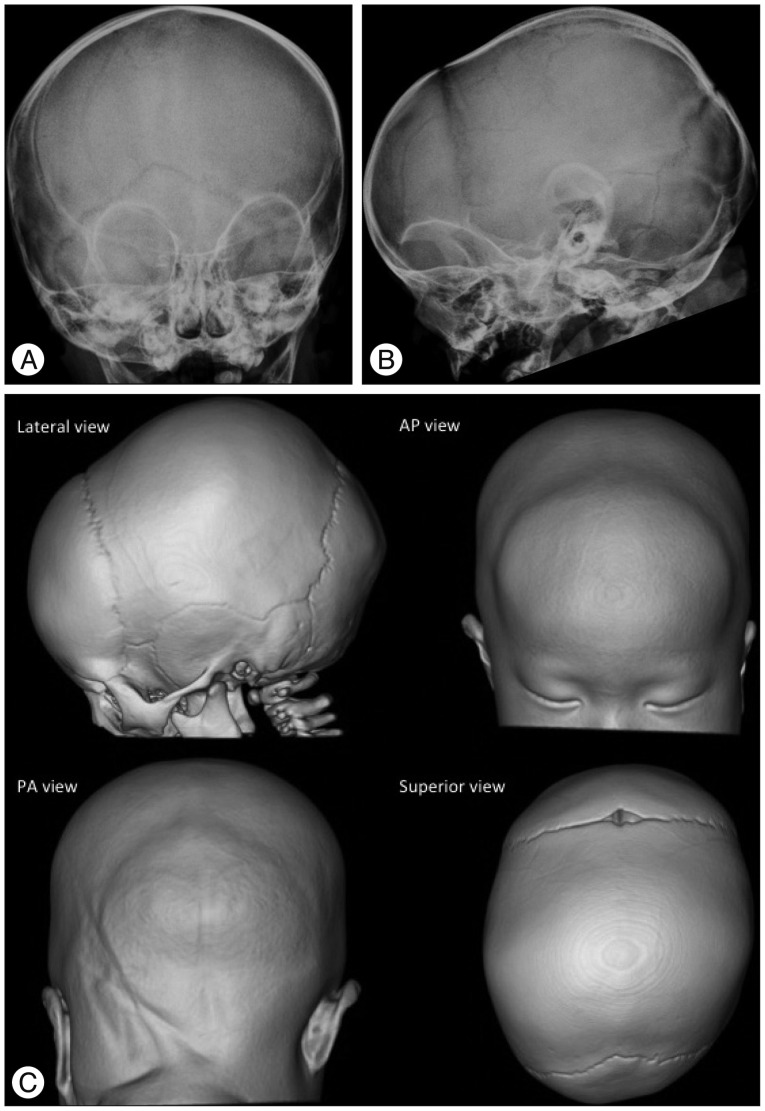
Sagittal synostosis
Restriction of growth perpendicular to the sagittal suture results in a narrow and elongated cranium with frontal bossing, occipital protrusion and ridging of the fused, heaped suture. This deformity is characterized by scaphocephaly (inverted boat with a keel), clinocephaly (flat cranium due to loss of cranial convexity), and leptocephaly (tall and narrow cranium) (Fig. 4).
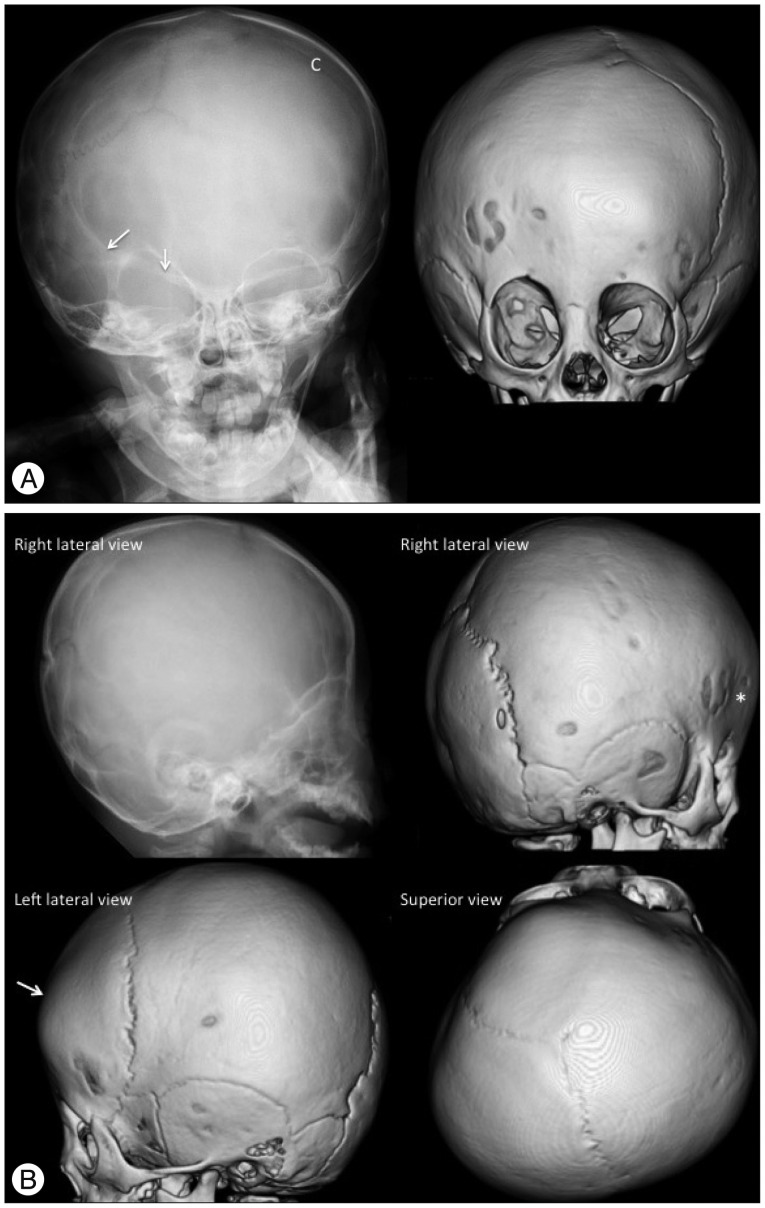
Coronal synostosis
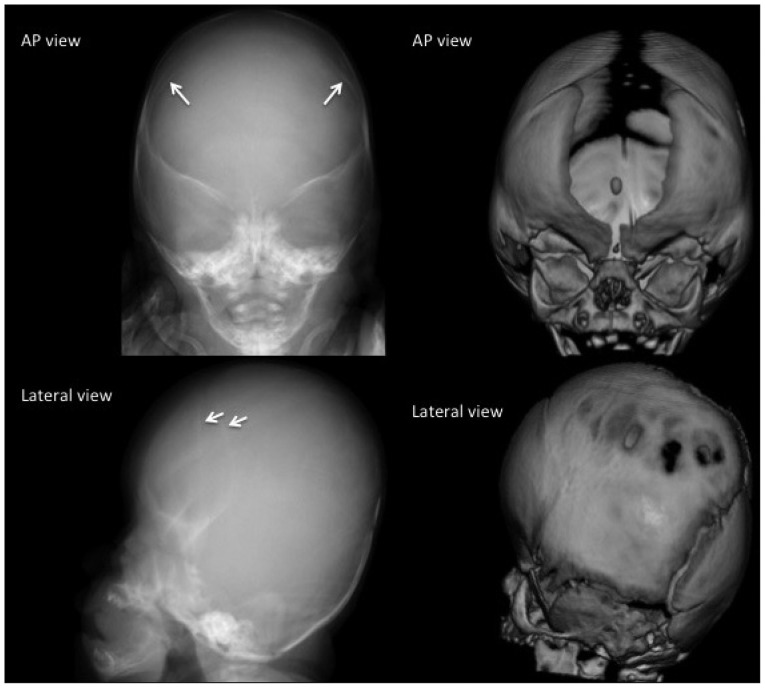
Coronal synostosis causes restriction of growth in the anterior-posterior direction, perpendicular to the coronal suture with compensatory overgrowth in the parietal direction, perpendicular to the patent sagittal suture. Unicoronal synostosis results in anterior plagiocephaly (oblique cranium) and appears as a shallow ipsilateral anterior cranial fossa with contralateral frontal bossing, an elevated roof and lateral wall of the ipsilateral orbit ("harlequin appearance"), a hypoplastic supraorbital ridge, elevated ipsilateral sphenoid wings, a contralaterally shifted anterior fontanel and facial asymmetry (Fig. 5). Bicoronal synostosis restricts skull growth in the anterior-posterior direction, which generally results in brachycephaly (short cranium). Isolated bicoronal synostois is relatively rare but is commonly observed in syndromic synostosis and is associated with upper and midface hypoplasia along with other craniofacial deformities and premature fusion of the skull base sutures leading to a small posterior fossa. Images reveal fused bicoronal sutures, shortened anterior-posterior and widened biparietal dimensions of skull, and bilateral "harlequin eye" deformity of the orbits with increased interorbital distance (hypertelorism) (Fig. 6).
Metopic synostosis
Premature fusion of the metopic suture results in a palpable ectocranial ridge or omega-shaped notch and a small anterior cranial fossa with a triangular pointed forehead (trigonocephaly) and parieto-occipital bossing due to bilateral constriction of the frontal bones. Imaging findings include decreased interorbital distance (hypotelorism), hypoplastic ethmoid sinus, and medially upward slanted orbital roof ("quizzical eye" appearance) (Fig. 7). Metopic synostosis should be differentiated from the metopic ridge, which is a normal variant of the metopic suture closure. One-third of cases of metopic synostosis are syndromic, with associated midline anomalies of the brain and the palate.
Lambdoid synostosis
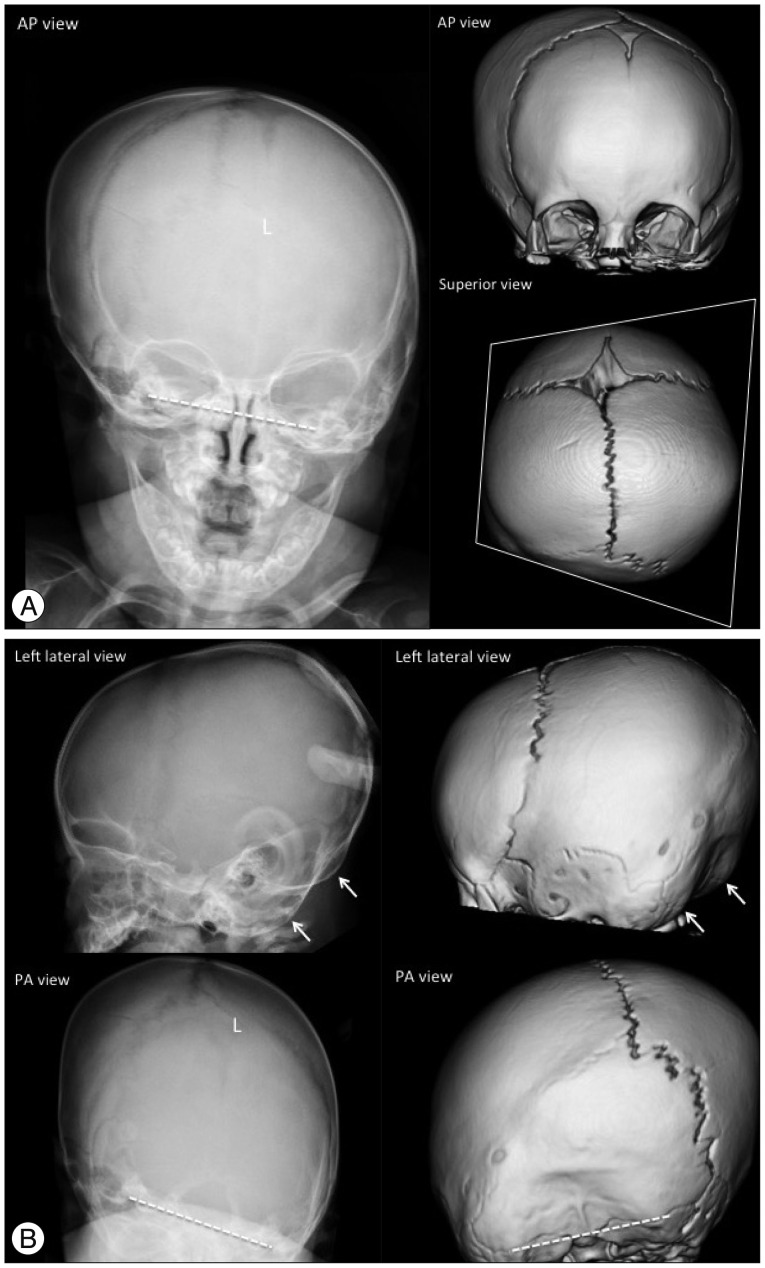
A unilateral premature fusion causes posterior plagiocephaly (oblique deformity of the posterior cranium), which is more commonly caused by positional problems compared to premature fusion of the cranial suture. Therefore, unilateral lambdoid synostosis should be differentiated from positional plagiocephaly. Images show ipsilateral occipitoparietal flattening, contralateral frontal and occipitoparietal bossing, a contralaterally shifted posterior fontanel, double contouring of the occipital margin due to a unilateral small posterior cranium, and a tilted skull base (Fig. 8). Bilateral fusion of the lambdoid sutures results in turricephaly (tall cranium; also known as oxycephaly and acrocephaly), with bilateral occipitoparietal flattening that leads to a small posterior cranial fossa and unimpeded compensatory growth at bregma.
Multisuture synostosis
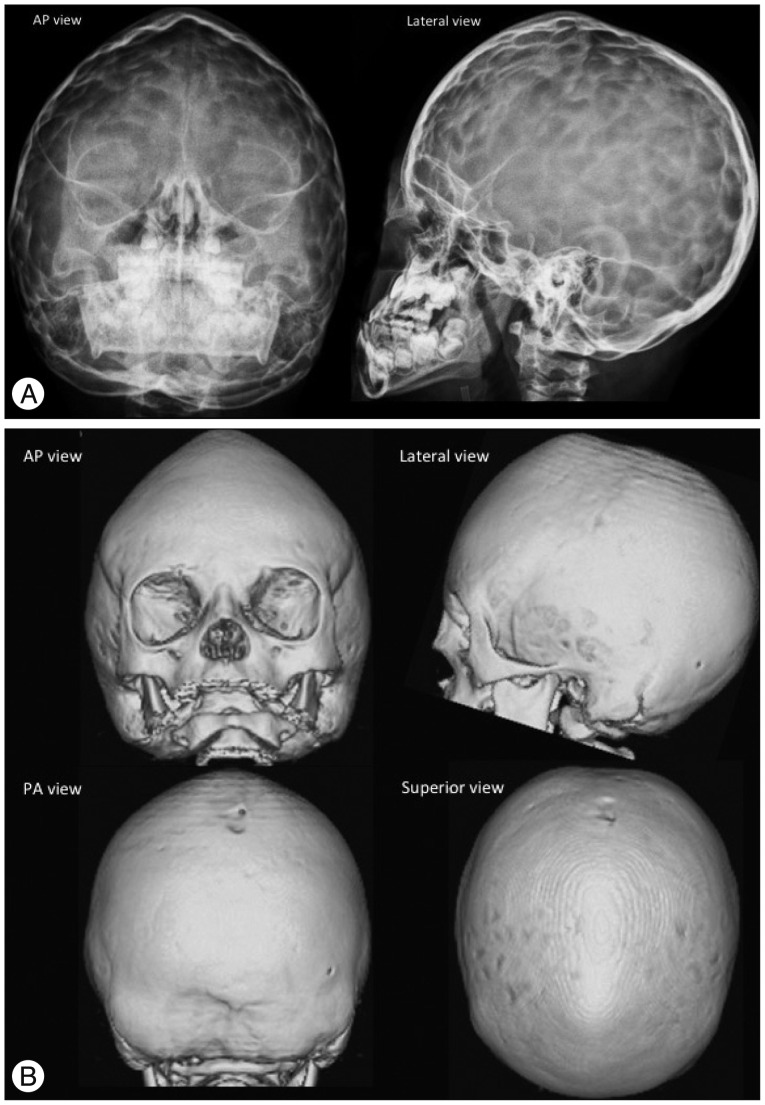
Multisuture synostosis is often syndromic. The patterns are variable according to the combination of sutures. Pansynostosis involves the sagittal, coronal and lambdoid sutures and is the most severe form resulting in the cloverleaf deformity of the skull (bulging of the temporal regions and severe proptosis, also known as Kleeblattschäde) or oxycephaly (a narrow and towering cranium) (Fig. 9). Bilateral lambdoid and sagittal synostosis is called Mercedes Benz synostosis. These complex forms of synostosis are often combined with other structural and functional complications.
Imaging findings of craniosynostosis mimics
Metopic ridge
Metopic ridge is a normal variant of the metopic closure that occurs in 4% of asymptomatic children between 0-18 months of age and should be differentiated from metopic synostosis. Infants with metopic ridge show a fused metopic suture without the other characteristic features of metopic synostosis such as trigonocephaly, hypotelorism, and the "quizzical eye" appearance23).
Deformational plagiocephaly
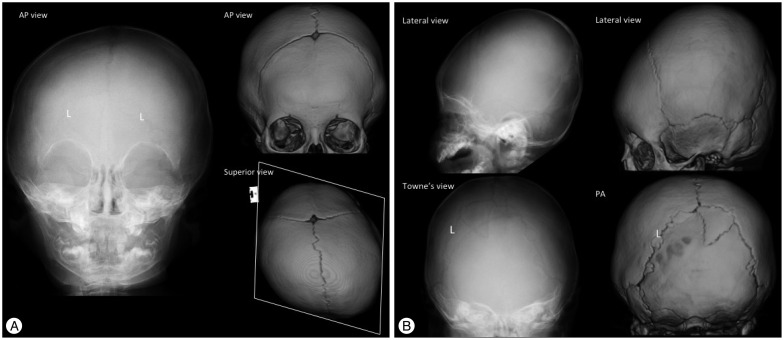
Positional deformities arise in infants from a preferential head positioning on one side during sleep and results in asymmetrical occipital flattening (posterior plagiocephaly). This is amenable to conservative treatment contrary to lambdoid synostosis, which requires surgical correction. The lambdoid suture in deformational plagiocephaly is patent and ipsilateral frontal bossing is combined as opposed to lambdoid synostosis (Fig. 10 compare with Fig. 8).
DISCUSSION FOR OPTIMAL IMAGING FOR DIAGNOSIS AND FOLLOW-UP OF CRANIOSYNOSTOSIS
Although 3-D CT has superior diagnostic value, concerns about the hazards of radiation exposure in children has led to a consensus to avoid or postpone radiographic CT imaging until the end of the first year of life or as late as possible in children with suspected or diagnosed craniosynostosis1,1516,17). The first step in assessing patients with an abnormal skull shape is a clinical examination in which almost all forms of monosutural craniosynostoses can be diagnosed. If there is a question of the diagnosis, ultrasonography is the technique of choice for diagnosis of neonates and infants. This simple and radiation-free technique can differentiate fused or patent sutures effectively and differentiate nonsynostotic pathology, such as positional skull deformities and molding, from craniosynostosis20,21). Increase of the width of the cranial sutures on serial sonograms may provide evidence for a possible increase in ICP, which is a major complication of craniosynostosis20). Schweitzer et al.17) investigated the individual features of all forms of craniosynostosis in plain skull radiography (AP and lateral images) to achieve proper diagnosis while avoiding the use of a CT scan. The effective radiation dose of plain skull radiography is approximately 0.01 mSv to 0.04 mSv. In monosutural craniosynostosis, plain skull radiography is only indicated in children with remaining diagnostic doubts after clinical and sonographic evaluation, immediately prior to surgery or in non-surgical cases after the first year of life to access for additionally affected sutures16). A CT scan may be unavoidable in complex (multisutural and syndromic types) or complicated types of craniosynostosis for treatment planning. The reported effective dose of radiation for a 3-D CT scan is in the range of 0.2 mSV to 2 mSV3,58,22). Recently, Ernst et al.7) reported that a 0.08 mSv 3-D CT protocol by using Model Based Iterative Reconstruction can be used in children with cranial deformities without compromising imaging quality. In a phantom study, Kaasalainen et al.9) achieved sufficient image quality using a CT protocol with an effective radiation dose of 0.02 mSv, which is comparable to the effective dose of plain skull radiography. Although this ultra-low-dose CT technique is not widely available presently and the diagnostic value for minor sutures is still questionable, these results are promising in children with complex craniofacial malformations who undergo repeated CT scans at the time of diagnosis and at various stages of surgical correction. The role of MRI in craniosynostosis has been limited due to its unreliability in identifying the cranial sutures. However, with advantages of radiation-free and excellent soft-tissue contrast, MRI has been an important modality in combination with ultrasonography in infants with suspected associated intracranial anomalies and complications of craniosynostosis. As mentioned above, Eley et al.6) established a novel 3-D MRI technique ("Black Bone") that is able to individually identify the cranial sutures similar to other 2-D imaging modalities. Further research is necessary to standardize the use of 3-D MRI's of the cranium; however, this technique is revolutionary for radiosensitive infants with craniosynostosis.
With advancements in devices and technology, we can presently apply MRI and 0.2 mSv 3-D CT to inspect the cranial bones, sutures and soft tissue of children with craniosynostosis. However, clinical evaluation followed by ultrasonography should be considered the first step for imaging diagnosis in infants with craniosynostosis. MRI should be considered in children with suspected intracranial anomalies and complications. Plain skull radiography satisfies the clinical need in the majority cases involving monosutural craniosynostosis, even for preoperative planning of surgical correction and postoperative follow-up. CT should be reserved for children with complex craniofacial deformities to plan the management of the disease. Presently, available commercial low-dose 3-D CT scanners have an effective radiation dose of approximately 0.2 mSv. In addition, 3-D MRI and ultra-low-dose 3-D CT scanners are expected as an alternative to plain skull radiography in the near future.