INTRODUCTION
It would be mandatory to choosing the optimal treatment regimens in patients with cerebral venous sinus thrombosis (CVST). But this often poses challenging for physician. In patients with acute CVST, the use of dose-adjusted unfractionated or low-molecular weight heparin has been considered an optimal treatment modality. But there is still a controversy as to it because intracranial hemorrhage (ICH) might occur or aggravate in patients with CVST5,6). On the other hand, endovascular therapy (EVT) may be another treatment option in patients whose underlying clinical conditions are more severe or medical refectory. We experienced a case of a 27-year-old man who presented with venous infarction accompanied by petechial hemorrhage secondary to the superior sagittal sinus (SSS) thrombosis. We successfully treated our case with mechanical thrombectomy using the Solitaire FR device (Covidien Neurovascular, Irvine, CA, USA). Here, we report our case with a review of the literature.
CASE REPORT
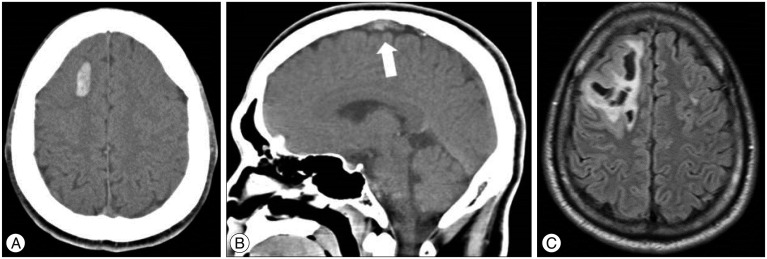
A 27-year-old right-handed man with a smoking history presented with syncope followed by headache. The patient had a 1-year-history of hyperthyroidism and received methimazole. On noncontrast computed tomography (CT) scans, the patient had a small amount of hemorrhage in the right upper frontal area, accompanied by an increased attenuation in the anterior-middle portion of the SSS (Fig. 1A, B). Therefore, the patient was given anti-coagulants and anticonvulsant. Over the next 24 hours, however, the patient exhibited repeated episodes of seizure followed by the left-sided hemiparesis. On follow-up MRI scans, the patient had expansion of hemorrhage with the adjacent edema in the right frontal lobe (Fig. 1C). Despite appropriate medications, the patient had deterioration of clinical presentations due to progressive thrombosis. Therefore, the patient received the EVT.
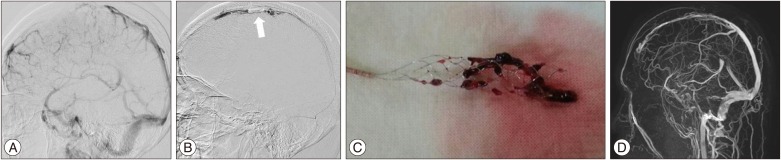
On initial angiography, the patient had a near-complete occlusion of the anterior 2/3 of SSS and cortical veins (Fig. 2A). A 90 cm 8 Fr vista guiding catheter was navigated into the right internal jugular vein. In addition, a 2.7 Fr excelsior microcatheter was navigated and then placed in the anterior portion of the SSS. Then, the Solitaire FR (4√Ч20 mm) was deployed in the anterior portion of the thrombosed SSS, and it was left for ten minutes before the retraction into the sheath. During its retraction, we performed the manual aspiration through the side port of the guiding sheath using a 50 mL syringe. Thus, we removed a small amount of thrombus. But the sinus remained occluded. We attempted the same procedures two more times. But we were not successful in recanalizing the occluded SSS. We therefore performed the mechanical thrombectomy using the same methods using the Solitaire FR (6√Ч20 mm) (Fig. 2B). Thus, we were successful in removing larger clots (Fig. 2C). On angiography, the patient achieved a recanalization of the occluded SSS and did improvement of the arteriovenous transit time, but there were some residual thromboses. Therefore, we injected a 100000 IU of urokinase for thrombolysis. The patient achieved gradual improvement of the neurological symptoms without additional episodes of seizures. At a 2-week and a 3-month follow-up, the patient underwent angiography and MR venography, respectively, thus confirming a good perfusion in the SSS (Fig. 2D). At a 3-month follow-up, the patient showed uneventful course without seizures and cognitive dysfunctions.
DISCUSSION
The CVST is an uncommon entity and its clinical presentations are highly variable. Its favorable prognosis has been well documented. But its mortality is estimated at approximately 5%2). If there is a continuous increase in the intravenous pressure, this would lead to the hemorrhage and cytotoxic edema arising from the capillary or venous rupture and decreased cerebral perfusion8). Once this happens, the fatal herniation rapidly occurs. It would therefore be mandatory to achieve an early recanalization of the occluded SSS in patients who presented with a rapid neurologic deterioration on neuroimaging studies. To date, it has been reported that the systemic anti-coagulation is effective for acute CVST. But the endovascular recanalization is an effective modality for immediate revascularization and the restoration of the sinus perfusion.
There have been several reports about the EVT such as balloon angioplasty12), stenting9), microsnare1), rheolytic thrombectomy and penumbra aspiration system4). According to a review of the literature, however, there are only two cases of cerebral sinus thrombosis that has been treated by stent retriever thrombectomy7,11). Although the concept of stent retriever thrombectomy is like an intraarterial thrombectomy, physician should consider its diameter and radial force. Brockmann et al.3) measured the diameter of the SSS on CT angiography, thus reporting that its mean horizontal diameter was 6.7 and 8.6 mm and its mean vertical one was 5.2 and 6.4 mm at the level of the coronal suture and 3 cm dorsal to the coronal suture, respectively. In the current case, we removed a small amount of the thrombus from the occluded SSS using a 4 mm device and did the main thrombus from the distal region of the coronal suture using a 6 mm one. Additionally, the diagnosis of CVST is commonly overlooked or delayed because there is variability in its signs, modes of onset and neuroimaging characteristics. This would lead to the formation of highly elastic thrombus in the SSS7). It can therefore be inferred that more radial force might be needed for the recanalization. Thus, we may assume that a 6 mm device would be more appropriate for the SSS thrombectomy as compared with a 4 mm because the intensity of the radial force is proportional to the diameter of the SSS, as shown in the current case.
If combined with thrombolytic agents, the Solitaire FR would be more advantageous. According to Li et al.10), 52 patients with CVST were treated using a wire and an angioguard protection device combined with thrombolyic agents. These authors reported that 14% and 6.8% of total patients had a mild increase in the parenchymal hemorrhage and achieved aggravation of the symptoms after receiving a 100-1500√Ч103 IU of urokinase during the mechanical thrombectomy, respectively. Although this percentage is low, it is potentially harmful for patients with pre-existing intracerebral hemorrhage. In the current case, we only used 100√Ч103 IU of urokinase for thrombolysis. This suggests that the mechanical thrombectomy using the Solitaire FR is available, if applicable, when combined with a small amount of urokinase.
CONCLUSION
In conclusion, our case highlights not only that the mechanical thrombectomy using the Solitaire FR may be alternative treatment option for achieving revascularization both rapidly and efficiently available, if applicable, when combined with a small amount of urokinase but also that it might be another option in patients with severe CVST who concurrently had rapid clinical deterioration with devastating consequences.