INTRODUCTION
In current attempts to attain posterior fixation of the middle and lower cervical spine, posterior cervical lateral mass screw fixation has been widely used. For example, cervical instabilities due to trauma, degenerative disease, infection or tumor are indicated for cervical fixation2,8,16,22). Many authors asserted that posterior cervical lateral mass screw fixation provided the same biomechanical stability as compared with anterior cervical fixation or posterior wiring technique6,11,20,25). Furthermore, owing to advances in the polyaxial screw-rod system, cervical fixation surgery may easily and more conveniently be performed7,12,18,19,24). Ever since Roy-Camille first introduced posterior cervical lateral mass screw fixation in 1972, numerous authors developed and modified it. Louis, Magerl, Anderson and An were representative of these authors1,2,16,21,27). According to various anatomical and clinical studies conducted previously, the two most popular techniques have been the Roy-Camille and Magerl techniques. Each of these techniques has an entry point and a trajectory for taking into account any possible injury to a nerve root, vertebral artery and adjacent facet joint1,8,10,22,26). These techniques also consider bicortical purchase imperative for successful bone fusion15). Generally, the Roy-Camille technique is associated with high incidences of a facet joint violation while the Magerl technique seems to have more frequent incidences of a nerve root injury4,14,26).
In addition to these techniques, the Kim's technique was introduced as an alternative method of a posterior cervical lateral mass screw fixation incorporating 2D-CT image and cadaveric study3,5). Viewing it from the lateral side, this modified method allows a screw to be driven into the area, which was 1 mm medial to the center of the lateral mass and in parallel to the center of the spinous process. The lateral angle was determined by the direction to which the screw driver leaned against the tip of the spinous process of the ipsilateral surface3,5).
The purpose of this investigation was 1) to analyze clinically-executed lateral mass screw fixation by the Kim's technique as suggested in the previous morphometric and cadaveric study and 2) to examine various complications and bicortical purchase that are important for bone fusion.
MATERIALS AND METHODS
Study population
Thirty-nine patients who underwent posterior cervical lateral mass screw fixation were investigated at this institute during the period from 2008 through 2010. A total of 178 cases of lateral mass screw operation performed with Kim's technique were analyzed. Through reviewing the operative records, patient charts and radiologic findings including three-dimensional computed tomography as well as plain X-ray images, this study examined nerve root injury, violation of the facet joint, vertebral artery injury and bicortical purchase.
Surgical technique
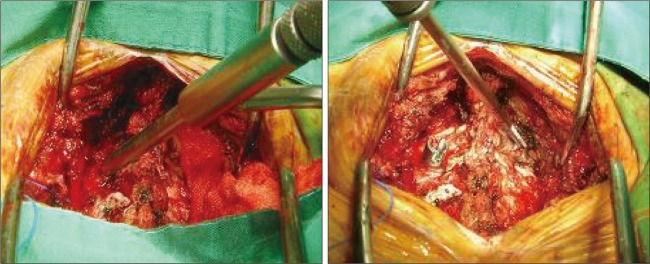
In this procedure, patients were placed in a prone position using a Mayfield skull clamp under anesthesia and the alignment of the cervical spine was verified using a C-arm fluoroscope. A skin incision was made through the midline to expose the outer edge of the lateral mass to the extent of the area of fixation after periosteal dissection. For screw insertion, the junction between the lamina and facet was used as the medial border. The lateral edge of the facet was decided as the lateral border while the cranial facet joint and caudal facet joint were regarded as the superior and inferior border, making it a rectangle. The point of area located 1 mm medial to the center of the rectangle was used as an entry point. The medial border could be verified by identifying the valley of the junction of the lamina and the facet. The lateral border was confirmed by the far edge after having a full exposure of the articular mass. The superior and inferior borders were represented by each facet joint. After determining the entry point in the operative field, the direction of the screw was verified by the spinous process. The drill bit was allowed to lean on the tip of the spinous process in the center of the posterior arch of the cervical spine, in parallel with the spinous process. As mentioned in the previous study5), the lateral angles of the cervical spine from C3 to C7 attained from this method were 29.0, 29.8, 29.5, 26.3 and 23.9, respectively.
The sagittal angle was determined by the angle of each spinous process. The size of the screw (The SKY product of GS Medical and VERTEX product of Medtronic) used was 3.5├Ś14 mm. Before inserting a rod, after completion of the lateral mass screw fixation of the level at which surgery was to be performed, a C-arm fluoroscope was used to verify the overall perspective of the screw and lateral alignment. In case of planning especially decompressive laminectomy, performing laminectomy ahead would leave us with inability to determine the angle using the spinous process. Thus, before performing total laminectomy, the sagittal and lateral angles were verified with respect to the adjacent anatomical structures, and then even tapping was carried out using a tapper. Finally, screw fixation was undertaken in accordance with the prepared trajectory (Fig. 1).
Clinical evaluation
A neurologic examination was carried out on admission. The neurologic examination results obtained before and after surgery were compared. The results of each neurologic examination, clinical course and complications were recorded in the patient chart. Routine follow-up observations were made at three, six and twelve months after surgery. The incidences of hardware complications, such as broken screws or pull-out of screw, and the achievement of successful bone fusion were also recorded along with other previously documented elements.
Radiographic evaluation
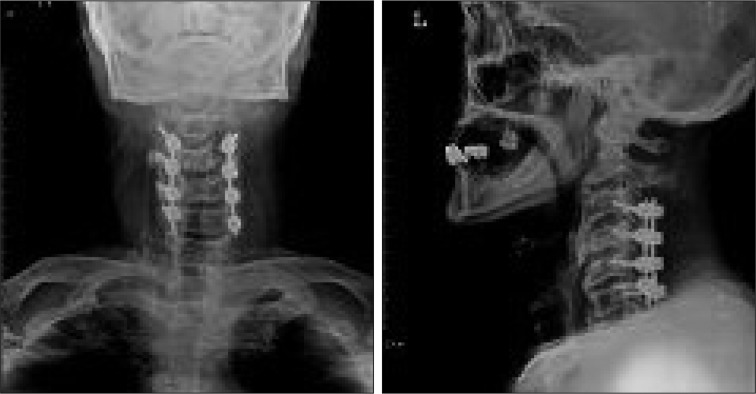
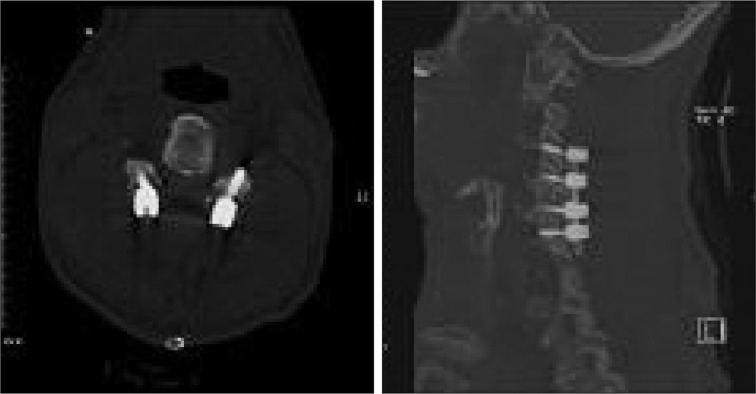
On admission, C-spine X-ray, CT and MRI results were examined. X-ray and CT images were verified after surgery. Surgical outcome, the position and direction of the screw as well as bicortical purchase were confirmed. The state of bone fusion was assessed by evaluating follow-up X-ray or CT results three months after surgery. Of these thirty-nine patients, 31 with trauma reached the goal of spinal fusion. Hence, postsurgical reduction and bone fusion outcome would be important factors in determining the success or failure of the surgery. Injury of the vertebral artery was determined by a transverse foramen involvement of the screw tip in the postsurgical CT images. Facet joint violation was judged by verifying whether or not the screw tip went over the facet joint in the postsurgical CT images. The presence of bicortical purchase was also decided by confirming bicortication of the screw in the postsurgical CT images. In the previous study, on the other hand, any injury to the nerve root by the screw was directly verified by examining the cadaver. However, a nerve root injury was determined by postsurgical clinical symptoms of patients in this investigation. Bone fusion was confirmed upon the presence of a bridging bone or motion limitation in the dynamic view (Fig. 2, 3).
Statistical analysis
SPSS/WIN (Ver. 14.0) was used for all statistical analyses while a p-value of 0.05 or less was considered statistically significant. In describing and summarizing data, the mean with standard deviation and frequency with percentage were used for qualitative data. Chi-square (Žć2) Test was also used for all statistical analyses.
RESULTS
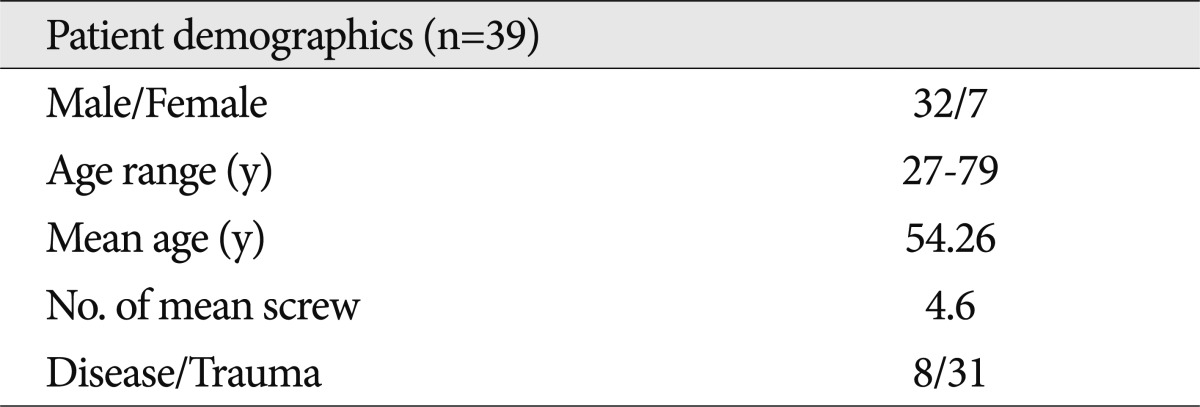
The data from thirty-nine patients who underwent posterior cervical lateral mass screw fixation were analyzed. There were 32 male and 7 female subjects with ages ranging from 27 to 79 years old with the mean age of 54.26 years old. The most frequent indication was spondylosyndesis due to instability following a trauma. A total of 178 screws were analyzed and the mean number of screws for each patient was 4.6. There were 18 screws for the level C3, 37 for C4, 56 for C5, 50 for C6 and 17 for C7. Fixation was performed on the average of 2.71 levels (2 to 5 levels). These data were summarized in Table 1. Screw complications and bicortical purchases for each level were analyzed in Table 2.
In the C3 level, bicortical purchase was evident for 15 out of 18 cases (83.3%). Three out of 18 cases (6.7%) showed a facet joint violation. In the C4 level, 31 out of 37 (83.8%) showed a bicortical purchase. Two out of 37 (5.4%) cases showed a facet joint violation. In the C5 level, 89.3% cases showed a bicortical purchase. Three out of 56 cases (5.4%) revealed a facet joint violation. In the C6 level, 47 out of 50 (94.0%) cases had a bicortical purchase. Six out of 50 (12.0%) cases showed a facet joint violation. In the C7 level, 76.5% cases had a bicortical purchase. Two out of 17 (11.8%) cases showed a facet joint violation. One-hundred fifty-six out of the total of 178 cases (87.6%) showed total bicortical purchase. Sixteen out of 178 cases (9.0%) revealed total facet joint injury.
In the comparisons of Bicortication ratio (p=0.310) and Facet joint injury ratio (p=0.479) among levels ranging from C3 through C7, the results showed no statistically significant difference found for each level. There was neither iatrogenic vertebral artery nor nerve root injury due to screws after lateral mass screw fixation of the posterior cervix had been performed. Bone fusion was achieved in all cases that undertook lateral mass screw fixation of the posterior cervical vertebrae. There were no cases with screws pulled out or broken.
DISCUSSION
After the introduction of lateral mass screw fixation by the Roy-Camille in 1972, various protocols on lateral mass screw positioning were suggested in consideration of nerve root and vertebral artery injury, facet joint violation, successful bone fusion and convenience of screw fixation. Heller et al.14) reported that there were higher rates of nerve root injury in Magerl technique than the Roy-Camille technique. Xu et al.26) introduced a modification of conventional Magerl technique, namely, a technique in which the direction of trajectory was shifted cranially in the area just below the articular surface, and by doing so, the entrance point was somewhat raised from that of previous one in the area 2 mm below the inferior edge of the superior facet in order to avoid nerve root injury. Barry et al.4) asserted that the screw would be driven into the direction of the midway between the nerve bundles and it would lead to a low incidence of a nerve root injury in the Roy-Camille technique. However, the Roy-Camille technique would have a higher frequency of facet joint violation as opposed to that of the Magerl technique.
Ebraheim et al.10) reported from their anatomical study that 15 degree lateral angulation would avoid injury of the vertebral artery in both the Roy-Camille and Magerl techniques. However, Cho and Kim5) reported that there were no differences in safety angle to avoid injury to the vertebral artery among the Roy-Camille, Magerl and Kim's techniques.
Heller et al.15) described that bicortical purchase had about thirty percent (30%) more pullout resistance as compared to unicortical purchase did. A long screw would increase the risk of nerve root injury, and an optimal screw length should be decided to attain successful screw fixation. Our senior author (KDH) once suggested a modified lateral mass screw technique that determined a screw trajectory using adjacent anatomical structures. Cho and Kim5) focused on Koreans assuming that the lateral mass of East Asians and Koreans would be smaller than that of Europeans or Hispanics. The mean screw length used for the Roy-Camille technique in the vertebrae ranging from C3 through C6 was 13.5 mm. The mean screw length used for the Magerl technique was 14 mm for the vertebra ranging from C3 to C6 while it was 13.6 mm for C7. This was the result that concurred with that of Yoon et al.28) study. In the meantime, it was reported that the minimal depth for bicortical screw fixation for the vertebrae ranging from C3 to C6 using the Kim's technique was 13.8 mm for C3, 13.9 mm for C4, 13.7 mm for C5 and 13.5 mm for C65). Thus, a 14 mm screw was used for optimization in order to reduce complications and gain bicortical purchase in this study.
According to Cho and Kim5), the length of screws needed for bicortical purchase of the lateral mass at C7 was 13.3 mm. In this study, however, bicortical purchase was achieved in 76.5% of lateral mass screw fixation at C7. This was slightly lower than other levels. Thorough reviews revealed that the lateral mass screw wasn't tightened enough in the C7 level for several cases. In these cases as described in Fig. 4, the head of screw was in contact with the lamina on the medial aspect even if the screw had not yet been advanced into the lateral mass for few threads. Screw tightening might be hindered because the angle between the spinous process to the lamina and the lateral mass was too steep in the C7 level due to the longer and larger size of the spinous process. Thus, a screw must be tightened a few threads more in the C7 level when the screw head is in contact with the cortical bone of the lamina on the medial aspect to ensure bicortical purchase at this level.
C7 is a transitional vertebra with a very thin lateral mass and the C7 spinal nerve is located closer to the anterior aspect of the lateral mass. Further precaution is required since there are higher possibilities of a nerve root injury with a long screw. In the C7 level, pedicle screw fixation that provides optimal stabilization is performed in large numbers29). However, owing to a higher risk of neurovascular structure injury with pedicle screw fixation as opposed to lateral mass screw fixation, it is difficult to choose either one as a better technique. Lateral mass screw fixation was chosen in this study.
Heller et al.14) recommend using a fluoroscope for guiding screw fixation during surgery. Confirmation of the location and direction of the screw by using a C-arm fluoroscope plays an important role in raising surgical accuracy. However, exposure to radiation during surgery is associated with radiation-related complications13,17). Thus, other surgeons such as Roche et al.23) introduced the modified An's method for performing lateral mass screw fixation without the help of a fluoroscope. The entrance point was 1 mm medial to the center of the lateral mass, and the screw was fixed at 33┬░ laterally and 17┬░ cranially. They described that the lateral mass screw had been fixed safely without complications using this technique9,23).
Although the Roy-Camille, Magerl and An methods are known to be used relatively safely, determination of lateral and sagittal angles during surgery may be somewhat unclear. For instance, there were mentions of 10┬░, 25┬░, and 30┬░ for lateral angles, but it would be difficult to make accurate measurements of these angles in reality. The same might be said with sagittal angles. Experienced surgeons could easily decide on lateral and sagittal angles empirically. However, beginners might not be familiar with it in particular and could be dependent on imaging devices such as a C-arm fluoroscope. Naturally, before undertaking such surgery, surgeons should consider sufficient training and such techniques.
This study commenced with these aspects in mind. There are similarities to the approach suggested by An et al., but the Kim's technique has several advantages. In the Kim's technique, the lateral angle is decided by having a screw driver leaning against the ipsilateral surface of the spinous process while the sagittal angle is determined by having it in parallel with the center of the spinous process in surgical view. Furthermore, these authors believe that this approach may not only reduce the usage of a C-arm fluoroscope reducing radiation exposure, but also shorten the operation time. In this study, incidences of injuries to nerve root or vertebral artery, facet joint violation and bicortical screw fixation were quantitatively analyzed and compared at each level.
In the Roy Camille Technique, Heller et al.14) reported that nerve root injury was 0.8% and the facet joint violation was 22.5% in their cadaveric study. In the Magerl technique, the rate of nerve root injury was 7.3% and facet joint violation was 2.4%. Baek et al.3) investigated bicortical purchases of three different cervical lateral mass screw fixation techniques of Magerl's, Roy-Camille's and Kim's with a cadaveric study. They reported that the rate of bicortical purchase of the Roy-Camille technique was 83.3% while that of the Magerl technique was 55.6%. In this study, there was no nerve root injury, while facet joint violation and bicortical purchase for each level was 9.0% and 87.6% respectively (Table 3). Therefore, considering these study outcomes, the Kim's technique might be an alternative choice of method for cervical lateral mass screw fixation. In comparisons of these techniques for each level from C3 to C7, there were no statistical differences in complication rate and bicortical purchase rate.
Considering pros and cons of the Roy-Camille and Magerl techniques, the Kim's technique has an advantage over the other techniques in the aspect that it may be performed at any cervical level with good results. It is regrettable that biomechanical evaluations were not performed and comparisons of these three techniques discussed had not been quite objective in this study.
CONCLUSION
The approach of posterior cervical lateral mass screw fixation has been transformed and progressed by many surgeons. In this study, the Kim's technique was found to be as good as any other known technique through analyses of complication rate and bicortical purchase, in comparisons with the results from other published cadaveric and clinical studies. Determination of screw angles by using adjacent anatomical structures, in an operational view, may provide, especially, junior spine surgeons with an advantage of easier and safer performance during lateral mass screw fixation procedure. The consideration is that the Kim's technique is an alternative choice that may be performed easily and safely in the treatment of many cervical diseases.