The Psychopathological Influence of Adolescent Idiopathic Scoliosis in Korean Male : An Analysis of Multiphasic Personal Inventory Test Results
Article information
Abstract
Objective
There are few published studies which have documented psychopathological abnormalities in patients with of adolescent idiopathic scoliosis (AIS) The aim of this study was to evaluate the psychopathological influence of AIS in Korean 19-year-old males.
Methods
The authors compared the Korean military multiphasic personal inventory (KMPI) military profiles of 105 AIS cases (more than 10 degrees of Cobb's angle without surgical treatment) with the KMPI profiles of 108 normal controls. The AIS group was split depending on Cobb's angle to further evaluate this relation by the severity of AIS.
Results
A significantly decreased result on the faking-good response scale and an significantly increased result on the faking-bad response were observed in the AIS group compared to the control (p<0.012). The neurosis scale results, including anxiety, depression and somatization symptoms, were significantly increased in the AIS group compared to the control (p<0.010). The severity level of personality disorder and schizophrenia were also significantly increased in the AIS group (p<0.010). Differences in KMPI scale scores were not related to the severity of AIS.
Conclusion
Young males with AIS tend to have abnormal results on the multiphasic personal inventory test compared to normal volunteers, suggesting that AIS may be related to psychopathology in the young male group in Korea. Although these psychopathology in AIS were differently observed compared to normal controls, but not interfered with military life. Clinicians are recommended to pay attention the psychopathological traits of patients with AIS.
INTRODUCTION
Patients with idiopathic scoliosis are nervous about the deformed trunk of the patient on a regular basis, and experience strong anxiety that the patient may lead their life with a deformed trunk in the future1,2,8,18). The multiphasic personal inventory test is widely used to investigate personality structure and psychopathology in various disciplines, but it is not commonly used in the field of spinal deformity disease. Additionally, there are few published studies which have documented psychopathological abnormalities in patients with adolescent idiopathic scoliosis (AIS). This study, therefore, using tests results from the Korean conscription system, reviews multiphasic personal inventory test scores to examine the psychological influence of AIS in Korean male adolescents.
MATERIALS AND METHODS
Korea has a conscription system, meaning that all males are examined for conscription by the Military Manpower Administration. In the course of this examination, examinees are administered the Korean military multiphasic personality inventory test (KMPI) from April to November 2011. By using these results, we collected the data of normal healthy volunteers and examinees with AIS. All examinees in this study were 19-year-old males tested at the Seoul regional Military Manpower Administration.
The normal group subjects (n=108) were interviewed by one physician and had no medical history, including that of spinal conditions, and no history of psychological problems. The examinees with AIS (105 cases) had their condition confirmed by thoraco-lumbar standing radiographs (TLSR) during the conscription process. The Cobb angle was the crossed angle on the perpendicular line from each end vertebrae that are the vertebrae at the upper and lower limits of the curve which tilted most severely toward the concavity of the curve4,5). We considered normal spinal curvature to be a Cobb angle of less than 10 degrees. Cobb angles in TLSR were recorded by a radiologist, an orthopedic surgeon and a neurosurgeon separated from each other. If the checked Cobb angle was differently checked by different physician, the Cobb angle was rechecked, and the median angle was selected in the situation of inter-observer variability. In this study, to examine psychopathological effects by the severity of AIS, cases with AIS was categorized by Cobb's angle according to the guideline issued by the Korean military directorate; 1) mild group with more than 10 degrees and lesser than 25 degrees of Cobb angle, 2) moderate group with more than 25 degrees and lesser than 40 degrees of Cobb angle, and 3) severe group with more than 40 degrees of Cobb angle using TLSR. In Korea conscription, cases with normal to mild scoliosis were judged as military service, cases with moderate scoliosis were decided as public service workers, and severe AIS cases were exempted from military service. Each AIS groups were compared in terms of KMPI results.
The KMPI is a conventional type of the Minnesota multiphasic personality inventory test (MMPI) adjusted for Korean conscription16). The KMPI was created in five stages. First, several military-associated questions were added to the pre-existing MMPI. A pre-test (575 questions) was administered to normal soldiers, normal university students, military prisoners, military hospital psychiatric patients and private hospital psychiatric patients. After this, three scales (validity scale, clinical scale and content scale) were established and divided by several profiles, similar to the MMPI. For the final examination, score standardization and a yield of distinct function were performed. The KMPI is similar to the MMPI in its overall aspects16). The KMPI also sets scores for each scale, which are transformed into a standardized T-score. Therefore, by comparing the T-scores of each group, we can easily measure trends in personality and psychopathology.
Several item groups are analyzed by the KMPI, such as the Response Set, Neurosis Set, Psycopathy Set, Accident Set, Prediction Set of accidents, and the Special Set. If results on any one of these scales exceeded the normal rage, this data was automatically categorized as an abnormal result. In this study, the results were divided into three types; Response Set (faking-good response, faking-bad response, and infrequency scale), the Neurosis Set (anxiety, depression, and somatization), and the Psychopathy Set (schizophrenia, personality disorder, and paranoia). Evaluation of the statistical significance of differences was carried out using student t-tests. Tests were considered significant at p-values of less than 0.05. Statistical comparisons were analyzed using SPSS 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
In this study, all 213 examinees were 19-year-old males who lived in Seoul. In both groups, examinees with psychological problems (depression, anxiety disorder, schizophrenia, etc.) were excluded. Table 1 shows the types of AIS participants had according to the severity of Cobb angle in this study. Mild group (more than 10 degrees and lesser than 25 degrees of Cobb angle) was 49 cases, moderate group (more than 25 degrees and lesser than 40 degrees of Cobb angle) was 50 cases, and severe group (more than 40 degrees of Cobb angle) was 6 cases. The severe cases were so few, so we conducted the AIS group categorize to mild group and moderate to severe group. The operated cases were 2, and these cases were not included in the KMPI profiles to avoid the interference of scoliosis surgical correction.
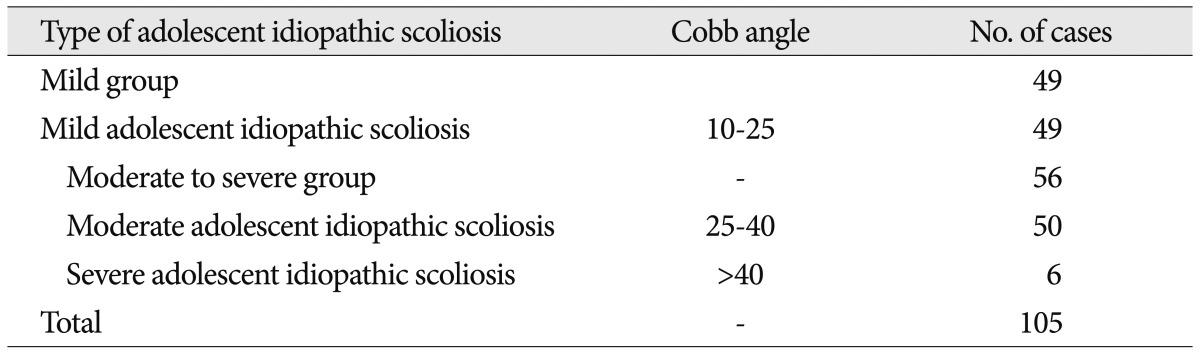
Types of adolescent idiopathic scoliosis according to the severity of Cobb angle
Table 2, Fig. 1 and 2 summarize the KMPI results for the normal group and the AIS group. The proportion of abnormal results, the Response Set, the Neurosis Set, and the Psychopathy Set of KMPI were compared between the two groups. There were significantly differently increased abnormal results in the AIS group (22.9%) than in the normal group (9.3%, p=0.007)(Fig. 1). In the KMPI results, the faking-good and bad response scale, the Neurosis Set (anxiety, depression, and somatization scale), and the Psychopathy Set (schizophrenia and personality disorder scale) were all significantly different between the two groups. The faking-good response scale showed significantly decreased results in the AIS group compared to the normal volunteer group (p=0.012). The faking-bad response was, by contrast, significantly increased in the AIS group (p=0.011). The infrequency scale was not differed by group (p=0.280). In the Neurosis Set, all the scales of anxiety, depression, and somatization were significantly increased in the AIS group (p=0.010, 0.003 and 0.002, respectively). In the Psychopathy Set, the schizophrenia and personality disorder scales showed a significantly increase in the AIS group (p=0.010 and 0.001), with no other differences present.
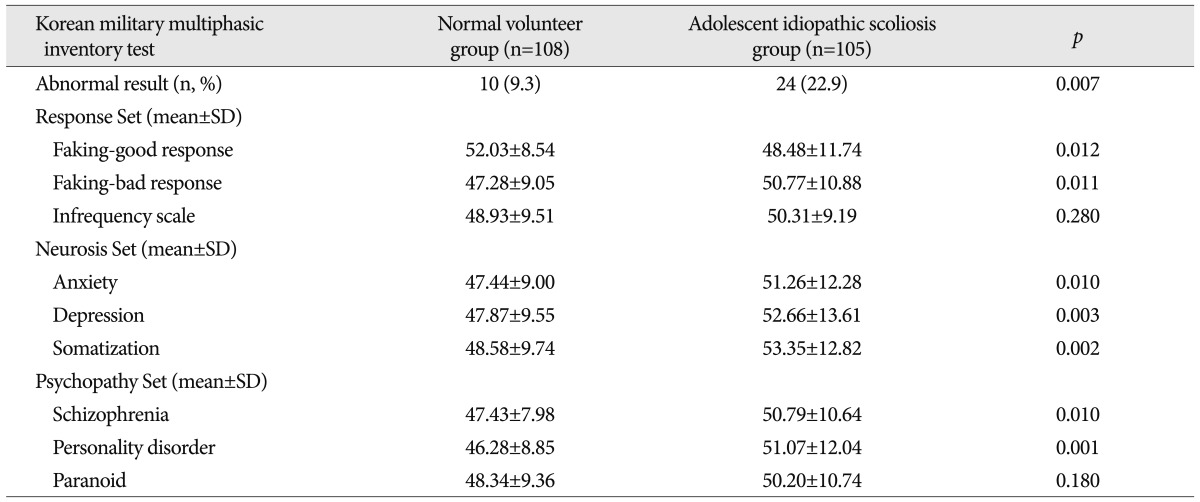
Korean military multiphasic inventory test results in the normal volunteer group and the adolescent idiopathic scoliosis group

Abnormal result percentages of Korean military multiphasic personality inventory test in the normal curves and adolescent idiopathic scoliosis (AIS) according to the severity of Cobb angle. *Statistically significant different.
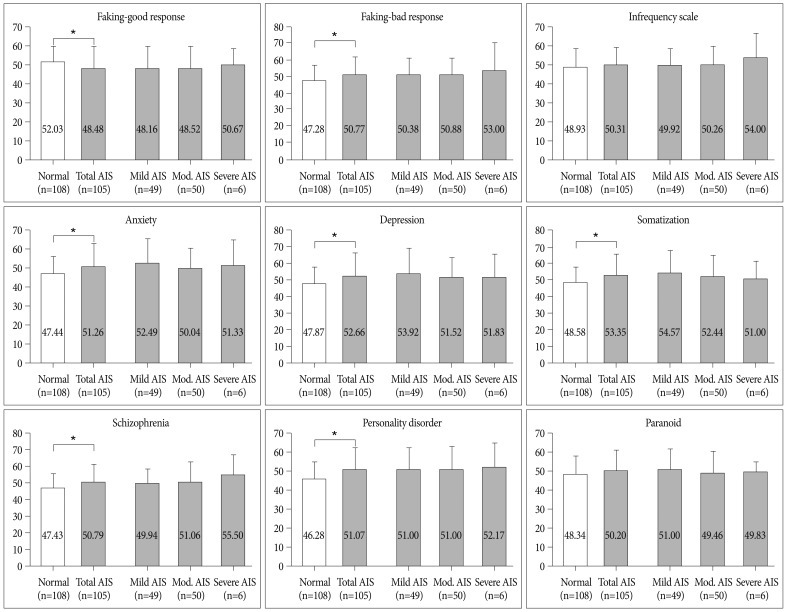
Diagrams of Korean military multiphasic personality inventory test results in the normal curves and adolescent idiopathic scoliosis (AIS) according to the severity of Cobb angle. *Statistically significant different.
We separated AIS subjects by the severity of Cobb angle. Mild group and moderate to severe group cases were 49 and 56 cases. Fig. 2 and Table 3 show the KMPI results by these two subgroups. There were no differences between groups in all KMPI profiles.
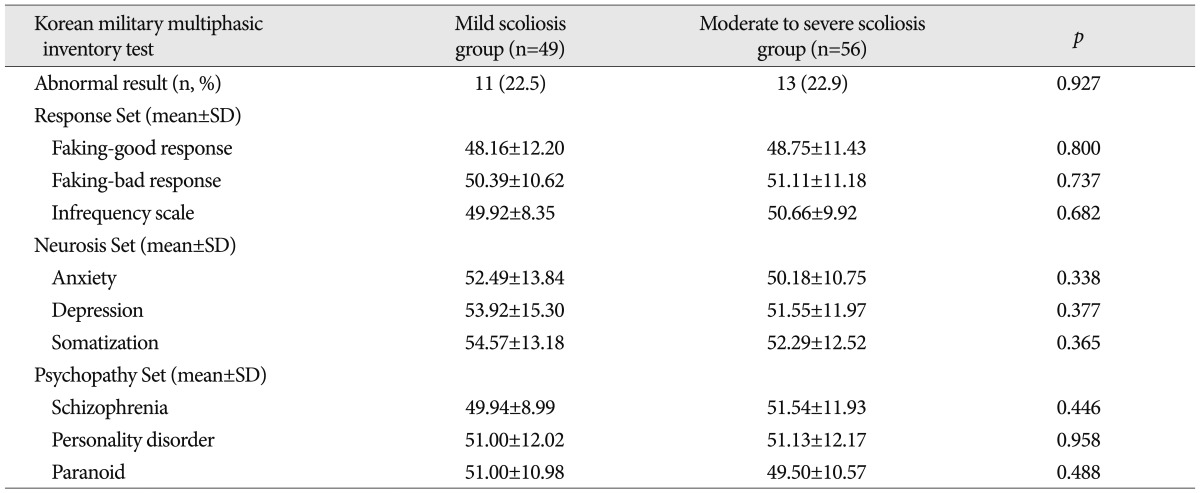
KMPI results in the adolescent idiopathic scoliosis according to the severity of Cobb angle
DISCUSSION
The multiphasic personality inventory is designed to assist in identifying personality structures and psychopathology22). The MMPI is one of the most frequently used personality tests in the mental health field19,21). It also has wider applicability and use; for example, it is used in law to identify malingering claims. However, this test is not commonly applied in the field of spinal deformity disease, and there are a few published studies about psychopathological abnormality in patients with AIS. Because the spinal deformity disease is a main concern of neurosurgical field, meticulous care about its psychopathological influence is required by neurosurgeons.
In the MMPI, there are ten types of clinical scales : hypochondriasis (concern with bodily symptoms); depression (depressive symptoms); hysteria (fixation on problems and vulnerabilities); psychopathic deviate (conflict, struggle, anger, respect for society's rules); masculinity/femininity (stereotypical masculine or feminine interests/behavior); paranoia (level of trust, suspiciousness, sensitivity); psychasthenia (worry, anxiety, tension, doubts, obsessiveness); schizophrenia (odd thinking and social alienation); hypomania (level of excitability), and social introversion (people orientation)17). MMPI analysis focuses on the relative elevation of profiles, with these being compared to profiles of various normal groups. Raw scores are transformed into standardized metric scores, T-scores, in order to facilitate clinical interpretation.
In this study, the KMPI was applied, which is an adjusted form of the MMPI. In this study, only three sets of the KMPI were used. Of these, the Response Set comprised faking-good response, faking-bad response, and infrequent response scale. People fake good responses (faking-good response) when they feel it will serve their interests to skew their answers so as to put them in what they perceive to be a good light. The opposite of this is faking-bad. The infrequent response scale detects infrequent responding among psychopathological populations. Second, the Neurosis Set comprises anxiety, depression, and somatization scales, presenting the respondent's tendency toward these neurotic statuses. Third, the Psychopathy Set comprises schizophrenia, personality disorder, and paranoia subscales, which also capture tendencies toward these conditions.
As shown in Fig. 1 and Table 2, young males with AIS tended to have more abnormal results on the multiphasic personal inventory test compared to normal volunteers. Decreased results on the faking-good response scale and increased results on the faking-bad response scale were observed in the AIS group, compared with the normal group. The Neurosis Set responses were also markedly increased in the AIS group. The schizophrenia and personality disorder scores were also elevated in the AIS group. Therefore it can be suggested that AIS conditions have a significant effect on the psychological state of adolescents.
In previous literature, the multiphasic personal inventory test in the AIS was not usually used. Maudsley personality test10-13), Erich Mittenecker and Walter Toman personality test14), Psychological General Well-being Index5,7), Short Form-364,5), Oswestry Disability Back Pain Questionnaire5,7), Scoliosis Research Society Patient Questionaire3,4), and Frankfurt Self-concept Scales20) were used to prevent patients stopping brace use or to assess the quality of life in AIS. Most of these studies indicated that AIS subjects had poorer psychological and quality of life outcomes than normal controls, which is similar to this study's results. Kasai et al.11) reported patients with scoliosis have frequently a slight introversion and mild neurotic tendency. Misterska et al.14) reported that patients with scoliosis self report having more self-criticism expression than their healthy peers. Noonan et al.15) also concluded that transient psychological effects are often present during treatement of scoliosis. Another study by Matsunaga et al.13) concluded that the measuring personality type is useful to reduce the psychological effect by offering conseling or permitting part-time brace wearing.
However, some reports that do not support those hypotheses and have reported lower levels of psychological distress, or no difference in AIS groups compared with controls. A study by Danielsson et al.5) about the quality of life of patients with AIS indicated little effect on the psychological and social aspects of quality of life. Imanzadeh et al.9) also concluded there was no significant relationship between evidence of scoliosis, depression and anxiety in athletic and non athlete subjects. These studies found some evidence that AIS subjects may even have psychological and quality of life outcomes that are similar with those for normal populations.
Although there are conflicting opinions about the psychological influence of AIS, it is nevertheless important to provide psychological support to AIS children and psychological advice to parents. This is because the common denominators for poor physical and psychological quality of life in patients with AIS were primarily personality traits, psychological distress levels and family support.
Because the personal inventory test results were significantly different between the AIS and normal volunteer groups in this study, it was hypothesized that the severity of AIS could be a trigger of abnormal personality or psychopathology. However, these scales were not correlated with the severity of AIS (Table 3). No previous studies have considered the psychopathological influence of the severity of AIS, so further research is needed to assess this issue.
This study has some limitations. First of all, the KMPI has not been widely documented or analyzed in the literature because its purpose was designed in the unique context of military conscription6). However, the KMPI is officially approved by the Korean government, as with the MMPI16). Secondly, only males were included in this study because the data was sourced from the military conscription examinations. Indeed, this result only showed the tendency of psychopatholgical influence of AIS, and it is not indicate for changing the criteria of conscription although the data was derived from the conscription. Although abnormal results were more increased in AIS, nobody met the criteria of psychopatholgical ground for exemption. Despite these limitations, however, the multiphasic personal inventory test may remain a useful tool for identifying personality changes or psychopathologies in AIS patients.
CONCLUSION
Young males with AIS may be more likely to display abnormal results on the multiphasic personal inventory test compared with normal volunteers, particularly in the scales for faking-good response, faking-bad response, anxiety, depression, somatization, schizophrenia and personality disorder, irrespective of the severity of Cobb's angle. This result suggests that AIS may influence psychopathology in the young male group in Korea, although it was not interfered with military life. Therefore, clinicians are recommended to pay attention the psychopathological aspects of patients with AIS.
Acknowledgements
This work was supported by an Inha University Research Grant.