Emerging Surgical Strategies of Intractable Frontal Lobe Epilepsy with Cortical Dysplasia in Terms of Extent of Resection
Article information
Abstract
Objective
Cortical dysplasia (CD) is one of the common causes of epilepsy surgery. However, surgical outcome still remains poor, especially with frontal lobe epilepsy (FLE), despite the advancement of neuroimaging techniques and expansion of surgical indications. The aim of this study was to focus on surgical strategies in terms of extent of resection to improve surgical outcome in the cases of FLE with CD.
Methods
A total of 11 patients of FLE were selected among 67 patients who were proven pathologically as CD, out of a total of 726 epilepsy surgery series since 1992. This study categorized surgical groups into three according to the extent of resection : 1) focal corticectomy, 2) regional corticectomy, and 3) partial functional lobectomy, based on the preoperative evaluation, in particular, ictal scalp EEG onset and/or intracranial recordings, and the lesions in high-resolution MRI. Surgical outcome was assessed following Engel's classification system.
Results
Focal corticectomy was performed in 5 patients and regional corticectomy in another set of 5 patients. Only 1 patient underwent partial functional lobectomy. Types I and II CD were detected with the same frequency (45.45% each) and postoperative outcome was fully satisfactory (91%).
Conclusion
The strategy of epilepsy surgery is to focus on the different characteristics of each individual, considering the extent of real resection, which is based on the focal ictal onset consistent with neuroimaging, especially in the practical point of view of neurosurgery.
INTRODUCTION
Regarding cortical dysplasia (CD), special interests were initiated by Dr. Andre Palmini's study in 1991, issued at the Sixth International Bethel-Cleveland Clinic Epilepsy Symposium in Bielefeld, Germany, last 1995 in line with the topic of "Pediatric Epilepsy Surgery". Furthermore, with the development of new structural and functional neuroimaging techniques, opportunities and indications for surgical intervention of CD are rapidly expanding. Therefore, CD became the most frequent (33%) etiology of pediatric epilepsy surgery according to the 2004 outcome survey of the International League Against Epilepsy (ILAE) and the third major substrate (13%) in adult epilepsy surgery patients4,18,20). However, surgery for frontal lobe epilepsy (FLE) has also been reported to be associated with a high failure rate because of difficulties in localizing the epileptic zone and the presence of eloquent areas. In addition, many articles that relate malformations of cortical development (MCD) were already published usually regarding clinical and pathological characteristics, as well as surgical outcomes, but few regarding the practical aspect of the extent of resection3,8,13,19,33).
For this reason, this study focused on surgical strategies in terms of the extent of resection to improve surgical outcome to meet the individual cases of FLE with CD.
MATERIALS AND METHODS
According to medical records, 11 patients of FLE were selected among 67 patients (temporal : 48, frontal : 11, parietal : 5, occipital : 3) who were proven pathologically as CD, out of a total of 726 epilepsy surgery series for 22 years since 1992. Patients who had a short follow-up period after surgery (less than 1 year) were excluded to deduce appropriate outcome.
This study's protocols for preoperative evaluation included the patient's neurological and neuropsychological examination, neuroimaging to identify a substrate-related lesion, and noninvasive 24 hour video-electroencephalography (EEG) according to the international 10-20 system.
Magnetic resonance imaging (MRI) was performed for all the patients for detecting structural abnormalities. All patients were classified according to the image findings on the MRI. A definitive group was categorized based on common MRI findings of CD2,6,8), which were approved by more than two interpreters, neurosurgeons, or neuroradiologists. A suspicious group was categorized by disagreement of interpreters because of the subtle signal intensity on fluid attenuation inversion recovery (FLAIR) images. A negative group was categorized as no specific lesion on brain MRI with consent. In addition, fluorodeoxyglucose-positron emission tomography (FDG-PET), single photon emission on computerized tomography (SPECT), and functional MRI (fMRI) were done to help decide the surgical target. Invasive intracranial monitoring with subdural grid, strip, or depth electrodes were also performed in selected cases with an EEG monitoring unit (EMU) for the purpose of the determination of the extent of resection. Intraoperative electrocorticography (ECoG) was also done for most patients. Somatosensory evoked potentials or awake surgical techniques were used case by case.
This study categorized surgical strategies into three groups according to the extent of resection based on the preoperative semiology, MRI, and EEG findings (Table 1, Fig. 1). The first one is the focal corticectomy group (lesionectomy), which was categorized by definitive focal ictal onset on scalp EEG or intracranial recordings and/or visible lesion on MRI consistent with EEG findings. The second is the regional corticectomy group (additional corticectomy), which was classified as regional ictal EEG onset independently with MRI lesion. The third and final group is the partial functional lobectomy group, which was categorized by diffuse lesion in which it is hard to define the extent of resection with difficulty in covering suspicious area by intracranial monitoring or making appropriate craniotomy site for an operative approach, such as a frontal pole or basal frontal area. Other surgical techniques, such as multiple subpial transection (MST), were additionally used in selected patients. Awake surgery or functional mapping was also performed when lesion was proximal to the functionally eloquent cortex.
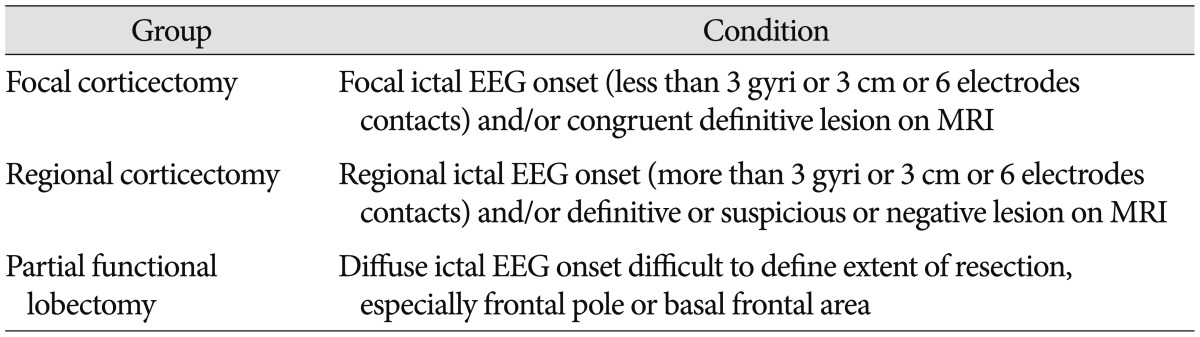
Three categories of the extent of resection based on surgical strategies
After surgery, all patients were maintained on the same antiepileptic drug regimens as before surgery and the medicine was tapered according to the patient's condition. They were observed for at least one year and surgical outcome was assessed following Engel's classification system11).
RESULTS
General characteristics
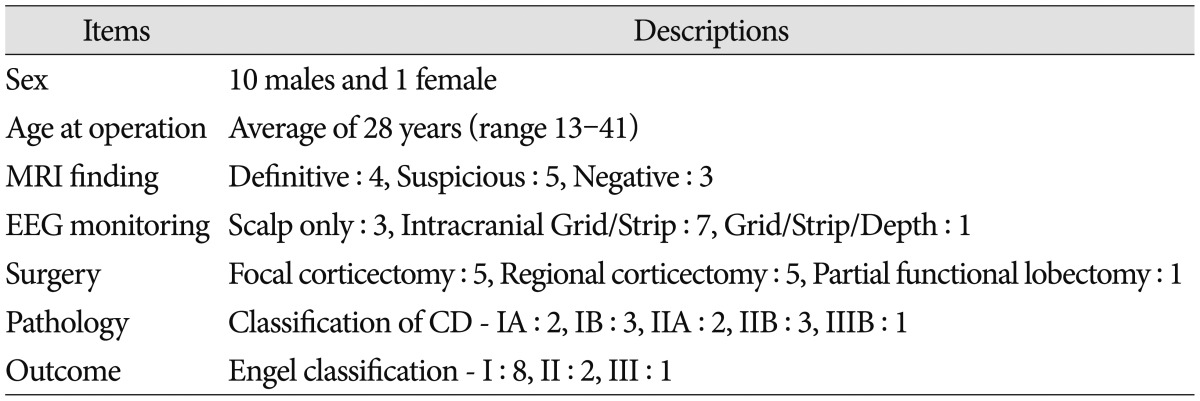
A total of 11 patients with FLE (16% of CD) were selected for this topic and they underwent surgical management between March 1995 and June 2013. There were 10 males and 1 female, with an average age of 28 years (range 13-41 years). General characteristics are described in Table 2, 3.
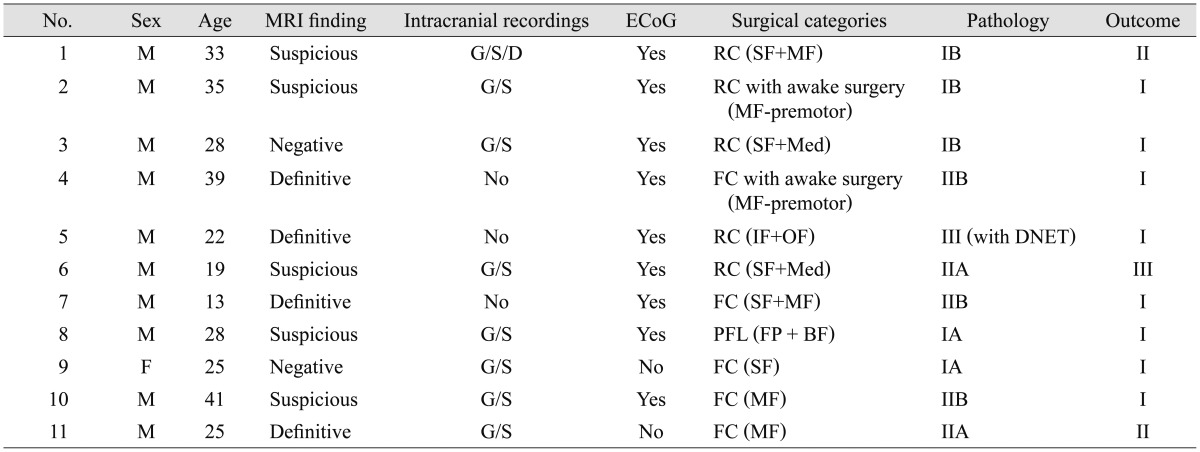
Characteristics of patients who had frontal lobe epilepsy with cortical dysplasia
Summary of 11 patients who had cortical dysplasia with frontal lobe epilepsy
MRI findings and surgical resection
MRI demonstrated definitive findings of cortical dysplasia in 4 patients (36%). In addition, 5 patients (45%) revealed a suspicious lesion, 1 patient with a subtle high signal intensity on the left superior frontal gyrus, and 4 patients with diffuse cortical atrophy or thickening on the frontal lobe. Two patients (19%) were included in the negative MR finding group.
A total of 8 patients (73%) needed preoperative evaluation with invasive intracranial monitoring like grid, strip, or depth electrodes (Fig. 2). Among them, 6 patients additionally underwent intraoperative ECoG to find the epileptic zone, whereas the other 2 patients had a single-stage operation with the help of only grid/strip. There were 3 patients (27%) in which only ECoG was used to remove the lesion because of the positive detection of focal ictal onset on scalp EEG accordant with MRI lesion (Fig. 3).
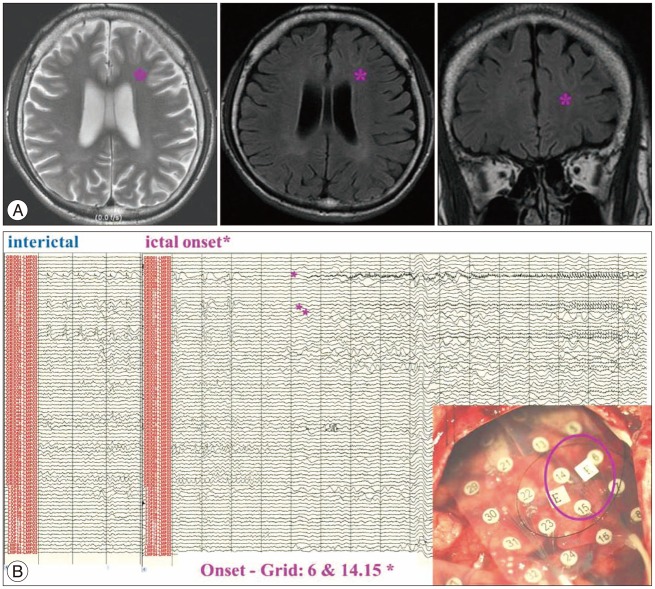
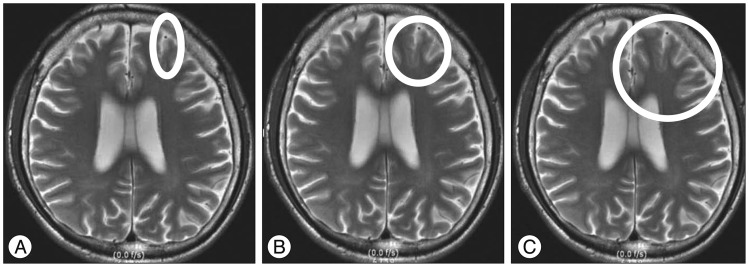
Illustration of case 10 with focal corticectomy with intracranial recordings. Patient is a 41-year-old male; 15-year history of complex partial seizures characterized by hypermotor seizure with right arm tonic posture and loud vocalization. The video-EEG evaluation revealed no definitive ictal onset. Brain MR showed subtle high signal change on the left middle frontal gyrus (A : stared). Invasive intracranial monitoring (Grid) demonstrates rhythmic alpha activity over left centroparietal area intermingled with muscle artifacts during ictal period and very frequent small spikes on the left frontal area (Fp1, F3) during interictal period (B). The extent of corticectomy was planned based on the ictal onset of intracranial recordings (C : pink circle of areas 6, 14, 15 on Grid). Patient belongs to Engel class I with a follow-up of 1 year.
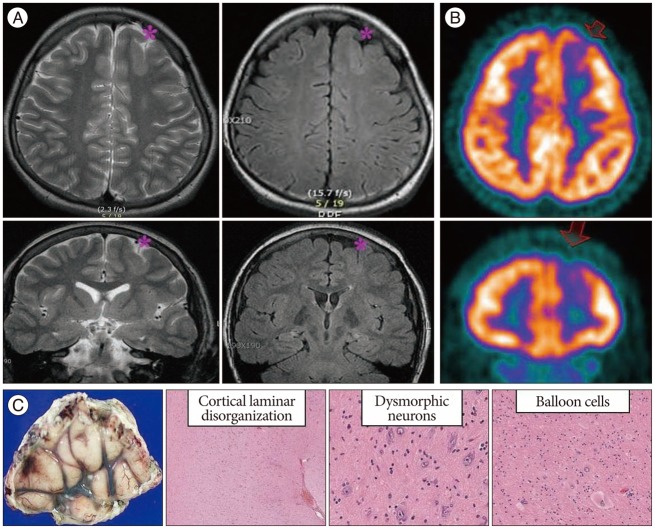
Illustration of case 7 with focal corticectomy without intracranial recordings. Patient is a 13-year-old male; seizure onset at 4 years of age was characterized by nocturnal seizure attack with head rotation to right and dystonia of right arm. Video EEG demonstrates left frontal ictal and interictal EEG discharges consistent with his semiology. MRI shows abnormal focal thickening of the cortex in the left superior frontal gyrus (A : stared). PET scan revealed focal hypometabolism at left frontal cortical area consistent with MR findings (B : arrows). Focal corticectomy was performed on left superior frontal gyrus under ECoG guide without intracranial recordings. Postexcisional ECoG reveales no residual spikes, and pathology revealed cortical dysplasia type IIb (C). Two years after surgery, he belongs to Engel class I.
Regarding to surgery, 5 patients (45.45%) were included in the focal corticectomy group. The extent of resection was determined by definitive lesion on MRI combined with the regions of focal ictal EEG onset. Although one patient had a negative MR finding, he showed focal ictal onset on scalp EEG consistent with grid monitoring.
Another set of 5 patients (45.45%) underwent regional corticectomy (lesionectomy and additional corticectomy). In this group, one 22-year-old male patient received tumor removal and adjacent corticectomy on the right inferior frontal gyrus and orbitofrontal area, as well as an additional procedure called MST to block the propagation of epileptic discharge and to minimize neurologic functional loss from language cortex injury. He was diagnosed with dysembryoplastic neuroepithelial tumor (DNET) and CD. CD was found on the cerebral cortex of peritumoral area.
Only one patient (9.1%) received partial functional lobectomy. His epileptic focus was presumed to be on the right middle frontal pole and basal frontal area. In this case, the study intended to reduce seizure frequency by disconnecting white matter of epileptic discharge. He fortunately had no seizure attack after surgery with concurrent medication (Engel classification I).
Pathology
All patients were pathologically diagnosed with CD. Their diagnoses were revised by the new ILAE classification system of CD in 20115,23). A total of 5 patients (45.45%) were confirmed to be type I (2 patients for IA, 3 patients for IB) and 5 patients (45.45%) to be type II (2 patients for IIA, 3 patients for IIB); 1 patient (9.1%) was classified to be type IIIB because of associated DNET.
Outcome
They were observed for at least 1 year after surgery. A total of 8 patients (72.7%) were seizure-free or only experienced auras during the period (Engel's classification I); 2 patients (18.2%) revealed only nocturnal seizures with significant improvement of daily life quality (Engel's classification II); and only 1 patient (9.1%) was included in class III. To conclude, this study presented much better outcomes (91%) than other studies (60-85% of good surgical outcome : combination of Engel's classifications I and II)20,22,25,32,35). Comparing with only Engel class I, this study's patients revealed superior results (72.7%) to those (45.1%) of previous studies12,16).
DISCUSSION
If a patient with intractable epilepsy who has evidence of underlying structural pathology confirmed with high-resolution MRI, the patient can be a surgical candidate. The association of the well-circumscribed lesion and good postoperative outcome has been demonstrated in many studies9,27,28,34) because of the uncomplicated decision-making regarding surgical extent and approach. A total of 4 patients with definitive lesion in this study's series buttressed these results through excellent postoperative outcomes (Engel's class I for 3 patients, II for 1 patient). With regard to pathology, Kabat and Król.23) presented that the specific MRI feature for CD was more evident in type II than type I. They also mentioned that FCD type II is more often found in extratemporal locations with predilection toward the frontal lobe23). Although the same frequency was detected for types I and II, a definitive MR lesion was more common for type II than type I FCD in this study's series. Kuzniecky26) reported a correlation between the presence of hyperintense areas on T2-weighted images and balloon cells, which can be found in type IIB FCD8).
For patients with negative lesion on MRI, EEG findings (on either scalp, intracranial monitoring or ECoG) can be very important contributions to epilepsy surgery. Typical MRI findings are not present in one third to one half of patients with cortical dysplasia who are undergoing epilepsy neurosurgery20). Through these cases, it should be noted that imaging does not always provide adequate clinical information about the location of operation, with the structural abnormality not necessarily indicating the epileptic zone28).
Then, how should the decision on the delineation of the extent of real resection take place? In the real operative situation, ECoG can be an additional option to decide the identity of the epileptic zone and the need for additional resection after initial cortical removal, and to delineate the extent of resection because the continuous ictal-like interictal epileptiform discharges were found on ECoG in the majority of patients harboring CD8,10,14,30). At present, lesionectomy alone has produced mixed results. Some authors report favorable seizure outcomes compared with tailored cortical resections, while others report the opposite15,35). However, several studies already revealed that the complete resection of cortical dysplastic lesion and epileptogenic areas around CD are important predictors of seizure outcome7,17,21,24,29), therefore, wide tailored resection can be considered a safe option to control intractable epilepsy. This study's protocol, the tailored resection by intraoperative recording (ECoG) and functional brain mapping techniques to identify the epileptic and eloquent areas, could be a procedural option especially for CD regarding the neurosurgeon's role.
In addition, how much should be included in the adjacent brain tissue? The importance of complete resection indicates that seizures may originate from the periphery and the center of CD. Previous studies revealed better surgical outcomes after a wider extended resection, which exceeded the areas that revealed epileptic discharges on the ECoG1,36). Regarding one case with concurrent tumor, Lee and Son27) and Seo et al.31) already reported 7 cases that had the coexistence of CD and neoplasia. They found that the surgical outcome was favorable when tumor is removed with the adjacent epileptic cortex. The same result has been verified in this study. It can be a reasonable recommendation to remove mass with the conception of a tailored resection of the peritumoral epileptic zone for brain tumor surgery.
CONCLUSION
In terms of delineation of the extent of resection, this study attempted to apply more strict indications to select the surgical candidates, such as more localized ictal EEG onset via scalp and/or intracranial electrodes consistent with more definitive MRI findings. In addition, for a more practical point of view, the final extent of resection was taken into great consideration on whether it could be expanded to the adjacent gyri according to the active interictal epileptiform discharges by the intraoperative ECoG as an adjuvant guideline more than that made by preoperative evaluation.
All of the above comprehensive updated surgical strategies could contribute to improved surgical outcomes as there was a 91% positive rating with the study's experienced comprehensive epilepsy team and its observance of an individual-oriented tailored resection.