Survival Rates and Risk Factors for Cephalad and L5-S1 Adjacent Segment Degeneration after L5 Floating Lumbar Fusion : A Minimum 2-Year Follow-Up
Article information
Abstract
Objective
Although the L5-S1 has distinct structural features in comparison with other lumbar spine segments, not much is known about adjacent segment degeneration (ASD) at the L5-S1 segment. The aim of study was to compare the incidence and character of ASD of the cephalad and L5-S1 segments after L5 floating lumbar fusion.
Methods
From 2005 to 2010, 115 patients who underwent L5 floating lumber fusion were investigated. The mean follow-up period was 46.1 months. The incidence of radiological and clinical ASD of the cephalad and the L5-S1 segments was compared using survival analysis. Risk factors affecting ASD were analyzed using a log rank test and the Cox proportional hazard model.
Results
Radiological ASD of the L5-S1 segment had a statistically significant higher survival rate than that of the cephalad segment (p=0.001). However, clinical ASD of the L5-S1 segment was significantly lower survival rates than that of the cephalad segment (p=0.038). Risk factor analysis showed that disc degeneration of the cephalad segment and preoperative spinal stenosis of the L5-S1 segment were risk factors.
Conclusion
In L5 floating fusion, radiological ASD was more common in the cephalad segment and clinical ASD was more common in the L5-S1 segment. At the L5-S1 segment, the degree of spinal stenosis appears to be the most influential risk factor in ASD incidences, unlike the cephalad segment.
INTRODUCTION
Lumbar spinal fusion is effective for reducing low back pain and radiculopathy and maintaining spine stability. As techniques for spinal instrumentation and imaging have developed, lumbar spine fusion is more widely performed than before5). However, adjacent segment degeneration (ASD) may occur following lumbar spine fusion because of increases in intervertebral stress and adjacent segment motions. ASD can be further categorized as radiological ASD (RASD), clinical ASD (CASD), and reoperation (i.e., additional decompression or arthrodesis). The rate of RASD is 5.2-100%; CASD, 5.2-18.5%; and reoperation, 2.6-27.4%5,10,12,18,21). Although numerous studies have attempted to study ASD after lumbar spinal fusion, it is difficult to explain the relations between radiological outcomes and clinical symptoms in a consistent manner4). And, many risk factors are known, including degeneration of the adjacent facet joint, fusion length, sagittal alignment, adjacent disc degeneration, lumbar stenosis, age, osteoporosis, sex, and postmenopausal state1,8,12,18,21).
The L5-S1 segment has distinctive biomechanical motions different from other lumbar segments16,22). It is related to the function of the iliolumbar ligament, which supports and stabilizes the lumbosacral junction6,15). Accordingly, the L5-S1 degeneration rate in patients who undergo L5 floating fusion (i.e., lumbar fusion stopped at L5) is 3.6-10.0%, which is lower than the rate of ASD in the proximal fusion level5,6,14). Our experiences suggest that L5 radiculopathy is common after L5 floating fusion. Additionally, disc degeneration at the L5-S1 segment occurs frequently in cases when marked degeneration occurs at the L3-4 and L4-5 segments2). Therefore, we attempted to study the radiological and clinical outcomes of ASD at the L5-S1 segment after L5 floating fusion. This study aimed to compare ASD at the cephalad and L5-S1 segments after L5 floating fusion and to elucidate the characteristics of ASD at the L5-S1 segment. Furthermore, this study aimed to identify the risk factors of ASD at the cephalad and the L5-S1 segments and any other factors affecting clinical outcomes.
MATERIALS AND METHODS
Between 2005 and 2010, L5 floating lumbar fusion was performed for 236 patients, and among them, 115 (44 male, 71 female) patients who were observed for more than 2 years were included in the study (Table 1). Patients treated with L5 floating lumbar fusion had severe low back pain and/or radiculopathy, which could not be improved through conservative management. Patients were excluded if operations were initiated because of acute fracture, malignancy, acute infection, preoperative spondylolisthesis ≥4 mm, or severe disc degeneration (Pfirrmann Classification)20) in adjacent segments. All patients underwent transforaminal lumbar interbody fusion by a single surgeon (second author) following an identical procedure, and no decompression was performed in adjacent segments. Whitecloud's function scale was used to measure functional outcomes6,24).
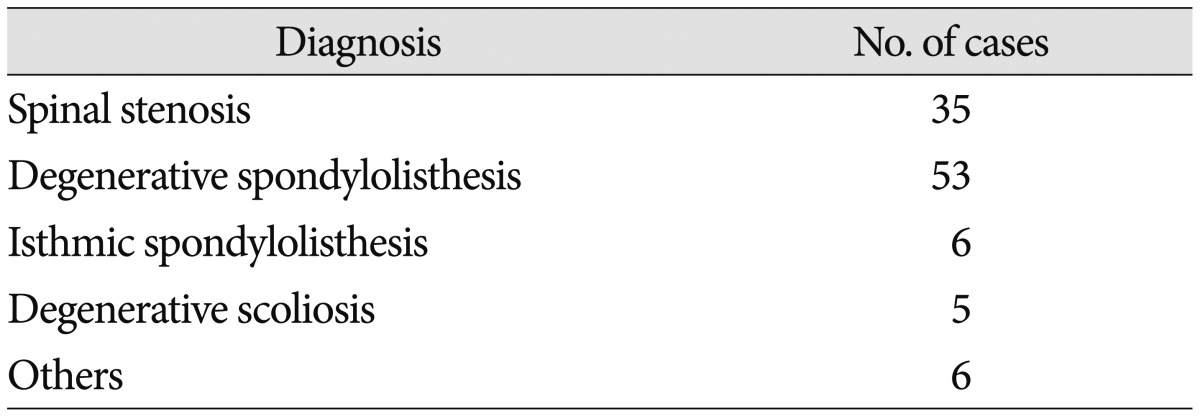
Patient population by initial diagnosis
ASD was defined as newly developed lesions in the adjacent segments of patients who did not have radiological and/or clinical changes within 6 months postoperatively12). ASD was further categorized as RASD, CASD, and reoperation, and the cephalad ASD and L5-S1 segment ASD were separated.
RASD was defined using plain radiography as follows : 1) instability : ≥10° angulations based on flexion/extension lateral radiographs; 2) listhesis >4 mm : anterior, posterior, or lateral translation on anteroposterior and lateral radiographs; and 3) an increase to grade 2 in disc degeneration based on the University of California at Los Angeles grading scale6). Changes in the cephalad and L5-S1 segments were evaluated before and after surgery and at each follow-up using plain radiography. CASD was defined as newly developed back pain and/or radiculopathy in relation to the adjacent operation sites. The time to RASD, CASD, and reoperation were also measured.
The osteoarthritis grade of the facet joint was evaluated based on preoperative computed tomography23). Disc degeneration was evaluated using the Pfirrmann 5-grade classification20), and spinal stenosis was evaluated using 4-grade classification on T2-weighted magnetic resonance imaging before surgery7). The measurements and evaluations based on radiography were initially obtained by the first author as an independent observer, and the two other surgeons reviewed and confirmed the results.
For RASD, CASD, and reoperation at the cephalad and L5-S1 segments, the 36- and 60-month survival incidences were investigated using the Kaplan-Meier survivorship method. Using a log rank test, we compared RASD, CASD, and reoperation in the cephalad and L5-S1 segments with respect to the other factors. Moreover, the risk factors for RASD, CASD, and reoperation on the cephalad and L5-S1 segments were investigated using the Cox proportional hazard model. Correlation analysis was performed using a Spearman rank test to determine the contribution of independent variables to the measured functional outcome. All statistical analyses were conducted using SPSS version 18.0.0 (SPSS Inc., Chicago, IL, USA), and a p value <0.05 was considered statistically significant.
RESULTS
Patient age at the time of operation was 58.2±10.0 years (range, 23-77 years). The levels of operations were L4-5 (64 patients), L3-5 (43 patients), and L2-5 (8 patients). The mean follow-up period was 46.1 months (range, 24-89 months).
In 115 patients, 25 (21.7%) and 8 (7.0%) had cephalad and L5-S1 segment RASD, respectively. Cephalad segment RASD was related to spinal instability (n=9, 36%) and spondylolisthesis (n=14, 56%), whereas L5-S1 segment RASD was mainly due to disc degeneration (n=6, 75%). CASD was found on the cephalad segment in 4 patients (3.5%) and on the L5-S1 segment in 12 patients (8.7%). The main symptom of cephalad segment CASD was back pain, and for L5-S1 segment CASD, it was either L5 radiculopathy (n=8) or back pain (n=4). Among patients with CASD, 2 cephalad segment cases (50%) and 5 L5-S1 segment cases (41.7%) were treated with reoperations (Table 2).
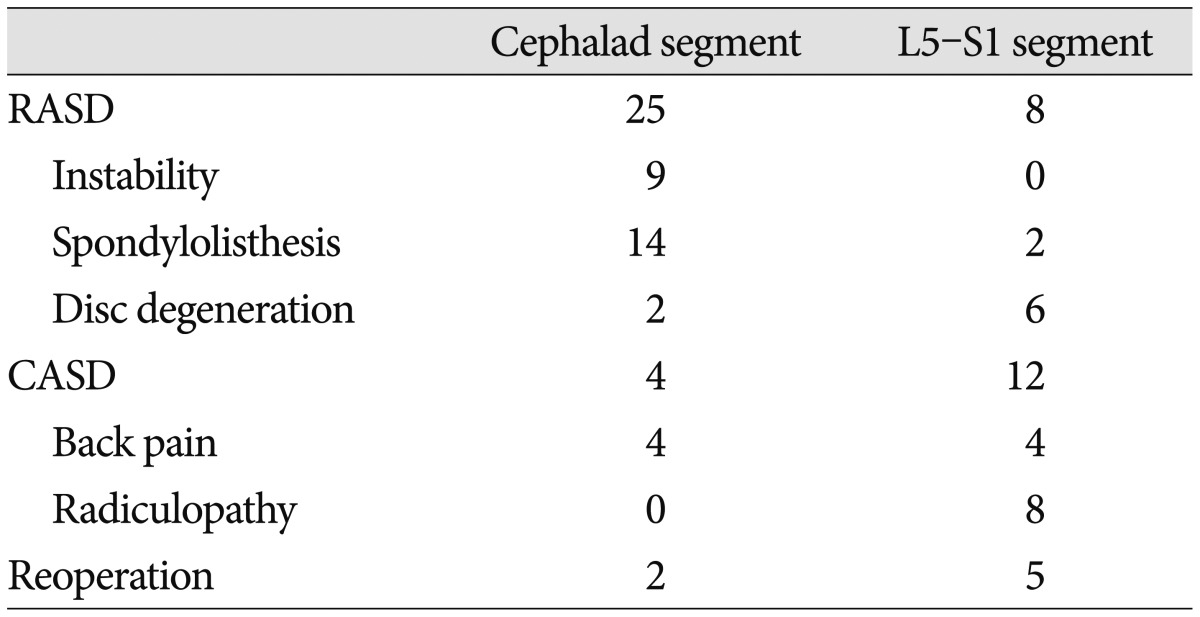
The incidence and character of the RASD, CASD, and reoperation at the cephalad and caudad (L5-S1) segments
Among 25 patients who had RASD at the cephalad segment, CASD was found in 4 patients (15.0%); however, CASD was not found among patients without RASD. Among 5 patients who had RASD at the L5-S1 segment, 3 patients (60.0%) had CASD. Moreover, 9 (8.4%) of 107 patients who did not have RASD when evaluated by plain radiography were found to have CASD (Table 3).

The prevalence of the RASD and CASD at the cephalad and caudad (L5-S1) segments
The occurrence rates of RASD and CASD at the cephalad and L5-S1 segments were compared using the Kaplan-Meier survivorship method. The 36- and 60-month survival rates of RASD at the cephalad segment were 88.0% and 63.2%, respectively, whereas those of RASD at the L5-S1 segment were 95.9% and 91.9%, respectively; this implies that RASD is more common at the cephalad segment than at the L5-S1 segment level (p=0.001) (Fig. 1). Conversely, the 36- and 60-month survival rates of CASD at the cephalad segment were 99.1% and 91.7%, respectively, and 91.2% and 87.6% at the L5-S1 segment, respectively; this implies that CASD was more common at the L5-S1 segment than at the cephalad segment level (p=0.038) (Fig. 2). No differences were found in the patients undergoing reoperation between the two groups (p=0.288) (Table 4, Fig. 3).

Kaplan-Meier survivorship curve. The survival rate of the cephalad and caudad (L5-S1) segments for radiological adjacent segment degeneration (ASD) (p=0.001).

Kaplan-Meier survivorship curve. The survival rate of the cephalad and caudad (L5-S1) segments for clinical adjacent segment degeneration (ASD) (p=0.038).
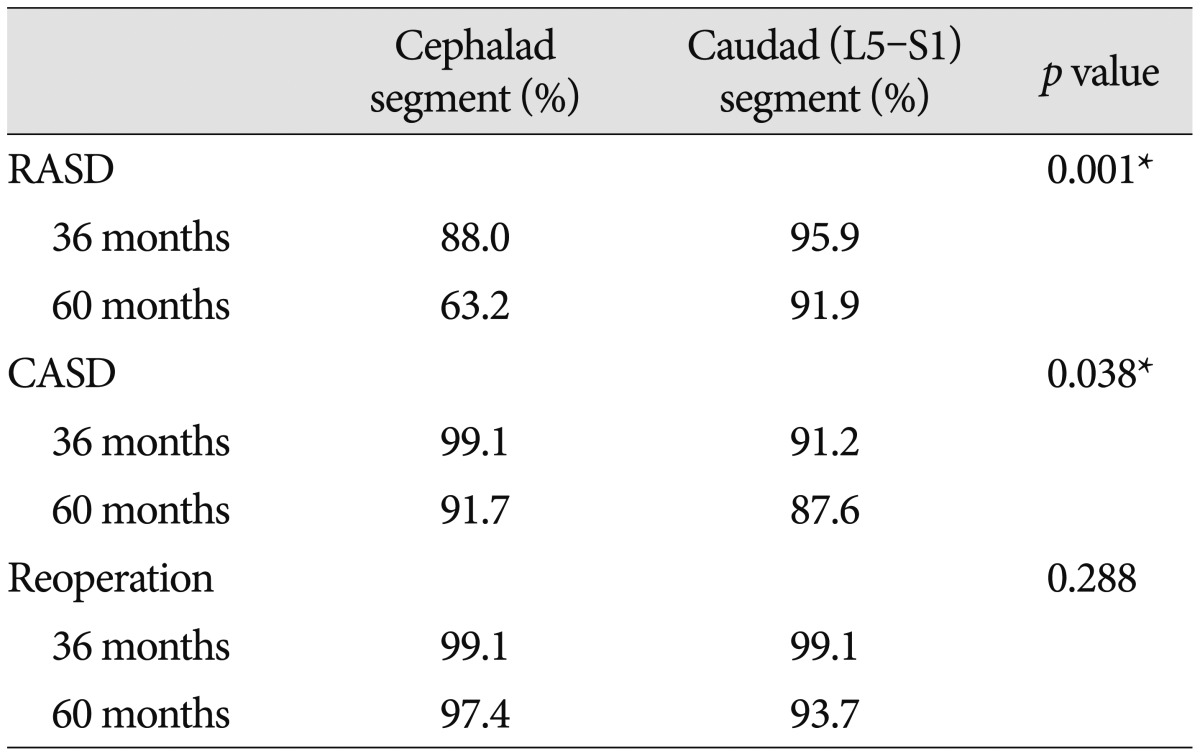
The survival rate of the cephalad and caudad (L5-S1) segments at 36 and 60 months

Kaplan-Meier survivorship curve. The survival rate of the cephalad and caudad (L5-S1) segments for reoperation (p=0.288).
RASD, CASD, and reoperation based on sex, age (>60 years), level (single vs. multiple), subchondral bone mineral density (T-score 2.5 criteria), disc degeneration (grade I/II/III vs. IV/V), spinal stenosis (none/mild vs. moderate/severe), and facet joint osteoarthritis (grade 0/1 vs. 2/3) were compared using a log rank test. The occurrence of RASD at the cephalad segment was significantly correlated to preoperative disc degeneration (p=0.010), and CASD was significantly related to disc degeneration and facet joint osteoarthritis before surgery (p=0.034, 0.049). In cases involving the L5-S1 segment, RASD, CASD, and reoperation were more common when spinal stenosis was higher than moderate (p=0.026, 0.015, 0.001, respectively) (Table 5).
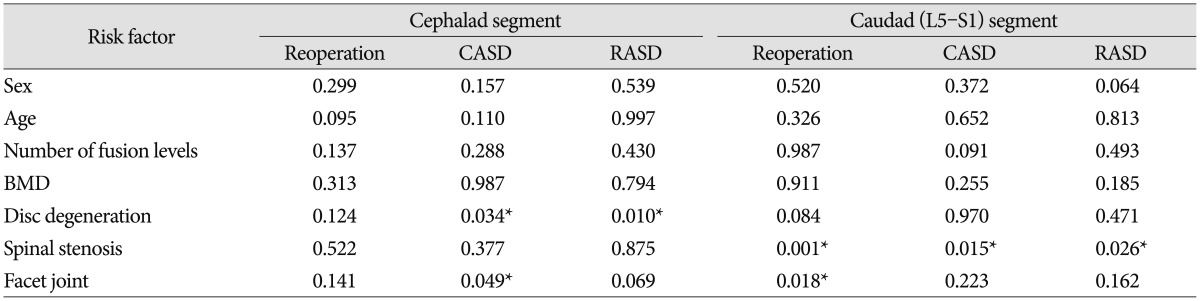
The result of prognostic factors analysis by the log rank test
The Cox proportional hazard model analysis showed that disc degeneration [p=0.002; odds ratio (OR)=5.1; 95% confidence interval (CI), 1.8-14.6] and occurrence of RASD at the cephalad segment and degree of spinal stenosis (p=0.008; OR=7.4; 95% CI, 2.0-36.3) was significantly correlated with CASD at the L5-S1 segment.
Based on Whitecloud's criteria for outcomes, 52 patients appeared to have excellent outcomes, 44 patients had good outcomes, 12 had fair outcomes, and 7 had poor outcomes. Factors that were correlated with outcomes based on Spearman rank correlation were age [Spearman's rho (r)=0.20, p=0.029], segment level (r=0.25, p=0.008), disc degeneration before surgery on the cephalad and L5-S1 segments (r=0.25, p=0.007 and r=0.22, p=0.017, respectively), spinal stenosis before surgery at the cephalad and L5-S1 segments (r=0.19, p=0.046 and r=0.19, p=0.042, respectively), and facet joint osteoarthritis grade at the cephalad segment (r=0.22, p=0.016).
DISCUSSION
The lumbosacral junction has distinctive structural and biomechanical characteristics that are different from those of other lumbar spine segments. During segmental flexion, the degree of flexion gradually increases as it approaches the lower lumbar segment, while the flexion angle decreases at the L5-S1 segment16,19,22). This occurs because the posterior band of the iliolumbar ligament and the relative thicknesses of the L5 transverse process affect the range of motion of the lumbosacral segment and therefore maintain stability13,17). Many authors have reported that ASD occurs more at the proximal segment than at the distal segment3,4,5). However, Sears et al.21) found that in 404 patients who underwent L5 floating fusion at 4 levels (excluding long segment fusion), cephalad ASD was found in 27 patients, caudal ASD in 27 patients, and both cephalad and caudal ASD in 5 patients, which showed that the rates of reoperation between the cephalad and L5-S1 segments ASD were identical. Similarly, our study found that reoperation on the lumbosacral junction was similar to that on the cephalad segment; however, because of the biomechanical influence of the lumbosacral junction, radiological and clinical outcomes were different in patients with cephalad segment involvement.
ASD is caused by excessive mobility because of disc and facet joint degeneration on segments adjacent to fusion sites, which results in facet joint degeneration and induces spondylolisthesis and spinal instability leading to back pain4). Furthermore, foramen and canal stenosis is caused by facet joint degeneration and hypertrophy, thickening of the ligamentum flavum, and disc degeneration, which leads to radiculopathy6). In particular, foraminal stenosis is markedly more common than central or lateral recess stenosis in the L5-S1 segments2). In our present study, back pain seemed to be the main symptom at the cephalad segment because of spinal instability and spondylolisthesis, and L5 radiculopathy seemed to be the main symptom due to foraminal stenosis in the L5-S1 segment.
In cephalad segment ASD, clinical symptoms were found only in RASD patients. However, at the L5-S1 segment, clinical symptoms were found regardless of presence of RASD on plain radiographs. When RASD was evaluated based on plain radiography, sensitivity was 100% but specificity was only 18.9% at the cephalad segment. However, at the L5-S1 segment, sensitivity and specificity were 25% and 4.9%, respectively, indicating lower diagnostic values. Cheh et al.4) reported sensitivity and specificity as 78.9% and 26.7%, respectively. This finding seems to have resulted from development of ASD in proximal areas of prior fusion (88.8%, 71 out of 80 cases). Instability occurs less frequently at L5-S1 because of the existence of the iliolumbar ligament. Furthermore, since L5-S1 is overlapped by the pubic bone on plain radiography, ill-defined radiographic images are produced, which may explain the low sensitivity and specificity. The cephalad segment has an especially high sensitivity and provides a clue regarding requirement of further evaluation. However, at the L5-S1 segment, plain radiography cannot provide sufficient information; therefore, additional tests are recommended. Similar results were found on comparative studies of RASD and CASD at the cephalad and L5-S1 segments.
Kim et al.9) reported that RASD was found at a rate of 55.9% with unilateral pedicle screw insertion and 72.9% with bilateral pedicle screw insertion in a minimum 10-year follow-up. Cheh et al.4) reported that 42.6% (80 of 188 patients) had RASD in a minimum 5-year follow-up period, and among those, 56.3% (45 of 80 patients) had CASD. In this study, we investigated the occurrence rates of RASD and CASD at the cephalad and L5-S1 segments in L5 floating fusion and compared the results. After 5 years, 36.8% had RASD at the cephalad segment and 8.9% at the L5-S1 segment. The occurrence rates of CASD were 8.3% at the cephalad segment and 12.4% at the L5-S1 segment.
In our study, the radiological and clinical survival rates were 92% and 88%, respectively, at the L5-S1 segment after 5 years. Ghiselli et al.6) reported that the radiological survival rate was 90% for L4-5 fusion at 10 years after surgery. Other authors reported that among patients with L5-S1 involvement, only 3-5% needed to be operated on6,12). However, the nonunion rate in the lumbosacral junction was 14.4% at 59 months, which was higher than the CASD and reoperation rate of the L5-S1 segment11). Therefore, it is not necessary to additionally include the L5-S1 segment. Moreover, preservation of the L5-S1 segment reduces buttock stiffness and diffuses pressures concentrated on the cephalad adjacent segment to the caudad adjacent segment14). Furthermore, fusion of the L5-S1 segment may involve longer operation, increased complications, subsequent degeneration of the sacroiliac joint, altered gait mechanics, and an increased pseudoarthrosis rate; this further supports the needlessness of including the L5-S1 segment2).
Ghiselli et al.5) reported that reoperations were required in 16.5% of patients within 5 years and in 36.1% within 10 years, and that new diseases occurred in the adjacent level at an annual rate of 3.9%. Sears et al.21) reported that 13% of patients required reoperations after 43 months from the initial surgery, and that new diseases were found in the adjacent sites at an annual rate of 2.2%. The prevalence for reoperation following L5 floating fusion at 10 years was 14.7%. In this study, 2.6% of patients with cephalad segment involvement and 6.3% of patients with L5-S1 segment involvement required reoperations within 5 years after surgery. This is partly because most of the patients in the study group had 1-2 level involvement, and since no patients underwent long-level fusion, ASD-related reoperations were required to a lesser extent.
Numerous studies have investigated the risk factors for RASD, CASD, and reoperation. Age, disc and facet joint degeneration, and multiple levels are well-known factors1,5,8,9,12,21). Among these factors that influence ASD, we found that factors affecting the cephalad and L5-S1 segments differ after L5 floating fusion. In our study, preoperative disc degeneration was the most significant factor for ASD at the cephalad segment with preoperative spinal stenosis at the L5-S1 segment.
The present study has limitations. First, the study is retrospective, and the follow-up periods and evaluation time of the clinical outcomes were not consistent. Second, only 115 patients (48.7%) of 236 patients were followed up, and the mean follow-up period was 46 months, which is shorter than that in previous studies. Third, since the definitions of RASD and CASD were different depending on authors, it was difficult to make accurate comparisons with previous studies. Especially in cases involving clinical ASD, the diversity in treatment methods (i.e., medication and injection) and indication of surgery were difficult to define. Therefore, a long-term, randomized, prospective study on expanded groups of patients is warranted.
CONCLUSION
In L5 floating fusion, ASD at the L5-S1 and cephalad segments appear to have different characteristics. RASD was more common at the cephalad segment, and CASD was more common at the L5-S1 segment. Occurrences of spinal instability, spondylolisthesis, and back pain were the major symptoms at the cephalad segment, and preoperative disc degeneration was the most significant factor influencing the outcomes. However, disc degeneration and radiculopathy were the main symptoms at the L5-S1 segment, and the most significant factor was preoperative spinal stenosis.