Analyses Using Micro-CT Scans and Tissue Staining on New Bone Formation and Bone Fusion According to the Timing of Cranioplasty via Frozen Autologous Bone Flaps in Rabbits : A Preliminary Report
Article information
Abstract
Objective
The timing of cranioplasty and method of bone flap storage are known risk factors of non-union and resorption of bone flaps. In this animal experimental study, we evaluated the efficacy of cranioplasty using frozen autologous bone flap, and examined whether the timing of cranioplasty after craniectomy affects bone fusion and new bone formation.
Methods
Total 8 rabbits (male, older than 16 weeks) were divided into two groups of early cranioplasty group (EG, 4 rabbits) and delayed cranioplasty group (DG, 4 rabbits). The rabbits of each group were performed cranioplasty via frozen autologous bone flaps 4 weeks (EG) and 8 weeks (DG) after craniectomy. In order to obtain control data, the cranioplasty immediate after craniectomy were made on the contralateral cranial bone of the rabbits (control group, CG).The bone fusion and new bone formation were evaluated by micro-CT scan and histological examination 8 weeks after cranioplasty on both groups.
Results
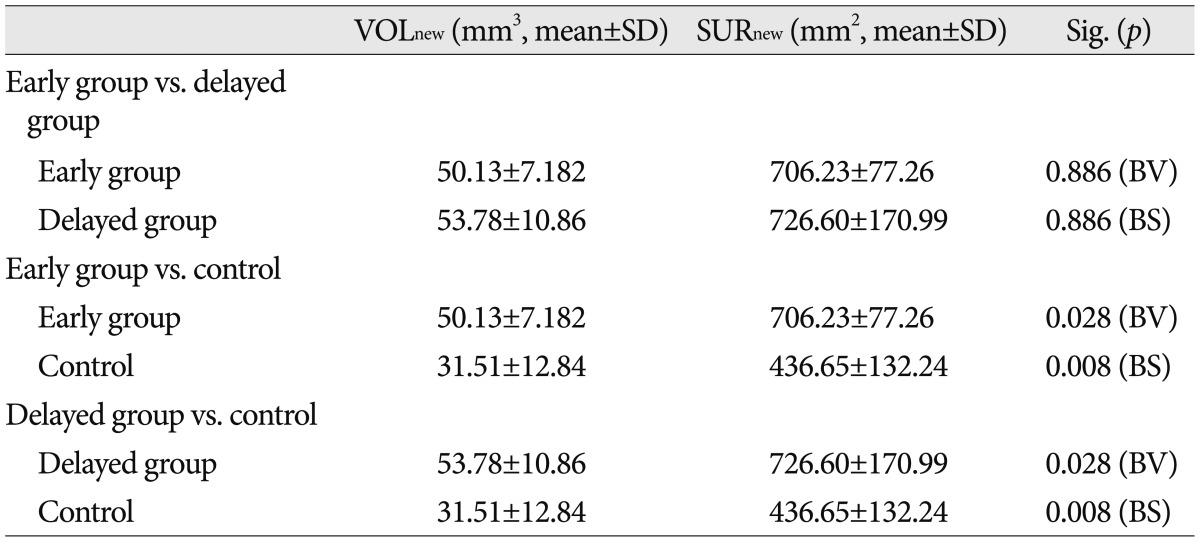
In the micro-CT scans, the mean values of the volume and the surface of new bone were 50.13±7.18 mm3 and 706.23±77.26 mm2 in EG, 53.78±10.86 mm3 and 726.60±170.99 mm2 in DG, and 31.51±12.84 mm3 and 436.65±132.24 mm2 in CG. In the statistical results, significant differences were shown between EG and CG and between DG and CG (volume : p=0.028 and surface : p=0.008). The histological results confirmed new bone formation in all rabbits.
Conclusion
We observed new bone formation on all the frozen autologous bone flaps that was stored within 8 weeks. The timing of cranioplasty may showed no difference of degree of new bone formation. Not only the healing period after cranioplasty but the time interval from craniectomy to cranioplasty could affect the new bone formation.
INTRODUCTION
Decompressive craniectomy is very effective method of reducing intracranial pressure. In a recent prospective clinical trial, decompressive craniectomy was confirmed to have reduced the mortality by 50% in the patients with cerebral edema caused by cerebral infarction17,23,42,43). In addition, it was effective for cerebral edema caused by traumatic brain damage2,19), subarachnoid hemorrhage10,16), intracerebral hemorrhage29), and cranial venous and sinus thromboses7). Cranioplasty is performed after craniectomy when intracranial pressure is under control for functional and aesthetic restorations. During the cranioplasty procedure, autologous bone flaps are preferably used due to their advantages in storage, viability, cost, prevention of disease transmission, and aesthetics. However, cranioplasty that uses the autologous bone flap has a risk of developing complications such as infection, intracranial hemorrhage, seizure, and hydrocephalus. Long-term complications, such as bone flap resorption and bone non-union, have incidence rates that reached 2-17%18,21,33). According to the studies on human cranioplasty, the timing of performing cranioplasty is one of the critical factors that may develop autologous bone flap resorption and bone non-union15). Although generally accepted concept about timing of cranioplasty using autologous bone is that early cranioplasty has more risk of infection and delayed cranioplasty has risk of non-union or resoprtion of bone flap4,6,25,44), the debates are still remained. Another report showed non-union and/or resorption of bone flap occurred more frequently on early cranioplasty patients who had surgery-related infections35). And the other said there were no relation of bone non-union to timing of cranioplasty32).
In this study, cranioplasty was performed on rabbits using frozen autologous bone flaps, while the levels of new bone formation and bone fusion after craniectomy were observed, according to the timing of cranioplasty to evaluate its efficacy.
MATERIALS AND METHODS
Experimental animals and groups
Experiments were conducted in compliance with the animal experimentation ethics upon approval from the Institutional Animal Care and Use Committee of our institute. Eight adult (16 weeks or older) male New Zealand white rabbits with the body weights ranging from 3.2 kg to 4.2 kg were used in this study. Four out of eight subjects were assigned to the delayed cranioplasty group (DG), and the remaining four subjects were assigned to the early cranioplasty group (EG). At day 0, craniectomy was performed at the right frontoparietal bone of the DG rabbit, and the obtained bone flap was stored in a freezer at a temperature of -80℃. At day 28 or week 4, bone defect was made in the right frontoparietal bone of the EG rabbit, and then, the bone flap was stored at the same condition. At day 56 or week 8, the frozen bone flap was fixed on the bone defect area of the DG and EG rabbits. In order to obtain control data, the same procedures were made on the left cranial bone of the rabbits, and the bone flap was immediately fixed (control group, CG). At day 112 or week 16, the EG and DG rabbits were sacrificed to conduct radiological and histological tests on their cranial bones (Fig. 1).
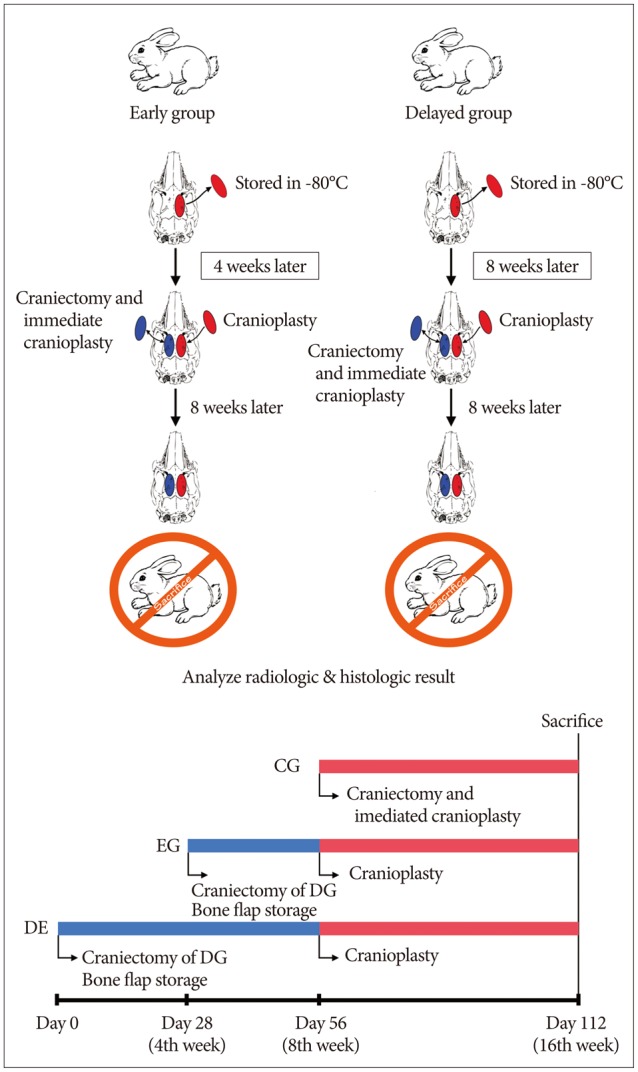
Diagram and time-line of experimental schedule. Eight rabbits were divided into two groups of the delayed cranioplasty group (DG, 4 rabbits) and the early cranioplasty group (EG, 4 rabbits). The craniectomy was performed on the right side cranial bone of the DG rabbit at day 0, and EG rabbit at day 28. The obtained bone flap was stored in a freezer of -80℃. At day 56, cranioplasty was performed on both groups via the frozen bone flap. In order to obtain control data, the craniectomy was made on the left cranial bone of the rabbit, and the bone flap was immediately fixed (control group). At day 112, the EG and DG rabbits were sacrificed.
The time span between craniectomy and cranioplasty was the healing time of bone defect and defined as "the primary healing time", while the time between the cranioplasty and rabbit sacrifice was the bone formation time of the gap between bone flap and cranium and defined as "the secondary healing time".
Preparation of the experimental model
Formation of bone defect and storage of bone flap
In order to induce anesthesia on the rabbits, 0.5 mL/kg of ketamin HCl (Ketalar, Yuhan Corporation, Seoul, Korea) and 0.25 mg/kg of xylazine HCl (Rompun, Bayer, Pittsburgh, PA, USA) were mixed and injected intramuscularly. For local anesthesia and hemorrhage control, 2% lidocaine HCl (Yuhan Corporation, Seoul, Korea) containing 1 : 100000 epinephrine was injected subcutaneously. After a 4-cm long incision was made along the midline of the cranial skin, the muscles and periosteum were incised layer by layer to expose the cranial bone (Fig. 2A). In order to make the bone flap, a bone flap margin was formed 3 mm lateral to the sagittal suture, which was located at the right side for the experimental groups and the left side for the control group, using a trephine drill with a 10-mm outer diameter and 9-mm inner diameter. To avoid damaging the dura mater, the inner table of the cortical bone was left (Fig. 2B, C). Using a 1-mm round burr, the space between the round bone-flap margin and the cranial bone was expanded out of the bone flap in order to create a 12-mm bone defect diameter (Fig. 2D). The reason why the size of the bone defect was decided at 12 mm was that the critical bone defect, which did not cause a spontaneous bone healing in rabbits, was reported to be 12 mm or larger37). The dura mater was carefully exposed (Fig. 2E), while the 9-mm bone flap was lifted in order to form a bone defect (Fig. 2F). The blood and soft tissues of the bone flap were removed, and the flap was wrapped up with gauze soaked sterilized saline. Each bone flap was put in a sterilized and labeled plastic container before they were kept in a freezer (CLN-540U, Nihon freezer, Tokyo, Japan) at a temperature of -80℃. Layer-to-layer suture was performed using absorbable sutures (3-0 vycryl) and unabsorbable sutures (3-0 nylon).
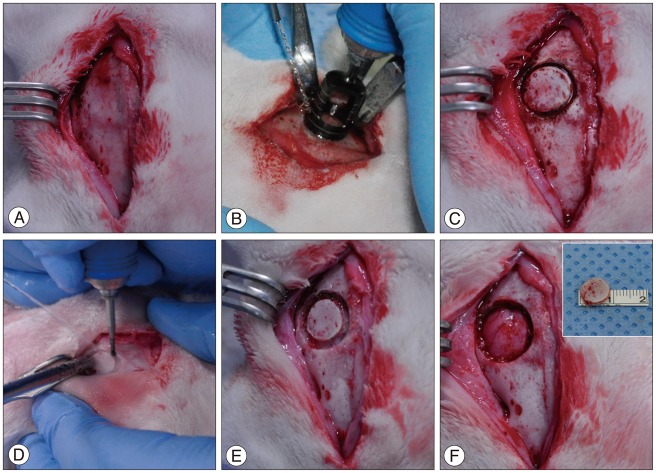
Preparation of the experimental model of formation of bone defect and bone flap. After incision was made along the midline of the cranial skin, the muscles and periosteum were incised layer by layer to expose the cranial bone (A). The bone flap margin was formed 3-mm lateral to the sagittal suture, using a trephine drill with a 10-mm outer diameter and 9-mm inner diameter. To avoid damaging the dura mater, the inner table of the cortical bone was left (B and C). Using a 1-mm round burr, the space between the bone-flap margin and the cranial bone was expanded out of the bone flap in order to create a 12-mm bone defect diameter (D), and the dura mater was carefully exposed (E). The 9-mm bone flap was lifted up and the bone defect was formed (F).
Cranioplasty
After anesthesia and skin incision that mentioned above, the fibrous tissues, which were formed during the primary healing time, were removed using a curette in order to expose the bone defect area (Fig. 3A). Afterwards, the autologous bone flap, which has been kept in the freezer, was applied to each labeled rabbit in order to perform cranioplasty. The cranial bone and the bone flap were fixed using a titanium-alloy miniplate and 3-mm screws (Synthes Inc., West Chester, PA, USA) (Fig. 3B, C). Using the same method, CG was formed on the left cranium of the rabbit (Fig. 3D).
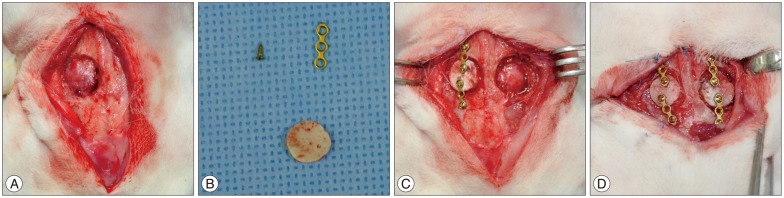
The fibrous tissues were removed in order to expose the bone defect area (A). Afterwards, the autologous bone flap (B), which has been kept in the freezer, was applied to each labeled rabbit in order to perform cranioplasty, and the bone flap was fixed to cranial bone using a titanium-alloy miniplate and screws (C). Using the same method, the control group was formed on the left cranium of the rabbit (D).
Radiologic observation
At week 16, the cranial bone of the sacrificed rabbit was scanned by the micro-computed tomography (micro-CT) (SkyScan 1173, SKYSCAN, Kontich, Belgium). The 2240×2240 pixel sectional images (Fig. 4A, B) and the three dimensional reconstructed images (Nrecon reconstruction program, SKYSCAN, Kontich, Belgium) (Fig. 4C, D) were obtained. After confirming the round bone flap through the micro-CT images and 3D remodeling images, we defined the region of interest (ROI) as the region within a 14-mm diameter from center point of bone flap. We measured the bone volume (VOLROI) and the bone surface (SURROI) of ROI (Fig. 5A). From VOLROI and SURROI, the bone volume (VOLbone flap) and the bone surface (SURbone flap) of the bone flap, and the volume (VOLmetal) and the surface (SURmetal) of metal fixture were removed. Afterwards, the CT scan images (Fig. 5B) and the 3D reconstruction images (Fig. 5C) of the new bone volume (VOLnew) and the new bone surface (SURnew) were quantified and measured.
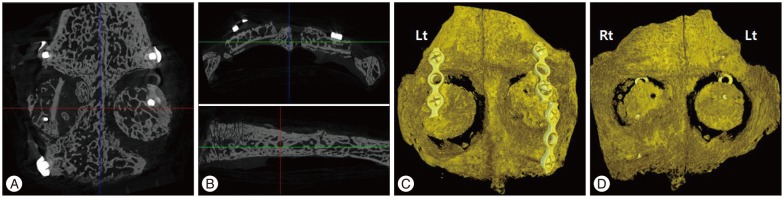
The axial sectional image (A), and coronal and sagittal sectional images (B) of computed tomography scans. The 3D reconstructed images showed outer surface (C) and inner surface (D) of cranium. The left side of cranium is experimental craniectomy site, and the right side is the control group.
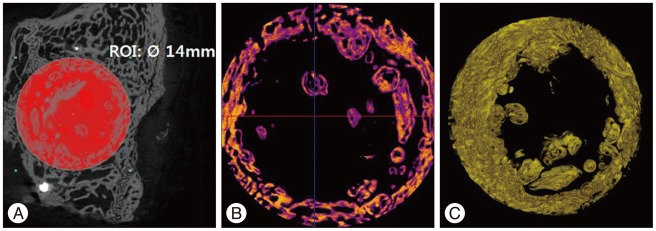
We defined the region of interest (ROI) as the region within a 14-mm diameter from center point of bone flap. We measured the bone volume (VOLROI) and the bone surface (SURROI) of ROI (A). From VOLROI and SURROI, the bone volume (VOLbone flap) and the bone surface (SURbone flap) of the bone flap, and the volume (VOLmetal) and the surface (SURmetal) of metal fixture were removed. Afterwards, the computed tomography scan images (B) and the 3D reconstruction images (C) of the new bone volume (VOLnew) and the new bone surface (SURnew) were quantified and measured.
VOLnew=VOLROI-(VOLbone flap+VOLmetal)
SURnew=SURROI-(SURbone flap+SURmetal)
Tissue processing and histological observation
After dehydration processing was completed, the graft was put in a methyl methacrylate solution in order to maintain a vacuum state. After the methyl methacrylate solution was permeated, the tissues were embedded. The tissues were put in a 5 mL of methyl methacrylate solution and 50 µL of JB-4 embedding kit component B was added in order to maintain a vacuum state for 10 minutes. Nitrogen gas was injected to be activated at room temperature (24-28℃) for 24 hours and to prepare a plastic block. The tissues were consecutively cut in a 10-µm thickness using a hard tissue cutter (Jung polycuts, Leica Biosystems, Nussloch, Germany). The sliced tissues were stained through the use of hematoxylin and eosin (H-E), while Goldner's modified Masson trichrome methods were used for optical microscopic observations.
Statistics
SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses. As a non-parametric test, Kruskal-Wallis test was used for the comparison among the DG, EG, and CG. As a post hoc test, Mann-Whitney test was used. The p values of ≤0.05 were considered significant.
RESULTS
No subject died or experienced complications such as infection, and none of them dropped out of the experiments conducted in this study. New bone formation was confirmed in all groups. The new bone formation observed in the micro-CT images was represented as bone volume (VOLnew) and bone surface (SURnew) (Table 1). The mean new bone volume of the DG was 53.78±10.86 mm3, while the mean bone surface was 726.60±170.99 mm2. The mean new bone volume and mean bone surface of the EG were 50.13±7.18 mm3 and 706.23±77.26 mm2, respectively. The mean new bone volume of the CG was 31.51±12.84 mm3, while the mean bone surface was 436.65±132.24 mm2. Statistically significant differences were observed in the mean new bone volume (p=0.024) and bone surface (p=0.007) among the three groups (Table 2). In the post hoc test, no statistically significant difference in bone volume (p=0.886) and bone surface (p=0.886) was observed between the DG and EG. When the CG was compared with the EG and DG, significant differences in bone volume (p=0.028) and bone surface (p=0.008) were observed in both comparisons (Table 3).

The new bone formation observed in the micro-CT images was represented as bone volume (VOLnew) and bone surface (SURnew)

The mean values of bone volume (VOLnew) and bone surface (SURnew) of new bone in the micro-CT images*
The post hoc test of each paired groups*
Similar to the findings in the micro-CT images, new bone formation was observed in the microscopic examination of the H-E stain and Goldner's stain in all of the rabbit tissues. The new bone formation was observed as a form of 1) a bony islet between the bone flap and the edge of the cranial bone (Fig. 6A), 2) a bony islet at the lower part of the bone flap (Fig. 6B), 3) a new bone formation at the edge of the cranial bone (Fig. 6C), and 4) a bone flap incorporation between the bone flap and the edge of the cranial bone (Fig. 6D).
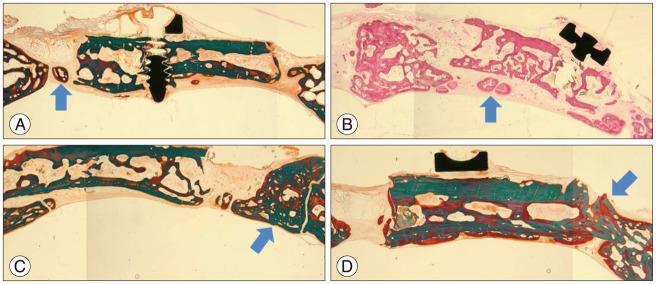
The histological patterns of new bone formation. The new bone formation was observed in the microscopic examination of the hematoxylin and eosin stain and Goldner's stain in all of the rabbit tissues. The new bone formation was observed as a form of 1) a bony islet (arrow) between the bone flap and the edge of the cranial bone (A), 2) a bony islet (arrow) at the lower part of the bone flap (B), 3) a new bone formation (arrow) at the edge of the cranial bone (C), and 4) a bone flap incorporation (arrow) between the bone flap and the edge of the cranial bone (D).
DISCUSSION
Cranioplasty, which is performed after craniectomy, has aesthetic and functional advantages, and it is used in a wide variety of diseases. However, various complications such as infection, intracranial hemorrhage, bone flap resorption, depressed bone flap, cerebral vasospasm, and hydrocephalus can develop after the cranioplasty procedure, and their incidence rate has been reported to be 15-36.5%4,5,8,14,20,27,32,36). The materials that are most frequently used in cranioplasty include autologous bone flap, poly-methyl-methacrylate (PMMA), and hydroxy apatite. The PMMA is known to show a similar frequency of complication development to that of the autologous bone flap, but its osteogenesis capability is much less than that of the autologous bone flap22,24). Hydroxy apatite can supplement the low osteogenesis capability of PMMA; however, it is expensive38). The autologous bone flap is the most widely used cranioplasty material due to its superiority in the viability, cost, prevention of disease tranmission, and aesthetics to artificial bones. Nevertheless, long-term complications such as bone non-union and resorption, which develop after the cranioplasty procedure using the autologous bone flap, are the major causes that require re-operation.
In a cranioplasty using autologous bone flap, bone flap incorporation occurs in the process of revascularization, osteoconduction, resorption, and osteogenesis12). In a bone union process, bone remodeling is completed through the repetition of bone resorption and new bone formation. Bone resorption is known to happen when problems arise during the bone reunion process39). The patient-side risk factors of bone resorption are known to include young age, traumatic cranial damage, multiple cranial fractures, and the size of the cranial defect. Meanwhile, iatrogenic factors, which include the timing of cranioplasty, have been reported13,15,21,40).
According to previous studies conducted on the timing of cranioplasty, its early performance resulted in an increase in the incidence of infection, while delayed performance resulted in an increase in the resorption of the autologous bone flap4,6,25,35,44). However, Piedra et al.32) reported that there is no difference in the frequency of the development of complications, such as bone non-union and resorption, and in the infection between the early and delayed cranioplasty performance groups. In the case of cranioplasty performed within two months after craniectomy, Schuss et al.35) reported a high frequency of infection, and resultant bone non-union and resorption. In this study, the timing of cranioplasty was set at 4 and 8 weeks with the EG and DG, and no significant difference in new bone formation was observed between the groups. Furthermore, when the frozen autologous bone flap was used on rabbits within 8 weeks, an active new bone formation was radiologically and histologically confirmed, and no significant difference in new bone formation was observed according to the freezing period.
There are several methods of storing the autologous cranial bone during the period between the procedures of craniectomy and cranioplasty. The method of freezing the autologous bone flap was introduced in the 1950s1,11,30), and since then, it has been the most widely used method. The most important factor to consider for a successful bone flap incorporation after cranioplasty is the viability of the bone flap9,28,34). Furthermore, the frozen autologous bone flap is known to have a comparatively favorable viability. When the frozen autologous bone flap was histologically analyzed at temperatures between -17℃ and -80℃, the Harvesian system of the bone tissues and structural proteins were confirmed to have remained the same regardless of the freezing period3,31,34), and the osteocytes were observed even until the 35th month after freezing34). Moreover, the freezing storage method is superior to the other methods in terms of preserving the cellular architecture30,34). An example of this is the cytoplasm of the lacunar cells, which was well preserved41). In the frozen cranial bone, new blood vessels are remodeled, and they play the role of an architectural frame that assists the growth of the osteoprogenitor cells. In addition, revascularization and infiltration of the osteoblasts occur from the edge of the cranial bone toward the bone flap34). These phenomena were also confirmed in this study. A new bone formation was observed at the edge of the cranial bone close to the bone flaps of all the DG and EG rabbits not only in the micro-CT, but also in the histological results. A bony islet formation was also observed. According to Sultan et al.41), the bony islet formation contributed to the promotion of bone flap incorporation and the reduction of bone flap resorption.
When cranioplasty is performed immediately after craniectomy, the best bone flap viability and a favorable new bone formation are usually observed41). In this study, however, the CG's new bone formation was significantly the worst when compared with the EG and DG. This may be due to the difference in the total healing time-no primary healing time in the CG, 8 weeks in the DG and 4 weeks in the EG-even though the three groups had the same secondary healing time of 8 weeks. According to Sohn et al.37), osteogenesis is a consistent process, but the time of initiating bone marrow maturity and bony islet formation in rabbits after the craniectomy procedure was 8 weeks after the surgery. This means that it takes 8 to 12 weeks to clearly observe and assess bone flap incorporation, bone remodeling, and osteogenesis. In this study, early bone flap incorporation was assessed through the early assessment on the healing process of the defect area. The primary healing time of the EG and DG was 4 weeks and 8 weeks, respectively, and their total healing time was 12 weeks and 16 weeks, respectively, while the total healing time of the CG was 8 weeks. This implies that the time of initiating new bone formation and bone flap incorporation is affected not only by the healing time after cranioplasty (secondary healing time), but also by the total period after craniectomy (primary and secondary healing time). Accordingly, the primary healing time given prior to bone transplantation may positively affect the bone healing process. The bone remodeling period after fracture on rabbits is widely known as 6-8 weeks of period-1 week of resoprtion, 0.5-1 week of reversal and 4.5-6 weeks of bone formation (on human, total 17 weeks-2 weeks of resorption, 2 weeks of reversal and 13 weeks of bone formation)26). At this point of view, the cranioplasty performing before end of bone remodeling period would have some advantages to obtain bone fusion. Thus, we think that cranioplasty performed within 8 weeks of primary healing time could result in good bone fusion.
This study had some limitations. Small sample size and the lack of power analysis for estimating appropriate sample are major concerns of this study. Despite of small sample size, the experimental result using animal models that the period between craniectomy and cranioplasty could affect the bone fusion is a meaningful result of this study. Another limitation is the different periods of total healing time and primary healing time among groups, because the duration of healing time after craniectomy has been known as one of important factors of bone fusion and union. We suggested more precisely designed study that focused on variations of healing duration among the groups should be mandatory. Considering the preliminary characteristic of this study, these limitations are expected to be surmounted on well-designed large study on future.
CONCLUSION
In this study, the cranioplasty procedure conducted on rabbits using the autologous bone flap frozen for less than 8 weeks resulted in favorable new bone formation and bone flap incorporation. These results were radiologically and histologically confirmed. Furthermore, not only the post-cranioplasty healing time (secondary healing time), but also the primary healing time, which was the time between the procedures of craniectomy and cranioplasty, were considered to positively affect the new bone formation and bone flap incorporation processes. Based on the confirmation in this study regarding the positive healing process of rabbits even during the delayed period, the delayed period between the craniectomy and cranioplasty procedures in humans may positively affect the bone flap incorporation process. Further studies on the ideal primary healing time may be required in the future.
Acknowledgements
This work was supported by a grant of Kyung Hee University in 2013 (KHU-20131019).
Experiment was conducted in compliance with the animal experimentation ethics upon approval from the Institutional Animal Care and Use Committee (IRB No. KHNMC AP 2013-007) of Kyung Hee University Hospital at Gangdong.