Straight-Forward versus Bicortical Fixation Penetrating Endplate in Lumbosacral Fixation-A Biomechanical Study
Article information
Abstract
Objective
Many lumbosacral fixation techniques have been described to offer a more screw-bone purchase. The forward anatomical fixation parallel to the endplate is still the most preferred method. Literature revealed little knowledge regarding the mechanical stability of lumbosacral trans-endplate fixation compared to the traditional trans-pedicular screw fixation method. The aim of this study is to assess the pull-out strength of lumbosacral screws penetrating the end plate and comparing it to the conventional trans-pedicular screw insertion method.
Methods
Eight lumbar and eight sacral vertebrae, with average age 69.4 years, Left pedicles of the 5th lumbar vertebrae were used for trans-endplate screw fixation, group 1A, right pedicles were used for anatomical trans-pedicular screw fixation, group 1B. In the sacral vertebrae, the right side S1 pedicles were used for trans-endplate fixation, group 2A, left side pedicles were used for anatomical trans-pedicular screw fixation, group 2B. The biomechanical tests were performed using the axial compression testing machine. All tests were applied using 2 mm/min traction speed.
Results
The average pull-out strength values of groups 1A and 1B were 403.78±11.71 N and 306.26±17.55 N, respectively. A statistical significance was detected with p=0.012. The average pull-out strength values of groups 2A and 2B were 388.73±17.03 N and 299.84±17.52 N, respectively. A statistical significance was detected with p=0.012.
Conclusion
The trans-endplate lumbosacral fixation method is a trustable fixation method with a stronger screw-bone purchase and offer a good alternative for surgeons specially in patients with osteoporosis.
INTRODUCTION
Lumbosacral segment fixation has been used frequently by many surgeons to enhance fusion and segmental stability to allow an early rehabilitation program. Different techniques have been described in the literature in a trial to create a more stable lumbar and sacral screws fixation. In the lumbar region, the forward anatomical fixation parallel to the endplate and the bicortical screw fixation through the anterior cortex parallel to the upper sacral endplate techniques, are still the most preferred methods of fixation by many spine surgeons3,21). Several studies demonstrated insufficiency of lumbar and sacral screw fixation mainly associated to the biological and mechanical features of the lumbosacral segment, the low sacral bone stock and the large cantilever deforming forces applied to the distal instrumentation from the long lever arm of the fixation constructs extending above the lumbosacral segment1,11). Variant methods of lumbosacral screw fixation have been described in different studies aiming to obtain a stronger screw-bone anchor2,11). The loss of lumbosacral fixation stability is a very well-known complication particularly in patients with poor bone quality. For that reason, many novel strategies have been developed to obtain an enhanced pull-out strength to achieve a more rigid construct2,9).
To increase the screw-bone pull-out purchase of pedicle screws in the lumbar spine segment, different trials have been introduced to alter the classical screw trajectory to permit the screw experiencing a higher density bone mass. In surgical practice, the currently used traditional pedicle screw trajectory is the trans-pedicular path, which is either following the anatomic axis of the pedicle directed 22° in the cephalocaudal direction in the sagittal plane or inserted parallel to the superior end plate of the vertebral body in the sagittal plane5,8,15).
The sacral screws most of the time are inserted bicortically, where they are directed medially parallel to the end plate or laterally into the sacra ala2,15,16). However many researchers have demonstrated the advantages of anteromedial screws replacement when compared to the anterolateral ones regarding the biomechanical stability and the neurological safety14,17,20). On the other hand, some studies have focused on the safety of the anteromedial bicortical sacral screws and have concluded that some vital structures like the middle sacral artery and vein, the common iliac artery and vein, the nerve root of L5, the colon and the sympathetic system chain, are exposed to injury during instrumentation7,18).
Recent studies have demonstrated the superiority of sacral trans-pedicular screw fixation penetrating the upper end plate in terms of pull-out strength13,19). However, searching the literature revealed little knowledge regarding the mechanical stability of lumbar and sacral trans-endplate fixation method compared to the traditional trans-pedicular screws fixation method.
The main purpose of this biomechanical study is to assess the pull-out strength of lumbar and sacral screws penetrating the end plate (trans-endplate method) and comparing it to the conventional trans-pedicular screw insertion method.
MATERIALS AND METHODS
After getting the approval of the ethical committee, reference number 2–11/01/2017, eight lumbar and eight sacral vertebral segments were obtained. Cadaveric samples were preserved in formalin based dilution for at less than one year. Donors were eight men. The lumbosacral segments were free from infections, tumors, congenital or traumatic conditions. The vertebral specimens were isolated and denuded of all paravertebral soft tissue. The left pedicles of the 5th lumbar vertebrae were used for trans-endplate screw fixation penetrating the upper end plate, where considered as group 1A. Starting from the level of the inferior border of the transverse process, just 2 mm distal to the pedicle entrance, the transendplate lumbar pedicle screw was introduced 30° cranially to penetrate the superolateral anterior aspect of the end plate (Figs. 1B and 2), whereas the right pedicles of the 5th lumbar vertebrae were used for anatomical trans-pedicular screw fixation through the body parallel to the end plate, group 1B (Figs. 1A and 2).
A : Traditional trans-pedicular screw fixation through the body parallel to the end plate. B : Trans-endplate screw fixation penetrating the upper end plate, starting from the level of the inferior border of the transverse process, just 2 mm distal to the pedicle entrance, the trans-endplate lumbar pedicle screw is introduced 30° cranially to penetrate the superolateral anterior aspect of the end plate.
The left pedicles of the 5th lumbar vertebrae were used for transendplate screw fixation penetrating the upper end plate, 2 mm distal to the pedicle entrance the lumbar pedicle screw was introduced 30° cranially to penetrate the superolateral and anterior aspect of the end plate. The right sides of the 5th lumbar vertebrae were used for anatomical transpedicular screw fixation through the body parallel to the end plate.
In the first sacral vertebrae, the right side S1 pedicles were used for trans-endplate fixation penetrating S1 upper end plate, just 2 mm distal to the pedicle entrance the screw was directed cranially 30° to penetrate the superolateral anterior aspect of the upper end plate of S1, where considered as group 2A. Whereas the left side pedicles of S1 vertebrae were used for anatomical trans-pedicular screw fixation through the body of S1 without penetrating the anterior cortex, group 2B (Fig. 3).
The right sides of S1 pedicles were used for trans-endplate fixation penetrating S1 upper end plate, just 2 mm distal to the pedicle entrance the screw was directed cranially 30° to penetrate the superolateral and anterior aspect of the upper end plate of S1. The left side pedicles of S1 vertebra were used for anatomical trans-pedicular screw fixation through the body of S1 without penetrating the anterior cortex.
In order to minimize the bone density difference between the examined cadaveric samples, biomechanical tests were submitted on the same cadaveric samples.
The body of the vertebrae was securely fixed with a metal grasp machine, whereas the poly-axial screw heads were connected with a hook directly molded to the testing machine (Fig. 2). The biomechanical tests were performed using the axial compression testing machine (AG-I 10 kN, Shimadzu Shikenki Engineering Co., Ltd, Shimadzu, Japan). All tests were applied using 2 mm/min traction speed (Fig. 4).

The biomechanical tests were performed using the axial compression testing machine (AG-I 10 kN, Shimadzu Shikenki Engineering Co., Ltd, Shimadzu, Japan). All tests were applied using 2 mm/min traction speed.
The SPSS version 15 (SPSS Inc., Chicago, IL, USA) was used. For the statistical analysis the Wilcoxon test was conducted. Statistical significance level was set up at p<0.05.
RESULTS
The average value of the pull-out strength of group 1A was 403.78±11.71 N, whereas the average value of group 1B was 306.26±17.55 N. There was a statistical significance between the two groups with p=0.012. The average value of the pullout strength for group 2A was 388.73±17.03 N, whereas the average value for group 2B was 299.84±17.52 N. A statistical significance was detected between the two groups with p=0.012 (Table 1, Fig. 5).
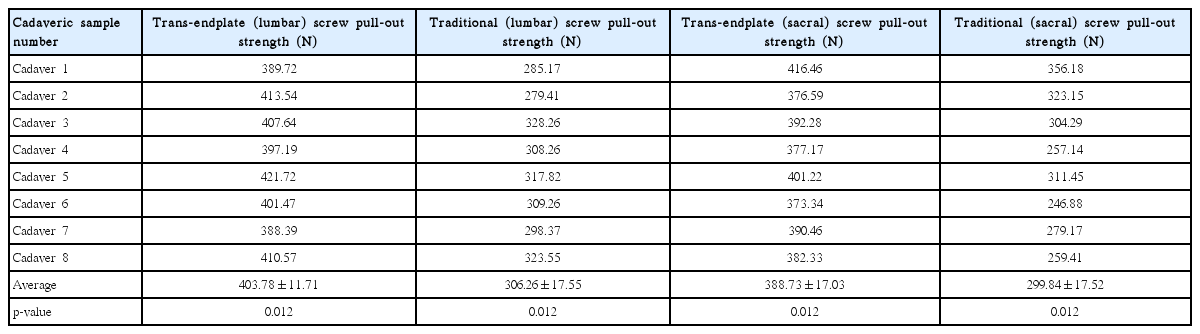
A comparison between the pullout strengths of lumbar and sacral traditional transpedicular screws and transendplate screws
A bar graph demonstrating the pull-out strength differences between different fixation techniques in L5 and S1 vertebrae.
DISCUSSION
Screw fixation in osteopenic bone remains a challenging issue for many spine surgeons3,12). The failure of lumbosacral fixation is usually a result of many well-known factors, some of which are, excessive stress on the lumbosacral area, the inappropriate direction of the screw insertion, the inadequate sacral bone reservoir and the pedicle fractures which may result due to the excessive over-loadings in the lumbosacral region4,7). The sacrum is known to have no true pedicles of cortical bone ring, but rather a confluence of cancellous bone from the first sacral segment vertebral body out to the sacra ala. Some limitations are encountered to overcome inserting screws into the sacral body, including the anteroposterior smaller diameter, the increase in the cancellous to cortical bone ratio, the very thinner anterior cortex and the close proximity of the anterior cortex to the major neurovascular vital structures22).
Improving the pull-out strength of the lumbosacral pedicle screw in osteoporotic vertebral bone is still a serious clinical challenge for many surgeons as demonstrated by a number of recent biomechanical studies conducted to develop new technologies to resolve this issue. Due to the increased aging spine population who require surgical intervention, improving bone-screw fixation is required due to the well-known history of complications like screw loosening, pull-out and implant failure in this group of patients10,18).
Zheng et al.23) showed that bone mineral density (BMD) of the S1 body was 31.9% more than the BMD of the sacra ala. He also demonstrated that BMD of the superior sacral endplate was higher than that of any other transverse layer near the lateral part of the S1 body. In addition, they have concluded that the anterolateral part of the upper S1 body was the densest area of the sacral trabecular intersection.
This biomechanical study was conducted to address the mechanical integrity of two different trajectory of the L5 lumbar and the S1 sacral screws under a uniaxial and toggle testing conditions. Although the static tests are commonplace in the literature19,23), however, future studies should be submitted to evaluate the dynamic properties of the new cortical fixation method.
We have used the trans-endplate lumbar and sacral fixation in many of our spine surgeries with clinical diagnosis of osteoporosis. We think that the end plate is a trustable place that would afford a very good screw grasp in osteoporotic bone, which we have repeatedly noticed during screw fixation due to the higher screw insertion torque strength experienced during application. These intraoperative recognitions are supported by the results of this in vitro biomechanical trial and it may be an important finding that my help surgeons to find a strong cortical bone screw purchase for a stable lumbosacral fixation specially in osteoporotic bone. Although feeling the insertion torque strength during insertion, permits the surgeon to judge the resistance of the inserted screw to pull-out forces. It is better to be careful not to protrude into the disc space as much as possible, rather than asserting that there is no risk of a vessel injury by screw protrusion to the disc space6,19,23).
However, like other biomechanical studies, this study has several limitations that should be noted. One limitation is that, all specimens were examined in a static uniaxial direction. The small number of the cadaveric samples involved in this experiment and the performance of the experiment on cadaveric samples not on true patients are also considered as limitations of this study. Further studies should be conducted in dynamic conditions with a large number of fresh cadaveric samples to yield a more detailed results.
CONCLUSION
The trans-endplate lumbosacral fixation method is a trustable safe fixation method with a stronger screw-bone purchase and can offer a good alternative for spine surgeons specially in patients with osteoporosis.
Notes
CONFLICTS OF INTEREST
The authors have no financial conflicts of interest.
INFORMED CONSENT
This type of study does not require informed consent.