Can Transradial Mechanical Thrombectomy Be an Alternative in Case of Impossible Transfemoral Approach for Mechanical Thrombectomy? A Single Center's Experience
Article information

Abstract
Objective
Until recently, the transfemoral approach (TFA) was used as the primary method of arterial approach in acute ischemic stroke (AIS). However, TFA resulted in longer reperfusion times and worse outcomes in the mechanical thrombectomy (MT) of patients with complex aortic arches and significant carotid tortuosity. We found that the transradial approach (TRA) is a more favorable alternative approach for MT in such cases.
Methods
We performed a retrospective review of our institutional database to identify 202 patients who underwent MT for AIS between February 2015 and December 2019. Patient characteristics, cause of TFA failure, procedure time, intra-procedural complications, and outcomes were recorded.
Results
Eleven (5.4%) of 202 patients, who underwent MT for AIS, crossed over to TRA for recanalization, and eight (72%) of 11 achieved successful recanalization (≥modified Treatment in Cerebral Infarction 2b). The mean age (mean±standard deviation [median]) was 82.3±6.6 (76) years, and five of the 11 patients were male. The last seen normal to puncture time was 467.9±264.72 (264) minutes; baseline National Institutes of Health Stroke Scale score was 28.9±14.5 (16). Six (55%) of the 11 patients had right vertebrobasilar occlusions, and the remaining five (45%) had anterior circulation occlusive disease. The time from groin puncture to final recanalization time (overall procedural time) was 78.0±20.1 (62) minutes. The mean crossover time from TFA to TRA was 45.2±10.5 (41) minutes. The mean time from radial puncture to final recanalization was 33.8±10.5 (28) minutes. Distal thrombus migration events in previously unaffected territories occurred in 3/8 patients (37%). At 90 days, three patients (28%) had a favorable clinical outcome.
Conclusion
Although rare, failure of TFA has been known to occur during MT for AIS. Our results demonstrate that TRA may be an alternative option for AIS intervention for select patients with subsequent timely revascularization. However, the incidence of distal thrombus migration was high, and the first puncture to reperfusion time was prolonged because of the time taken for the crossover to TRA after failure of TFA. This study provides some evidence that the TRA may be a viable alternative option to the TFA for MT of AIS.
INTRODUCTION
Over the last decade, multiple, large, randomized, controlled clinical trials have emphasized the importance of mechanical thrombectomy (MT) for the improvement of outcomes after acute ischemic stroke (AIS) [1,3,5-7,10,13,20]. According to these clinical trials, the conventional transfemoral approach (TFA) is the mainstay approach for MT because of its optimal catheter control, rare thrombotic complications, and immediate access to large-diameter devices [5,13]. Despite advances in technology, complex vascular anatomy may occasionally cause substantial delays in clot engagement in cases of MT performed via TFA. Further, TFA cannot be adopted when patients have extensive atherosclerotic disease in the aortic arch, anatomical variations in their aortic or brachiocephalic vessels, dissection of the thoracic aorta, or iliofemoral occlusive disease [1,5,11]. Although these difficulties posed by TFA in the MT of AIS are uncommon, they result in longer revascularization times and poor outcomes [19].
The findings of large, randomized clinical trials indicate that the transradial approach (TRA) has been used in the field of coronary intervention because of lower complication rates, lower cost, and early mobilization of patients compared with TFA [12]. In the field of neurointerventional procedures, including MT, the small sheath size of TRA does limit the ability to use larger catheters, such as proximal balloon guide catheters, and tri-axial systems in cases that may require advanced catheter support [2,13]. Hence, TRA has not been extensively adopted in the neuroendovascular field. However, in emergencies such as AIS, the ability to gain vascular access and optimize the delivery of thrombectomy devices to the face of the clot is of paramount importance. Therefore, several studies have recently compared TRA and TFA in patients undergoing MT and have demonstrated advantages of TRA such as navigation of tortuous aortic arches and carotid vasculature, similar puncture-to-reperfusion times, and successful revascularization rates compared with TFA [8,11,20].
Hence, we postulated that TRA could be an alternative option when TFA may be difficult, especially in patients with tortuous aortic arches and carotid vasculature. In our series, these complex vascular anomalies made MT prohibitively difficult in up to 5.4% of patients with AIS when TFA was adopted. Here, we report our recent experience with MT via TRA, which served as an alternative approach in those patients.
MATERIALS AND METHODS
This retrospective study was approved by the Institutional Review Board of Kangwon National University (IRB No. 2020-08-003). We retrospectively analyzed the institutional neurointerventional database that included consecutive patients undergoing attempted MT for AIS. Patients in whom TRA was used to approach the large vessel occlusion were included, when TRA was used owing to failure or difficulty in performing the TFA. Demographic and radiologic causes of crossover from TFA to TRA, procedural features, procedurerelated complication, and radiologic and clinical outcomes were recorded.
Indication for MT
The guidelines of the American Heart Association/American Stroke Association have provided class I support for the use of MT for the following indications : 1) internal carotid artery (ICA)/middle cerebral artery M1 occlusions, treatment within <6 hours, National Institutes of Health Stroke Scale (NIHSS) score of ≥6, Alberta Stroke Program Early Computed Tomography score of ≥6, and minimal premorbid disability with a modified Rankin Scale (mRS) score of 0–1 and 2) large-vessel occlusion in the anterior circulation, symptom onset 6–16 hours, and meeting the DAWN (diffusion weighted imaging or computed tomography perfusion assessment with clinical mismatch in the triage of wake-up and late presenting strokes undergoing neurointervention with Trevo) and endovascular therapy following imaging evaluation for ischemic stroke-3 trials [20]. In case of a large-vessel occlusion in the posterior circulation, nonenhanced CT was performed, followed by either a computed tomography angiography (CTA) or cerebral magnetic resonance imaging with magnetic resonance angiography (MRA), to confirm the presence of posterior circulation occlusion and to exclude both large brainstem infarction and intracranial bleeding. Our institution used no upper age or NIHSS score limit when selecting patients for MT. Our institution considered treatment of patients with up to 24 hours of stroke onset.
Transfemoral and TRAs
TFA was the first approach in all MTs. The patient was under conscious sedation in supine position on the angiography table, and the right arm was prepared in the supine position [2,6]. As a rule, a 9 F guide sheath was placed in the femoral artery. For crossover to TRA, the right wrist and both groins were prepped and draped. A coaxial or triaxial system, consisting of a long diagnostic catheter and guidewire placed inside a 9 F balloon guide catheter (Cello, Medtronic, Minneapolis, MN, USA) Optimo (Tokai Medical Products, Aichi, Japan), was advanced into the target carotid artery. The 5 F diagnostic catheter was removed, and a microcatheter with a microwire was introduced through the balloon guide catheter and navigated across the thrombus. The stent-retriever device was deployed in a standard fashion and withdrawn after 3–15 minutes with temporary blockage of f low by inf lation of the balloon and manual aspiration during stent retrieval. In cases of mechanical aspiration with stent retrieval, a triaxial system, consisting of a microsystem navigated through an intermediate catheter (ACE reperfusion catheter; Penumbra, Alameda, CA, USA), was placed at the clot face and turned on just before unsheathing the stent retriever. The stent retriever was deployed for 3–15 minutes and removed under constant aspiration. When the patient crossed over to TRA, a modified Allen test was performed prior to puncture by using pulse oximetry on the thumb followed by compression of both ulnar and radial arteries until the waveform disappeared. After the ulnar artery was released, the patient was considered to have passed the test if there was normalization of waveforms within 10 seconds. A micropuncture kit (20 G) was used for puncture. The puncture site was usually just proximal to the styloid process of the radius bone, and the puncture was followed by the insertion of a microdilator with a small incision. After access was achieved, a 6 French short sheath (Cook Medical, Bloomington, Indianapolis, IN, USA) was placed in the radial artery, and a spasmolytic ‘radial cocktail’ consisting of 5 mg of nicardipine and 200 µg of nitroglycerin was injected intra-arterially through the sheath. All patients had a short sheath with a distal access catheter (Envoy DA; Codman Neuro, Raynham, MA, USA), and a 0.038 guidewire (Terumo Interventional Systems, Somerset, NJ, USA) was advanced to approximately the level of the brachial artery. A Simmons 2 Selection catheter (Merit Medical, South Jordan, UT, USA) telescoping inside the 6 F distal access catheter was introduced into the radial artery all the way to the brachial artery to catheterize the appropriate common carotid artery. We used a 5 F Davis catheter (Cook Medical) if the right vertebral artery (VA) had been selected. A roadmap from this location enabled the wire, selection catheter, and the distal access catheter to be advanced into the ICA or VA. The MT was performed with a range of devices including a Solitaire stent-retriever (Medtronic), Aspiration System (Medtronic), Penumbra System (Penumbra), and Embolus Retriever with Interlinked Cages (ERIC; MicroVention, Tustin, CA, USA). In all cases, an arterial compression device was used for puncture site hemostasis (TR Band; Terumo Interventional Systems).
Outcome measures
We assessed procedure-related parameters such as the last seen normal to groin puncture time, overall procedural time (groin puncture to final recanalization), the mean crossover time from TFA to TRA, the mean time from radial puncture to final recanalization, recanalization grade (Thrombolysis in Cerebral Infarction [TICI] score), occurrence of distal thrombus migration (e.g., distal thrombus migration events in previously unaffected territories), procedure-related complications (e.g., puncture site, vessel dissection or perforation, symptomatic intracerebral hemorrhage, dissection). The functional outcome was defined as mRS at 3 months. The modified TICI (mTICI) scale was used for reperfusion grading. Recanalization was defined as being “successful” if mTICI was 2b/3. The functional outcome at 3 months was considered “favorable” if mRS ≤2 (independent). The results are shown as mean±standard deviation (median).
RESULTS
Patient
This study included 202 patients (Table 1). The mean age was 82.3±6.6 (76) years, and five of the 11 patients were male. The baseline NIHSS score was 28.9±14.5 (16). The most common location of occlusion was the six right vertebrobasilar occlusions (55.0%) followed by two left M1 (18.0%), two right M1 (18.0%), and one left M2 segment (9.0%). Three (33.0%) of 11 paitent received intravenous tissue-type plasminogen activator (IV tPA).
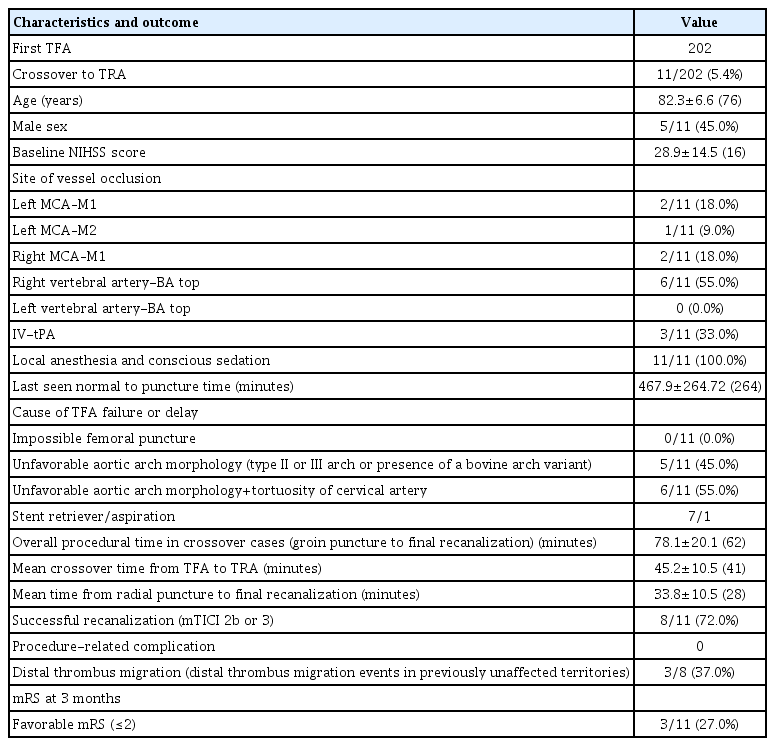
Baseline characteristics and summary of technical and clinical outcomes
MT
The TFA was used as the first route in all MTs (202 patients) for AIS without failure of femoral puncture. Eleven (5.4%) of 202 patients were underwent MT for AIS crossed over to TRA for recanalization. The last seen normal to puncture time was 467.9±264.72 (264) minutes. The mean time from groin puncture to final recanalization time (overall procedural time) was 78.0±20.1 (62) minutes. In 11 patients in whom the target artery access through the TFA was delayed or failed, five (45%) had an unfavorable aortic arch morphology, such as type II or type III arch or a presence of a bovine arch variant (Fig. 1) and six (55%) had a tortuosity of cervical artery (common carotid artery [CCA], ICA, and VA) with unfavorable aortic arch morphology (Fig. 2). The overall procedural time in crossover cases (groin puncture to final recanalization) was 78.1±20.1 (62) minutes. The mean crossover time from TFA to TRA was 45.2±10.5 (41) minutes. The mean time from radial puncture to final recanalization was 33.8±10.5 (28) minutes. A stent retriever was used in 7/8, and thromboaspiration was performed in 1/8 patients.

An 83-year-old female with National Institutes of Health Stroke Scale 21. A : Magnetic resonance angiography showed the occlusion of basilar artery top (white arrow) with aortic arch “type III” and unfavorable right vertebral artery origin angle. B : Right subclavian artery anteroposterior (AP) angiography from transfemoral approach showed that guiding catheter could not advance to the target artery. C : Right subclavian artery AP from transradial aporoach via guiding catheter. D and E : A Solitaire stent retriever (4×30) was deployed and achieved modified Thrombolysis in Cerebral Infarction score 3 recanalization with a single pass. Her functional outcome was favorable (modified Rankin Scale 1) at 3 months.
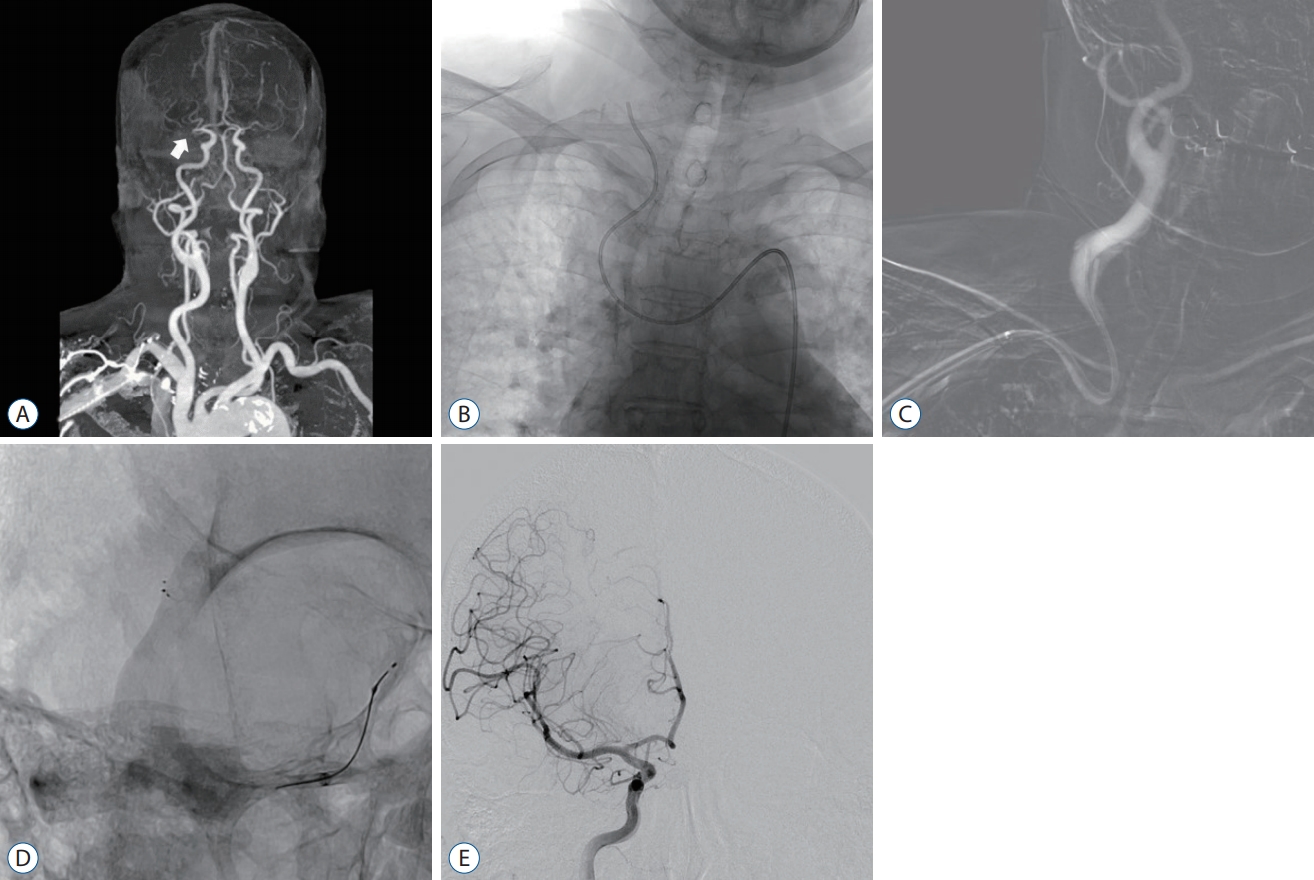
An 80-year-old female with National Institutes of Health Stroke Scale 14. A : Computer tomographic angiography showed the occlusion of the right middle cerebral artery (MCA), M1 (white arrow) with aortic arch “type III” and severe tortuosity of the common and internal carotid artery. B : Unsubtracted anteroposterior (AP) angiography via transfemoral approach; the guiding catheter could not advance to the target artery. C : Right subclavian artery AP roadmap via the transradial approach via guiding catheter. D and E : A Solitaire stent retriever (5×30) was deployed and achieved complete recanalization of MCA with multiple passes. However, a migrated thrombus was seen in the right distal anterior cerebral artery (dACA). We did not perform mechanical thrombectomy for the distal thrombus migration on the right dACA. Her functional outcome was favorable (modified Rankin Scale 2) at 3 months.
Technical and clinical outcomes
The rate of successful recanalization (mTICI 2b or 3 reperfusion) via TRA was 72% (8/11). In three unsuccessful cases (≤mTICI 2a), one patient received balloon angioplasty for a proximal stenosis of proximal ICA, a guiding system was not able to advance past the stenosis, and the access to the left CCA was not possible via first TFA and secondary TRA in the other two patients with unfavorable anatomy (type III aortic arch with a bovine arch and looping of cervical arteries). No procedure-related complications were noted. Distal migrated thrombus events in previously unaffected territories occurred in 3/8 (27%). At 90 days, three patients (27%) had a favorable clinical outcome, and five (45%) died. Of five died cases, three patients who obtained successful recanalization for posterior circulation occlusion died by other medical problems (septic condition and cardiac problem).
DISCUSSION
The use of TRA in coronary angiography was described in the 1980s [10,12]. The advantages of TRA include a lower risk of puncture site complications, post-procedural immobilization, and puncture site discomfort. Furthermore, the superficial location of the distal radial artery provides the advantage of easy positioning, rapid approach, and compression after sheath removal [11,12,17]. The use of TRA in the field of interventional neurosurgery has been described since the 2000s, with a few studies mainly focused on the treatment of intracranial lesions such as aneurysms and atherosclerotic disease [2,9,17,18]. Despite the advantages and feasibility, an important limitation of TRA for MT is the smaller size of the distal radial artery compared with that of the femoral artery, which prevents operators from using catheters larger than 8 F in most cases. This is especially a disadvantage for MT as it may require large-profile aspiration catheters or balloon guided catheters [6,15]. However, several studies have reported that elongated and tortuous vessels (aortic arch and craniocervical arteries) were associated with increased technical difficulty and consequently prolonged procedural times, lower recanalization rates, and poorer outcomes [2,12,14,18-20]. If catheter access through TFA appears difficult or impossible, an alternative approach, an alternative approaches need to be considered. We thought that the TRA may be better than the other approach (trans-brachial, trans-carotid approach) for MT. The reasons were as follows. First, the superficial and distal location of the radial artery confers the benefit of easy positioning, rapid crossover (switching to TRA) and reliable hemostasis. Second, especially in patients with type II or type III aortic arch configuration with bovine arch, catheterization by a Simmons-shaped catheter through TRA provided the ability to catheterize all brachiocephalic arteries. Particularly, direct access of the right VA via right TRA could be achieved by using an angled DAVIS catheter whereas it may be very challenging via TFA.
Therefore, we hypothesized that TRA might facilitate a successful reperfusion and favorable clinical outcome in such cases.
Recent studies have examined the safety and efficacy of MT for AIS. Chen et al. [5] studied 51 patients, 18 of which underwent MT via TRA and the remaining 33 via TFA, and found that there was no significant difference in operative times, periprocedural complications, or clinical outcomes between the two groups. Haussen et al. [9] reported that TRA was attempted in 15 of 1001 patients : it was used in 12 cases due to TFA failure and in three as the primary strategy, and nine of these 12 patients had successful recanalization without radial puncture site complications. Additionally, Almallouhi et al. [1] reported that of a total of 2203 patients who underwent a wide range of neurointerventions via TRA, 1697 patients (77%) underwent diagnostic procedures, and 506 (23%) underwent interventional procedures. Successfully completed procedures included aneurysm coiling (n=97), flow diversion (n=89), stent-assisted coiling (n=57), balloon-assisted coiling (n=19), and stroke thrombectomy (n=76). There were no major complications related to the radial access site. These results show that TRA has a high rate of procedural success (95%) with low complication rates (2%).
In our study of 202 patients who underwent MT for AIS, 11 patients (5.4%) crossed over due to complex aortic arch anatomy and tortuosity of cervical arteries because of the difficulty of guiding catheter delivery to the target carotid artery via TFA and a delay of more than 41 minutes.
The timing of switching from the TFA to the TRA was vague and difficult. Like many other interventionists, we had attempted many device and techniques (various kinds of angled 5 F catheters such as the Simmons and Vitek catheters, shapeable guidewire, co- or tri-axial system, etc.) In our study, it took about 70 minutes for the first two cases to be switched to the TRA. However, we grew in experience for these cases and found out the importance of a quick decision for a switching from the TFA to the TRA. Thus, decisions must be made early by observing the behavior of the guidewire and catheter and anatomical feature (difficult aortic arch morphology and cervical artery anatomy) from initial image (CTA or MRA).
According to previous studies, more than a 30-minute delay in guiding catheter delivery to the target artery may lead to lower rates of recanalization [19,21]. Also, we have typically used the combined technique (proximal balloon occlusion and distal aspiration) for MT using a stent retriever to prevent a distal migrated thrombus. Within 30–40 minutes, we tried to deliver large-profile aspiration catheters or balloon guided catheters through TFA. Especially in our 11 patients with elongated aortic arch, severe tortuosity of target arteries, or bovine configuration of the arch, we decided that time is more important than to prevent a distal migrated thrombus; hence, our choice was prompt crossover to TRA for a more favorable trajectory for rapid access to the target arteries.
Our results show that the rate of successful recanalization (mTICI 2b or 3 reperfusion) was 72% (8/11). In contrast, the results of multiple, large, randomized, controlled clinical trials indicate that successful recanalization (mTICI 2b or 3 reperfusion) was achieved in only ~60% of patients [3,21]. However, in our study, three patients (27%) had a favorable clinical outcome at 90 days. Moreover, our overall procedure time (groin puncture to final recanalization, median : 62 minutes) took longer than the 30–40 minutes reported by multiple, large, randomized, controlled clinical trials that used a primary TFA [6,7,16]. As the overall procedure time was high, the clinical outcomes would probably be poor. However, our favorable result was a consequence of a crossover to TRA and suggests that TRA could be recommended as a first-line intervention for patients with complex arches or significant cervical artery tortuosity noted on initial stroke evaluation CT angiography. However, the use of 8-Fr- or 9-Fr balloon guide catheters in TRA can be difficult because of the smaller caliber of the radial artery compared with that of the femoral artery. In our study, three distal thrombus migration events in previously unaffected territories had occurred in successful recanalization cases (3/8, 27%). In using TRA as a first-line approach, our concern was the limitation of catheter and device selection. A 6 F guiding system must be used during TRA, which limits the use of larger balloon guide catheters and has been shown to be ineffective for reducing the risk of distal thrombus migration. Furthermore, there are no smaller systems designed specifically for navigating the craniocervical vessels via TRA [4,17]. We predict that good results may be obtained regardless of whether TRA is a first- or second-line intervention if balloon guides are used for MT, and flow arrest is achieved.
This study has several limitations : first, it is a retrospective analysis, and second, it only analyzed a small number of patients. Third, as our study employed only one operator, the rates of TFA failure may have depended on the skill and procedural knowledge of this operator. We speculate that there may be a relatively higher rate of TFA failure and delay of overall procedure time if TFA is performed by clinicians who are in the early stages of learning the procedure. Fourth, while none of the patients had any clinically significant symptomatic access complications, and screening for asymptomatic procedure-related complications, such as radial artery occlusions, was not routinely performed. Fifth, mortality rate is relatively high in our cases (5 of 11). The contributing factors (such as time parameter or other factors) for high mortality should have been evaluated by statistical analysis. However, very small number of patients precluded a statistical analysis.
Prospective randomized studies with larger sample sizes are needed for objective assessment of the benefits of TRA over traditional TFA.
CONCLUSION
Although difficult or impossible catheter access to the target vessel during MT of AIS is not commonly observed in the TFA, it may result in longer reperfusion times and worse outcomes. Our results show that using the TRA as an alternative approach resulted in a high rate of successful recanalization with low complication rates. This study provides some evidence that the TRA may be a viable alternative option to the TFA for MT of AIS.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
INFORMED CONSENT
This type of study does not require informed consent.
AUTHOR CONTRIBUTIONS
Conceptualization : HWC, HSJ
Data curation : HWC, HSJ
Formal analysis : HWC, HSJ
Funding acquisition : HWC, HSJ
Methodology : HWC, HSJ
Project administration : HWC, HSJ
Visualization : HWC, HSJ
Writing - original draft : HWC, HSJ
Writing - review & editing : HWC, HSJ