A Nationwide Study on the Impact of COVID-19 Pandemic on Volume of Spine Surgery in South Korea
Article information

Abstract
Objective
In March 2020, World Health Organization declared a global pandemic caused by a novel coronavirus (SARS-CoV-2). The disease caused by this virus is called COVID-19. Due to its high contagiousness, many changes have occurred in overall areas of our daily life including hospital use by patients. The aim of this study was to investigate the impact of COVID-19 on volume of spine surgery in South Korea using the National Health Insurance database and compare it with the volume of a homologous period before the pandemic.
Methods
Data of related to spine surgery from January 2019 to April 2021 were obtained from the National Health Insurance and Health Insurance Review and Assessment Service database. Primary outcomes were total number of patients, rate of patients per 100000 population, and total number of procedures. The number of patients by hospital size was also analyzed.
Results
COVID-19 outbreaks occurred in South Korea in March, August, and December of 2020. Compared to the previous year, the total number of patients who underwent spinal surgery showed a decrease for 2–3 months after the first and second outbreaks. However, it showed an increasing trend after the third outbreak. The same pattern was observed in terms of the ratio of the number of patients per 100000 population. Between 2019 and 2021, the mean number of spine surgeries per month tended to increase. Mean annual medical expenses increased over the years (p=0.001). When the number of spine surgeries was analyzed by hospital size, proportion of tertiary general hospital in 2021 increased compared to those in 2019 and 2020 (vs. 2019, p=0.012; vs. 2020, p=0.016). The proportion of general hospital was significantly decreased in 2020 compared to that in 2019 (p=0.037).
Conclusion
After the COVID-19 outbreak, patients tended to postpone spinal surgery temporarily. The number of spinal surgeries decreased for 2–3 months after the first and second outbreaks. However, as the ability to respond to the COVID-19 pandemic at the hospital and society-wide level gradually increased, the number of spine surgeries did not decrease after the third outbreak in December 2020. In addition, the annual number of spine surgeries continued to increase. However, it should be noted that patients tend to be increasingly concentrated in tertiary hospitals for spinal surgery.
INTRODUCTION
Many infectious diseases have occurred with a great impact on human life. In the modern society, a large-scale epidemic has a great impact on the overall national society beyond the health care sector [8]. For example, the SARS (severe acute respiratory syndrome) epidemic in 2003 and the MERS (Middle East respiratory syndrome) epidemic in 2015 affected the world including South Korea [7]. In November 2019, a suspected case of bat-to-human transmission was reported in Wuhan, China, followed by the declaration of a cluster pneumonia outbreak. In March 2020, World Health Organization (WHO) declared a global pandemic caused by novel coronavirus (SARS-CoV-2). The disease caused by this virus is named COVID-19 [31]. Although most COVID-19 patients complain of fever and/or myalgia with respiratory symptoms such as cough and dyspnea, many patients show mild or no symptom. In elderly patients and those with underlying diseases such as heart disease, lung disease, and diabetes, COVID-19 may progress to a severe disease. In younger patients, the disease is more likely to remain asymptomatic or mild. However, even asymptomatic patients can transmit the virus [3].
The fear of asymptomatic transmission of this virus has affected many aspects of our daily lives since the outbreak of the COVID-19 pandemic, one of which is hospital use by patients [16-18,22]. Spinal disease is one of the most common reasons patients visit hospitals in South Korea. Spine surgery is also one of the top 10 common surgeries performed in South Korea [10]. However, since the COVID-19 pandemic, patients tend to postpone hospital care or surgery unless it is an emergency or acute illness. This may affect the prognosis of patients with spinal disease. Revealing whether there is a change in spinal surgery due to COVID-19 is necessary to cope with another pandemic that may come in the future. Identifying changes in spine surgery following the COVID-19 pandemic could also help us effectively allocate medical resources. As far as we know, studies analyzing changes in the number of spine surgeries in South Korea based on data from the Health Insurance Review and Assessment Service (HIRA) and National Health Insurance database have not been reported yet. Thus, the purpose of this study was to investigate the impact of COVID-19 on the volume of spinal surgeries performed in South Korea and compare it with that in the same period before COVID-19 pandemic occurrence.
MATERIALS AND METHODS
Study population and data collection
All data were obtained from the National Health Insurance and the HIRA database. The data were constructed after anonymization according to confidentiality guidelines of HIRA. Since this study used anonymized public data, ethical approval was waived by the Institutional Review Board of Soonchunhyang University Seoul Hospital (2022-04-007). We obtained the number of total patients who underwent spine surgeries, the number of patients per 100000 population, the total number of spine surgeries, spinal patient medical expenses, and the number of spinal surgeries according to the size of the hospital in terms of the number of beds. Data from January 2019 to December 2019 were categorized into before COVID-19 pandemic occurrence group. Data from January 2020 to April 2021 were categorized into after COVID-19 group. All data are presented in actual data or as mean±standard deviation.
The primary outcome was the monthly volume of spine surgeries before and after the COVID-19 pandemic occurrence. Since there were three COVID-19 outbreaks before April 2021 in Korea, we evaluated the impact of each outbreak on the number of spine surgeries.
Statistical analysis
All statistical analyses were performed using SPSS software version 19.0 (SPSS Statistics/IBM Corp, Chicago, IL, USA). Continuous variables are expressed as mean and range. Categorical variables are expressed as frequencies. All statistical analyses comparing data were verified through analysis of variance (ANOVA). Chi square test was used to evaluate the difference in monthly volume. p-values below 0.05 were considered to be statistically significant. All continuous variables are presented as mean unless stated otherwise.
RESULTS
Number of patients who underwent spine surgeries
COVID-19 outbreak occurred in March, August, and December of 2020 in Korea. In March, April, and May of 2019, numbers of patients who underwent spinal surgeries were 14351, 14941, and 15408, respectively. During the same period after the first outbreak in March 2020, numbers of patients who underwent spine surgeries were 13453, 13587, and 14961, respectively, which were decreased by 94%, 91%, and 97%, respectively, compared to those in the same period of the previous year. However, in June of 2020, the number of patients who underwent spine surgery was 16774, an increase of 116% compared to 14441 in June of the previous year.
In July, August, and September of 2020, numbers of patients who underwent spinal surgeries were similar to those of the previous year : 16572, 15204, and 14296 in 2019 vs. 16800 (101% compared to the previous year), 15205 (100%), and 14211 (99%) in 2020, respectively. In October, Novermber, and December of 2020, numbers of patients who underwent spinal surgeries showed an increasing trend compared to those of the previous year : 14535, 14608, and 15678 in 2019 vs. 15847 (109%), 16256 (111%), and 16279 (104%) in 2020, respectively.
In January, February, March, and April of 2021, numbers of patients who underwent spinal surgeries continued to increase compared to those in the same month of the previous year : 16534 (103%), 13954 (103%), 17955 (133%), and 16521 (122%), respectively. These results are summarized in Table 1 and Fig. 1A. However, there was no statistically significant difference in the number of spine surgery patients during the same month by year (p=0.207). The same pattern was observed for the number of patients per 100000 population (p=0.89) as shown in Table 1.
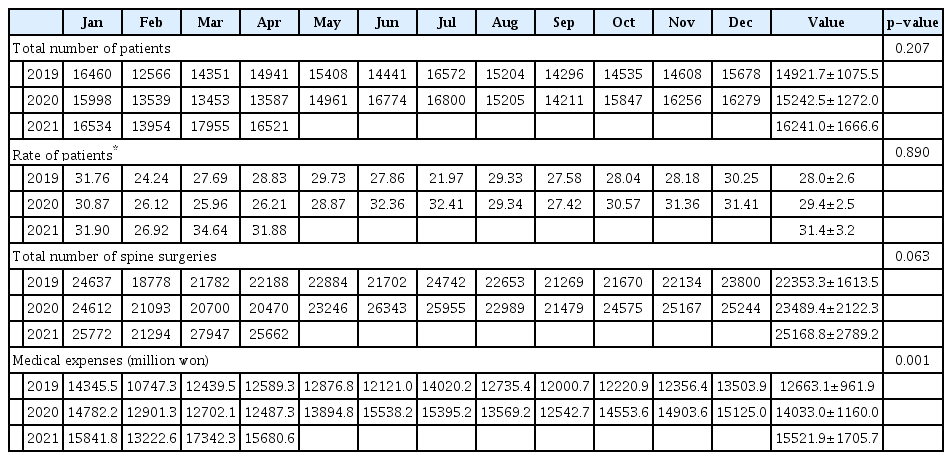
Total number of patients who underwent spine surgeries, rate of patients per 100000 population, total number of spine surgeries, and medical expenses related with spine surgery between 2019 and 2021

A : Total No. of patients who underwent spine surgery per month. B : Total No. of spine surgery per month. C : Medical expenses related to spine surgery per month (1000 won).
Number of spine surgeries
Mean number of spine surgeries per month for each year was 22353.25±1613.49 in 2019, 23489.42±2122.30 in 2020, and 25168.75±2789.24 in 2021. Although the mean number of spinal surgeries per month tended to increase by year, such increase was not statistically significant (p=0.063).
In March and April of 2020, when the first outbreak occurred, numbers of spinal surgeries were 20700 and 20470, respectively, which were decreased to 95% and 92% of those during the same month in 2019 (21787 and 22188, respectively). However, in May 2020, the number of spinal surgeries was 23246, which was 101% of 22884 cases in the same month of 2019. In June and July 2020, numbers of spine surgeries were 26343 and 25955, respectively, where were increased by 121% and 104% from 21702 and 24742 in the same months of 2019. After the second outbreak, in August and September 2020, numbers of spine surgeries were 22989 and 21479, respectively, which were similar (increase by about 101%) to 22653 and 21,269 in the same months of 2019. In October, November, and December of 2020, numbers of spine surgeries were 24575, 25167, and 25244, respectively, which were increased by 113%, 114%, and 106%, respectively, compared to 21670, 22134, and 23800 in the same months of the previous year.
Another outbreak occurred in December 2020. From January to April 2021, numbers of spine surgeries in these 4 months were 25772, 21294, 27947, and 25662, respectively. In February, the number remained the same (101%) as the number of the previous year. Numbers of cases in January (105%), March (135%), and April (125%) were all increased compared to those in the same months of the previous year. These results are summarized in Table 1 and Fig. 1B.
Trends of medical expenses
When medical expenses related to spinal surgeries were evaluated, they were similar to those of the previous year in April 2020. For the rest of the peiord, all were increased compared to those of the previous year. Overall mean annual medical expenses for spine surgeries were 12663.12±961.91 million won, 14032.97±1159.96 million won, 15521.87±1705.68 million won in 2019, 2020, and 2021, respectively, showing statistically significant (p=0.001) increases. Trends of medical expenses are shown in Table 1 and Fig. 1C.
Number of spine surgeries by hospital size
When the number of spine surgeries was analyzed by hospital size in 2019, overall mean number of spinal surgeries was 315.92±35.99 in clinic, 12058.83±900.32 in hospital, 6188±462.94 in general hospital, and 3790.67±328.23 in tertiary hospital. Mean percentages of cases performed in clinic, hospital, general hospital, and tertiary hospital were 1.41%, 53.95%, 27.68%, and 16.96%, respectively. These percentages in 2020 changed to 1.4%, 53.02%, 29.34%, and 16.24%, respectively. Compared to that of the previous year, the proportion of spine surgeries performed in general hospitals was increased from 27.68% to 29.34%, where as that performed in hospitals was decreased from 53.95% to 53.02% (p=0.037). In 2021, percentages of spine surgeries performed in clinic, hospital, general hospital, and tertiary hospital were 1.38%, 53.13%, 27.34%, and 18.15%, respectively. The proportion of spinal surgeries performed in tertiary hospitals was increased significantly from 16.96% in 2019 and 16.24% in 2020 to 18.15% in 2021 (p=0.012). These results are summarized in Table 2 and Fig. 2.
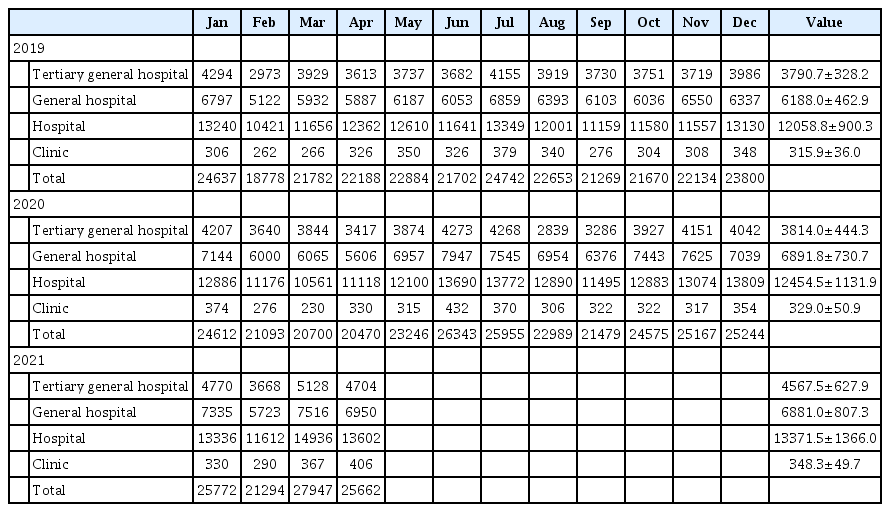
Number of spine surgeries by hospital size

Compared to 2019, the proportion of spinal surgery performed in general hospitals in 2020 increased from 27.68% (2019) to 29.34% (2020) (p=0.037). And compared to 2019 and 2020, the proportion of spinal surgery performed in tertiary hospital in 2021 increased from 16.96% (2019) and 16.24% (2020) to 18.15% (2021) (p=0.012).
DISCUSSION
Characteristics of COVID-19
SARS-CoV-2, the virus that causes COVID-19, is mainly transmitted through direct channels such as respiratory droplets or human contact through coughing or sneezing. Indirect transmission can also occur through contact with aerosolized particles or virus-contaminated surfaces remaining in the air [12,30]. The incubation period between exposure and symptom onset is usually between 3 and 5 days. It can take up to 14 days [12,13]. These transmissions can occur not only in symptomatic patients, but also in asymptomatic patients [3]. Patients infected with COVID-19 have symptoms of various spectrum. They mainly complain of symptoms of fever, cough, myalgia or fatigue, expectoration, and dyspnea. Minor symptoms include headache or dizziness, diarrhea, nausea, and vomiting [15]. In severe cases, it can lead to death. The mortality rate is about 5% [15]. It was reported that 58% of cases occurred in men and less than half of the infected had underlying diseases such as diabetes, high blood pressure, and cardiovascular disease [12]. COVID-19 is associated with a greater risk of serious morbidity and mortality in the old age group and those with comorbidities [12].
COVID-19 and spine surgery
The outbreak of COVID-19 should not just be viewed as a rapidly spreading upper respiratory infection, but a social phenomenon [9]. COVID-19 has had a great impact of society as a whole, especially on the medical community and medical profession [2,11,17-19,22,25]. The lack of ICU due to COVID-19 could affect the high-risk spine surgery. In addition, because many patients with spinal disorders are elderly with medical comorbidities, there is a high risk of progression to the severe COVID-19 stage [12]. However, it can be difficult to cope efficiently during the COVID-19 epidemic without proper guidelines. Therefore, some organizations including the American College of Surgeons, Unitied States Centers for Disease Control and Prevention, the Orthopedic Trauma Association, and the Royal College of Surgeons of England have suggested guidelines [1,4,21,23,24,27,29]. The French spine surgery society has prepared specific guidelines for spinal disease management in COVID-19 pandemic situations to help manage patients with emergency spinal disease [21]. The North American Spine Society has also presented a guideline for the triaging system for surgical treatment of spine patients [29]. There are also reports of information on how to set up in the operating room, how to do intubation/extubation, and how to transfer to the recovery room [12].
COVID-19 and management of patients with spinal diseases
In order to prevent the spread of COVID-19, social distancing has been emphasized worldwide, including South Korea. Also in the early days, there was a belief that the COVID-19 pandemic would soon be over if we endured social distancing for a while. This has led patients to delay surgical decisions. It has also affected the way doctors manage inpatients and outpatients. However, contrary to initial expectations, the COVID-19 pandemic is continuing for more than 2 years. Many patients with spinal disease no longer postpone active treatment, including surgery. Also, based on the concern that another pandemic may occur in the future, guidelines for treating patients with spinal diseases need to be prepared.
Even during a pandemic, spine surgeons should answer emergency patient calls, evaluate patients in a timely manner, and manage patients who are already hospitalized [12]. It may be good idea to divide medical staff into teams such as inpatient management, surgery, on-call, and outpatient service. They can alternate on a weekly basis without contacting each other if necessary in a pandemic situation [12]. At the peak of the pandemic, home treatment instead of hospitalization is recommended as much as possible for patients with vertebral compression fractures who complain of only back pain without neurological deficits. For patients who complain of uncontrolled radiating pain, choosing nerve root injection instead of surgery may be an option during a pandemic peak. By relocating patients in this way, appropriate anesthesia, nursing, and support before and after surgery are possible so that patients in need of emergency surgery could be treated [26].
In addition, depending on the doctor’s preference, telemedicine may be considered [20]. In a verification study performed at Neumarkt Clinic in Germany, neurological tests conducted remotely through audiovisual telemedicine presented results comparable to bedside examination [20]. Despite the controversy, telemedicine can be a useful alternative approach during a pandemic in that it can minimize the risk of diseae exposure for medical staff, while allowing patients to stay at home and comply with public health recommendations [12]. It can also be used for screening for COVID-19-related symptoms before face-to-face treatment [12].
COVID-19 and medical education/training program
On-tact education gradually replaces face to face education as the COVID-19 pandemic prolongs, there are many concerns that resident and fellowship training is not be conducted as before. Many trainees face uncertainty about their progress and the impact on their training [32]. Chang et al. [5] has published results of a survey of 229 residents. Their results showed that traditional teaching methods were reduced, while online-based teaching methods were increased. However, satisfaction with online-based teaching methods was lower than that with traditional methods.
Fortunately, as shown in the results of this study, the total number of spine surgeries in South Korea did not decrease, and it does not seem to affect the clinical experience of residents and fellows. However, many parts of conference and education program are changing from off-line to on-line, it is necessary to think about effective methods of education and training. There is a need to discuss about effective education and training method by appropriately combining the parts that have change and traditional methods.
COVID-19 and spine surgery in South Korea
The COVID-19 pandemic is affecting all aspects of our daily lives, including hospital visits. According to Lee et al. [14], neurosurgical emergency patients were analyzed, and the number of trauma and stroke paitents decreased as the overall activity decreased. In spine patients, Ham et al. [9] have analyzed the number of daily outpatients from 2017 to March 2020 and found that the number of daily outpatients is decreased significantly compared to that in the same month before the pandemic. And in Japan, the first COVID-19 semi-lockdown led to a decrease in elective surgeries and an increase in urgent surgeries [28]. However, their studies only included the period up to the beginning of the pandemic, so the trend after that is unknwon. In the present study, we analyzed the most recent data up to April 2021 published in HIRA and National Health Insurance up to the time of this study.
After the first and second outbreaks in March and August of 2020, the number of spine surgeries and patients who underwent spinal surgery decreased or stagnated for about 2 or 3 months. It then increased again. However, after the third outbreak in December 2020, the number of spine surgeries and patients did not decrease, but remained similar or increased. This means that, unlike at the time of the initial COVID-19 outbreak, an appropriate response system has been established in each hospital later. Patients' perceptions of COVID-19 have also changed.
In the case of France, the total number of spinal surgery in 2020 decreased by 13% compared to 2019 due to the pandemic [6]. Unlike France, despite a prolonged COVID-19 pandemic, the mean annual number of spine surgeries steadily increased between 2019 and 2021 in South Korea. This difference may be due to the influence of policy differences in countries responding to COVID-19. However, we found differences according to hospital size in the overall increase in the number of spine surgeries. In particular, there were statistically significant differences in the number of spine surgeries performed in tertiary hospital and general hospital. Compared to 2019, the proportion of surgeries performed in tertiary hospital in 2020 was decreased, although the decrease was not statistically significant (16.96% and 16.24%, respectively). However, the proportion of tertiary hospital in 2021 was increased compared to those in 2019 and 2020 (vs. 2019, p=0.012; vs. 2020, p=0.016). Patients' beliefs that tertiary hospitals could help them better cope with COVID-19 infections might have influenced this finding. The proportion of surgeries performed in general hospitals was significantly decreased from 2019 to 2020 (p=0.037). However, the fact that there was a large-scale strike by doctors in South Korea from August to September 2020, especially among residents, might have influenced the change in the number of these surgeries.
Despite the pandemic of COVID-19, medical expense continued to rise in 2020 and 2021 compared to that in 2019 (p=0.001). There was no significant difference in the medical expense between 2020 and 2021 (p=0.107). Due to the nature of this study design, only information on the total amount of medical expenses could be obtained, so detailed analysis for the medical cost could not be conducted. There might be changes in insurance standards or the prevalence of endoscopic surgery. Also, patients had to undergo repeat COVID-19 screening tests in the emergency clinic, before and during admission to the hospital. The cost for COVID-19 screening could also be one of the cause of increased medical expense.
The initial intention of our study was to determine whether the number of spine surgeries in the country did not decrease during the COVID-19 pandemic. Patients with non-emergency diseases such as degenerative spine disease were reluctant to visit the hospital due to concerns about in-hospital infection. Even doctors have sometimes postponed scheduled surgeries, with the hope that the COVID-19 pandemic will subside after a while. In addition, as and the available medical resources become scarce because of increasing of the number of COVID-19 patients, treatment for non-emergency diseases was delayed within hospitals. However, this study present that the total number of spine surgery did not decrease during the COVID-19 period. It should be noted more patients underwent spine surgery in higher-level hospital. This means that higher-level hospitals are more likely to deal with pandemic situations, and this may mean that patients have been treated with greater confidence. However, when another pandemic situation arises in the future, the concentration of patients to higher-level hospitals may lead to medical collapse, so it is meaningful to prepare for it in advance. Therefore, it may be necessary to prepare plan for the future.
Limitations
Since this was a retrospective study using HIRA and National Health Insurance data, there was a limitation in that it was difficult to analyze factors such as patient demographic data, diagnosis, medical expense details, and type of surgery, which might have affected our results. In comparison of the number of spine surgeries by hospital size from 2019 to 2020, all 12 months were included in 2019 and 2020, but only 4 months from January to April of data were included in 2021. Therefore caution is required in interpreting the results. In addition, there was a limitation in that there was no investigation into changes in patients’ perceptions or behaviors of in-hospital treatment that might affect patients’ visits to hospitals after the COVID-19 era. However, through this study, we can predict in advance how another pandemic will affect the medical community in the future. Further research is required for sustainable and safe treatment.
CONCLUSION
After the COVID-19 outbreak, patients tended to postpone spinal surgery temporarily. The number of spinal surgeries decreased for 2–3 months after the first and second outbreaks. However, as the ability to respond to the COVID-19 pandemic at hospital and society-wide levels gradually increased, the number of spine surgeries did not decrease even after the third outbreak in December 2020. In addition, the annual number of spine surgeries continued to increase. However, it should be noted that patients showed a tendency to focus on tertiary hospitals for spinal surgery.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Informed consent
This type of study does not require informed consent.
Author contributions
Conceptualization : MHL, HRP, JCC; Data curation : MHL, HRP; Formal analysis : MHL, HRP; Methodology : MHL, HRP; Project administration : MHL, HRP, JCC; Visualization : MHL, HRP; Writing - original draft : MHL, HRP; Writing - review & editing : MHL, HRP, JCC, HKP, GSL
Data sharing
None
Preprint
None
Acknowledgements
This research was supported by Soonchunhyang University Research Fund.