Role of Neurosurgeons in the Treatment of Acute Ischemic Stroke in the Emergency Room
Article information

Abstract
Objective
With the recent increase in mechanical thrombectomy (MT) for acute ischemic stroke (AIS), the role of neurosurgeons in AIS treatment has become increasingly important. This study aimed to assess the outcomes of patients with AIS treated by neurosurgeons and neurologists in the emergency room (ER) of a tertiary hospital in South Korea.
Methods
From January 2020 to June 2021, 536 patients with AIS within 24 hours of symptom onset were admitted to our hospital via the ER. Based on the type of doctors who provided initial care for AIS in the ER, patients were divided into two groups : (a) neurosurgeon group (n=119, 22.2%) and (b) neurologist group (n=417, 77.8%).
Results
Intravenous tissue plasminogen activator (tPA) was administered in 82 (15.3%) of 536 patients (n=17 [14.3%] in the neurosurgeon group and n=65 [15.6%] in the neurologist group). The door-to-tPA time was not significantly different between both groups (median, 53 minutes; interquartile range [IQR], 45–58 vs. median, 54 minutes; IQR, 46–74; p=0.372). MT was performed in 69 patients (12.9%) (n=25, 36.2% in the neurosurgeon group and n=44, 63.8% in the neurologist group). The neurosurgeon group achieved a shorter door-to-puncture time than the neurologist group (median, 115 minutes; IQR, 107–151 vs. median, 162 minutes; IQR, 117–189; p=0.049). Good clinical outcomes (3-month modified Rankin Scale 0–2) did not differ significantly between the two groups (96/119 [80.7%] vs. 322/417 [77.2%], p=0.454).
Conclusion
The neurosurgeon group showed similar door-to-treatment time and clinical outcomes to the neurologist group in patients with AIS in the ER. This study suggests that neurosurgeons have comparable abilities to care for patients with AIS in the ER.
INTRODUCTION
South Korea is aging rapidly, and the population aged 65 years and over will account for 30% in 2036 and 40% in 2050 [6]. As the elderly population is expected to increase in the future, the prevalence of stroke is also expected to increase [11]. Neurologists play an important role in the treatment of acute ischemic stroke (AIS) by administering recombinant tissue plasminogen activator (tPA). Recently, with the rapid development of neurointerventional procedures for the treatment of AIS, the role of neurosurgeons has become increasingly important [5,7,11].
The management of patients with AIS remains multidisciplinary [12]; however, neurologists are still mainly responsible for AIS care. Recently, the issue of the manpower shortage in neurology departments has been raised owing to the overwork of neurology residents [9]. A previous study reported an increased number of patients with AIS per neurology resident and an increased number of duty days per resident [9]. These issues could have resulted from a decreased number of neurology residents and an increased number of patients with AIS.
There are no exact data or reports on how many hospitals are not always available (24/7) for AIS care in South Korea. However, some hospitals are not available 24/7 for AIS care because of the shortage of neurologists [7], which was the case at our hospital. Due to the absence of neurology residents in our hospital, our neurologists experienced burnout and were frequently replaced. As a result, 24/7 AIS care units are no longer available at our hospital. As 24/7 AIS care became unavailable, not only patients with ischemic stroke but also those with hemorrhagic stroke no longer came to our hospital, and the total number of patients with cerebrovascular disease decreased.
To overcome this problem, cooperation between neurosurgeons and neurologists was needed, and neurosurgeons decided to take charge of AIS care. However, neurosurgery residents do not want to work for AIS care because of the increased workload and the fact that AIS care in the emergency room (ER) is generally not the job of neurosurgeons. Consequently, since January 2020, cerebrovascular neurosurgeons have decided to provide AIS care in the ER, and neurosurgeons and neurologists have taken turns providing AIS care.
Recently, similar to our hospital, some patients with AIS have been treated by neurosurgeons at the ER in South Korea. However, there is no exact data or reports on this topic. This study aimed to assess the outcomes of patients with AIS treated by neurosurgeons and neurologists in the ER at our institute.
MATERIALS AND METHODS
The present study protocol was reviewed and approved by the Instituional Review Board of Samsung Changwon Hospital (SCMC2022-04-020).
Patient population
The study period was from January 2020 to June 2021. We reviewed the data of patients with AIS admitted to our hospital via the ER. The inclusion criteria were as follows : 1) patients with symptomatic stroke, 2) cerebral infarction or transient ischemic attack were confirmed using diffusion-weighted imaging (DWI), and 3) patients admitted to the neurosurgery or neurology department. The exclusion criteria were as follows : 1) patients with hemorrhagic stroke and 2) >24 hours from symptom onset to the ER. Fig. 1 illustrates the case accrual process.
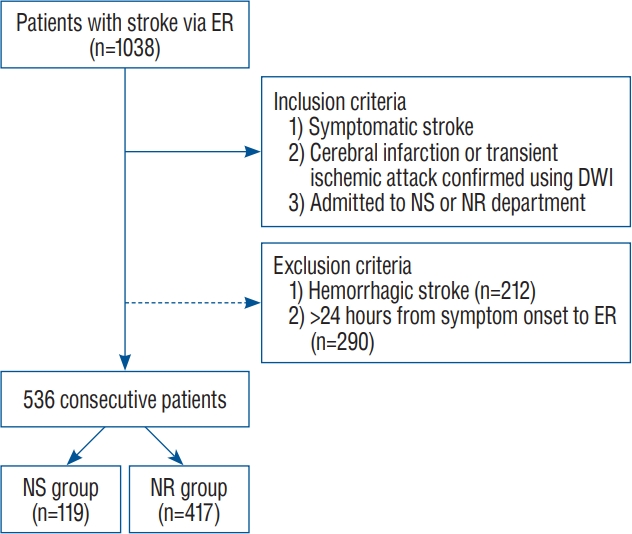
The case accrual process. ER : emergency room, DWI : diffusion-weighted imaging, NS : neurosurgery, NR : neurology.
Data collection and patient characteristics
Medical records, including age, sex, medical history (e.g., hypertension and diabetes mellitus), time from symptom onset to ER, National Institutes of Health Stroke Scale (NIHSS) score on admission, type of doctor who took care of the patient in the ER, use of intravenous tPA, time from door-to-tPA, use of mechanical thrombectomy (MT), time from door-to-puncture, stroke unit admission, and clinical outcomes were reviewed retrospectively.
The NIHSS score of each patient was assessed on admission. Patients were divided into two groups based on the type of the doctor who provided AIS care in the ER : (a) the neurosurgeon group and (b) the neurologist group. Variable factors such as intravenous tPA and MT were assessed between the two groups. Patients admitted within 4.5 hours of symptom onset were considered suitable candidates for intravenous tPA. Clinical outcomes were assessed using the 3-month modified Rankin Scale (mRS) score and mortality. Based on mRS scores, outcomes were defined as good (0–2) and poor (3–6).
Stroke care system in our hospital
During the study period, there were seven to nine stroke physicians in our hospital, consisting of four to six neurologists and three neurosurgeons. Stroke physicians took turns providing AIS care. When patients with suspected stroke visited the ER, ER physicians would call the stroke physician on duty, and the stroke physician would attend to the patient with suspected stroke in the ER. Imaging studies included brain computed tomography and stroke magnetic resonance imaging (MRI) examinations. Stroke MRI included magnetic resonance angiography, DWI, and perfusion imaging.
There were four neurointerventionalists in our hospital, consisting of three neurosurgeons and one neurologist. When cerebral large artery occlusion was observed and MT was planned, MTs were performed by one of three neurosurgeons, except for patients cared for by a neurointerventionalist-neurologist. After MT, patients were admitted to the stroke doctor's department who cared for the patient in the ER.
Statistical analysis
The variables were compared between the neurosurgeon and neurologist groups. Variables were also compared between patients with good and poor clinical outcomes. Patients with intravenous tPA and those with MT were compared between the neurosurgeon and neurologist groups, respectively.
Categorical variables were analyzed using the chi-square test or Fisher’s exact test. Continuous variables were analyzed using Student’s t-test or Mann-Whitney U test. Statistical significance was set at p<0.05. Multivariable logistic regression analysis was used to evaluate the factors associated with good clinical outcomes. Variables with a p-value <0.20 in the univariate analysis were included in the logistic regression analysis. All statistical analyses were performed using SPSS version 22 (IBM Corp., Armonk, NY, USA).
RESULTS
A total of 1038 patients were included in this study. Of these patients, 502 were excluded for the following reasons : 1) patients with hemorrhagic stroke (n=212) and 2) >24 hours from symptom onset to ER (n=290). Finally, 536 consecutive patients were included in this study. Of these, 324 patients (60.4%) were men. The mean patient age was 68.7 years (range, 26–96). Neurosurgeons treated 119 patients (22.2%) with AIS and neurologists treated 417 patients (77.8%) with AIS.
Fig. 2 shows the NIHSS scores on admission for all patients in the neurosurgeon and neurologist groups. The severity of AIS was mild in most patients. Among all patients, 341 (63.6%) had an NIHSS score of 0–4. Fig. 3 shows the 3-month mRS scores for all patients, as well as those in the neurosurgeon and neurologist groups. The clinical outcome of patients with AIS was good in the majority of patients. Overall, 418 patients (78.0%) had a 3-month mRS score of 0–2. Medical treatment only was given to 416 patients (77.6%), intravenous tPA to 82 patients (15.3%), MT to 69 patients (12.9%), and both intravenous tPA and MT to 31 patients (5.8%) (Fig. 4).
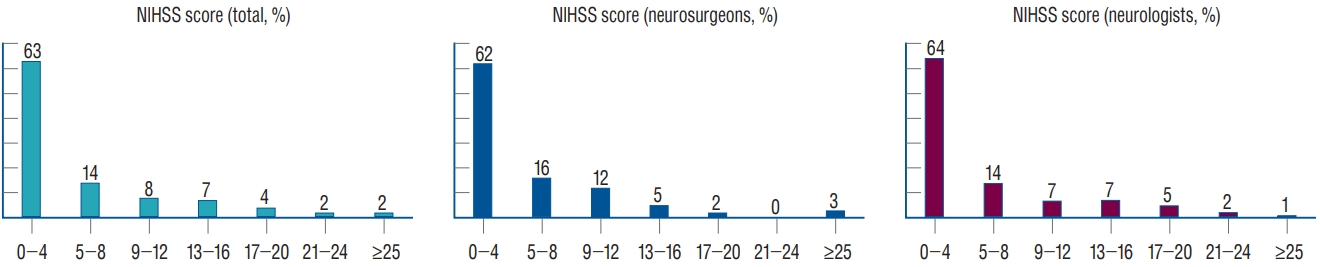
National Institute of Health Stroke Scale (NIHSS) scores on admission for all patients, neurosurgeon group, and neurologist group.
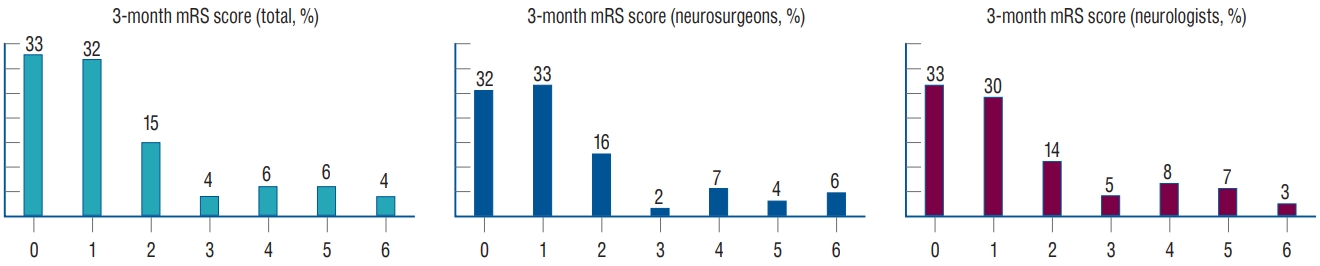
Three-month modified Rankin Scale (mRS) scores for all patients, neurosurgeon group, and neurologist group.
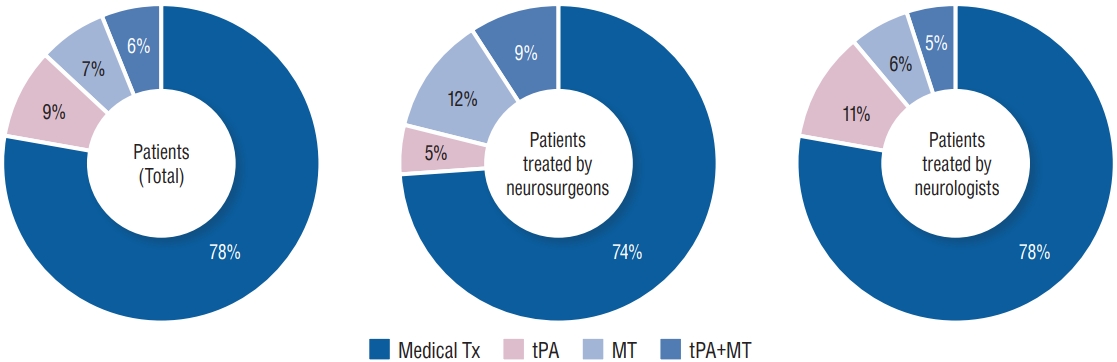
Treatment types for all patients, neurosurgeon group, and neurologist group. Tx : treatment, tPA : tissue plasminogen activator, MT : mechanical thrombectomy.
A comparison of the patients with AIS treated by neurosurgeons and neurologists is presented in Table 1. The rate of intravenous tPA administration was not significantly different between the two groups (17/119 [14.3%] vs. 65/417 [15.6%], p=0.775). Furthermore, MT was performed more frequently by neurosurgeons than neurologists (25/119 [21.0%] vs. 44/417 [10.6%], p=0.005). Good clinical outcomes were not significantly different between the two groups (96/119 [80.7%] vs. 322/417 [77.2%], p=0.454). The mortality was also not significantly different between the two groups (7/119 [5.9%] vs. 14/417 [3.4%], p=0.280).
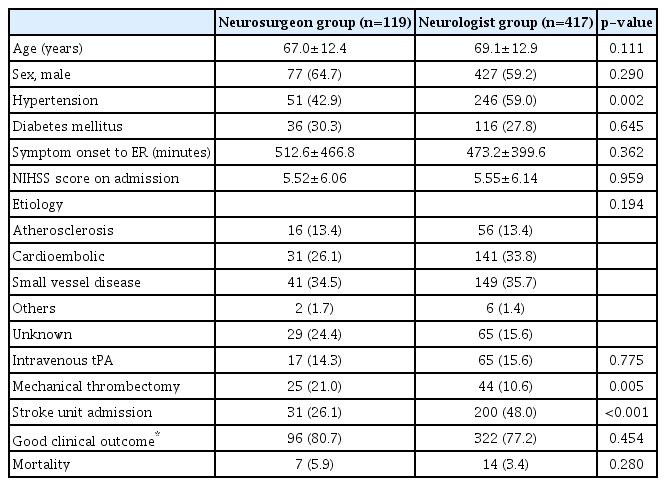
A comparison of patients with acute ischemic stroke treated by neurosurgeons and by neurologists
Table 2 shows the comparison between patients with good clinical outcomes and those with poor clinical outcomes. Patients with good clinical outcomes were significantly younger than those with poor clinical outcomes (67.0±12.8 vs. 74.6±11.0 years, p<0.001). Patients with good clinical outcomes were more likely to be men than those with poor clinical outcomes (269/416 [64.4%] vs. 55/118 [46.6%], p=0.001). The time from symptom onset to ER was significantly longer in patients with good clinical outcomes than in those with poor clinical outcomes (502.1±428.3 vs. 410.2±357.9 minutes, p=0.034). The NIHSS score on admission was significantly lower in patients with good clinical outcomes than in those with poor clinical outcomes (3.31±3.51 vs. 13.5±6.75, p<0.001). Regarding the etiology, patients with good clinical outcomes had a higher rate of small vessel disease than those with poor clinical outcomes (183/416 [44.0%] vs. 7/120 [5.8%], p<0.001). Patients with good clinical outcomes had a lower use of intravenous tPA and MT than those with poor clinical outcomes (57/416 [13.6%] vs. 25/118 [21.2%], p=0.005, 30/416 [7.2%] vs. 39/118 [33.1%], p<0.001). The rate of stroke unit admission was significantly higher in patients with good clinical outcomes than in those with poor clinical outcomes (197/416 [47.1%] vs. 34/118 [28.8%], p<0.001).
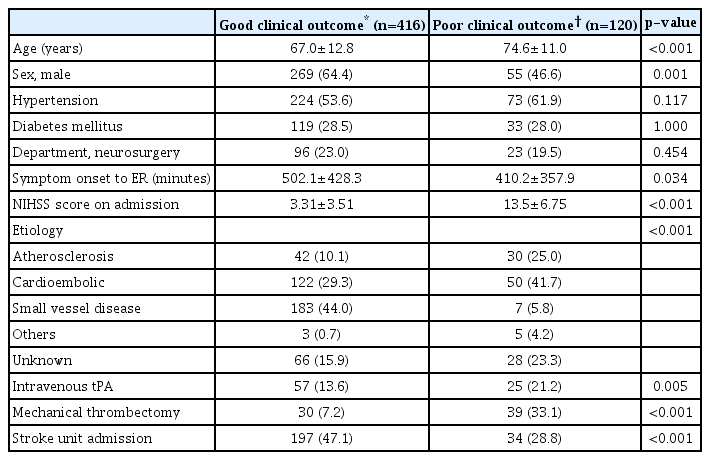
A comparison of patients with good clinical outcomes and those with poor clinical outcomes
The multivariable logistic regression analysis for factors associated with good clinical outcomes in patients with AIS, including age, sex, hypertension, time from symptom onset to ER, NIHSS score on admission, etiology, use of intravenous tPA, use of MT, and stroke unit admission, showed that age (adjusted odds ratio [OR], 0.944; adjusted 95% confidence interval [CI], 0.920–0.969; p<0.001) and NIHSS score on admission (adjusted OR, 0.730; adjusted 95% CI, 0.689–0.774; p<0.001) were independently associated with good clinical outcomes in patients with AIS (Table 3).

Multivariable logistic regression analysis of factors affecting good clinical outcome
Table 4 shows the comparison of patients who received intravenous tPA between the neurosurgeon and neurologist groups. Intravenous tPA was administered to 82 patients (15.3%) in the neurosurgeon group (n=17) and the neurologist group (n=65). The door-to-tPA time was not significantly different between the two groups (median, 53 minutes; interquartile range [IQR], 45–58 vs. median, 54 minutes; IQR, 46–74; p=0.372). Good clinical outcomes were not significantly different between the two groups (12/17 [70.6%] vs. 45/65 [69.2%], p=1.000). Mortality was also not significantly different between the two groups (1/17 [5.9%] vs. 3/65 [4.6%], p=1.000).
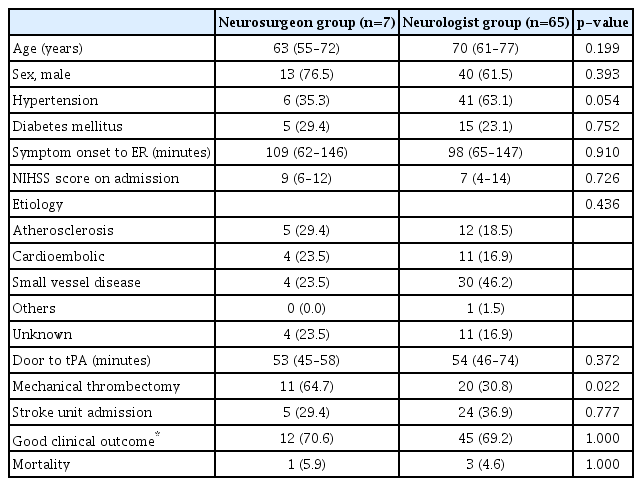
A comparison of patients with intravenous tissue plasminogen activator treated by neurosurgeons and neurologists
A comparison of patients who underwent MT treated by neurosurgeons and neurologists is presented in Table 5. Overall, MT was performed in 69 patients (12.9%) in the neurosurgeon group (n=25) and the neurologist group (n=44). Of the 44 patients in the neurologist group, 37 patients underwent MT by one of the three neurosurgeons, and six patients underwent MT by a neurologist. The neurosurgeon group achieved a shorter door-to-puncture time than the neurologist group (median, 115 minutes; IQR, 107–151 vs. median, 162 minutes; IQR, 117–189; p=0.049). Good clinical outcomes were achieved more often in the neurosurgeon group than in the neurologist group (14/25 [56.0%] vs. 16/44 [36.4%]); however, the difference was not statistically significant (p=0.135). Mortality was also not significantly different between the two groups (3/25 [12.0%] vs. 3/44 [6.80%], p=0.660).

A comparison of patients with mechanical thrombectomy treated by neurosurgeons and neurologists
DISCUSSION
The manpower shortage of neurologists for 24/7 AIS care has been reported, and neurologists are trying to overcome this problem by increasing the number of neurology residents [9]. However, there are no exact data or reports on the number of hospitals where 24/7 AIS care in unavailable. This study may provide a basis for neurosurgeons to be responsible for AIS care in situations where 24/7 AIS care is not available due to the shortage of neurologists.
In recent years, neurosurgeons have become responsible for AIS care [11]; however, neurologists play an important role in AIS care. In a previous single-center study, cerebrovascular neurosurgeons and vascular neurologists reported similar rates of intravenous tPA administration, referral to MT, mortality, and functional outcome in patients with AIS [1]. However, there are no reports on the role of neurosurgeons in AIS care in South Korea. This study suggests that neurosurgeons can provide patients with AIS with treatment efficacy and outcomes similar to those of neurologists in South Korea.
In this study, the severity of AIS was mild in most patients, and the clinical outcome of patients with AIS was good in the majority of patients. These results are consistent with those of previous studies [6,14]. Our results also showed that patients who received medical treatment only accounted for more than 70%, which is in line with previous reports [1,7]. Moreover, most patients with AIS had mild severity and good clinical outcomes after medical treatment only, and only a few patients with AIS needed thrombolytic treatments, including intravenous tPA administration and MT. Our study suggests that neurosurgeons should be interested in the treatment of patients with mild severity because these patients comprise the majority of patients with AIS.
Our results showed that MT was performed more frequently in the neurosurgeon group than in the neurologist group. In this era of doctors with subspecialties beyond specialty, cerebrovascular neurosurgeons may be more specialized in making MT decisions compared to all neurologists, including neurologists with subspecialties other than stroke [8]. Furthermore, we found no significant difference in good clinical outcomes and mortality between the neurosurgeon and neurologist groups, which suggests that neurosurgeons have comparable abilities to neurologists to care for patients with AIS in the ER.
In this study, good clinical outcomes were associated with younger age and lower NIHSS score on admission, suggesting that early neurologic status is the most important prognostic factor [3,13]. The time from symptom onset to ER was significantly longer in the patients with good clinical outcomes than in those with poor clinical outcomes. This may be partially explained by the fact that patients with mild symptoms visited the ER later than those with severe symptoms. Patients who did not receive intravenous tPA or MT achieved better clinical outcomes than those who received intravenous tPA or MT. This may be partially explained by the fact that patients with mild symptoms who did not need tPA or MT might have better clinical outcomes.
Our results showed that door-to-tPA time and good clinical outcomes in patients who received intravenous tPA were not significantly different between the neurosurgeon and neurologist groups. These results suggest that neurosurgeons can treat patients with AIS using intravenous tPA [1]. In addition, neurosurgeons achieved significantly shorter door-to-puncture time than neurologists in patients who underwent MT and that neurosurgeons tended to achieve better clinical outcomes than neurologists, which is consistent with our previous report [8]. These results suggest that neurosurgeons are more suitable than neurologists for patients with large artery occlusion who need MT by making rapid decisions and performing MT faster.
The rate of stroke unit admission was significantly different between the neurosurgeon and neurologist groups. This suggests that neurosurgeons are not fully aware of the importance of a stroke unit. The stroke unit reduces mortality and morbidity by managing exclusively in dedicated wards with a dedicated stroke team [2,16,17]. It started in South Korea in the 2010s and was distributed [10]. The low rate of stroke unit admission for the neurosurgeon group may be because neurologists are the managers of the stroke unit and neurosurgeon's patients are not easily admitted to the stroke unit. Another reason may be that neurosurgeons prefer intensive care units over stroke units. However, the effectiveness of a stroke unit is well known, and neurosurgeons should increase its use.
This study has some limitations. First, it was a single center retrospective study with attendant selection bias. Second, the sample size was small, which may have led to low statistical power. Third, it may not be fair to compare the ability of neurosurgeons and neurologists to provide AIS care in the ER in the absence of neurology residents. Finally, assessing the ability to care for patients with AIS in the ER by door-to-tPA time, door-to-puncture time, clinical outcomes, and mortality rate could be insufficient, because the ability to distinguish AIS from stroke mimics is also important [4,15].
CONCLUSION
In this study, the neurosurgeon group showed similar treatment rates and clinical outcomes to the neurologist group in patients with AIS in the ER. This study suggests that neurosurgeons have comparable abilities to care for patients with AIS in the ER. Further multicenter studies with larger sample sizes must be conducted to confirm these preliminary results.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Informed consent
This type of study does not require informed consent.
Author contributions
Conceptualization : SHK; Data curation : SHL, BSK; Formal analysis : TMN, HL; Funding acquisition : YZK; Methodology : JHJ, DHK; Project administration : KHK; Visualization : KHR; Writing - original draft : SHL; Writing - review & editing : SHK
Data sharing
None
Preprint
None