Chronic Subdural Hematoma in the Aged, Trauma or Degeneration?
Article information
Abstract
Chronic subdural hematomas (CSHs) are generally regarded to be a traumatic lesion. It was regarded as a stroke in 17th century, an inflammatory disease in 19th century. From 20th century, it became a traumatic lesion. CSH frequently occur after a trauma, however, it cannot occur when there is no enough subdural space even after a severe head injury. CSH may occur without trauma, when there is sufficient subdural space. The author tried to investigate trends in the causation of CSH. By a review of literature, the author suggested a different view on the causation of CSH. CSH usually originated from either a subdural hygroma or an acute subdural hematoma. Development of CSH starts from the separation of the dural border cell (DBC) layer, which induces proliferation of DBCs with production of neomembrane. Capillaries will follow along the neomembrane. Hemorrhage would occur into the subdural fluid either by tearing of bridge veins or repeated microhemorrhage from the neomembrane. That is the mechanism of hematoma enlargement. Trauma or bleeding tendency may precipitate development of CSH, however, it cannot lead CSH, if there is no sufficient subdural space. The key determinant for development of CSH is a sufficient subdural space, in other words, brain atrophy. The most common and universal cause of brain atrophy is the aging. Modifying Virchow's description, CSH is sometimes traumatic, but most often caused by degeneration of the brain. Now, it is reasonable that degeneration of brain might play pivotal role in development of CSH in the aged persons.
INTRODUCTION
Chronic subdural hematomas (CSHs) are generally regarded to be consequences of head trauma1451). The most commonly accepted pathophysiological explanation of CSH is that mild head trauma leads to tearing of bridging veins with subsequent bleeding, thus creating the hematoma7). However, a history of trauma is absent in about 30–50% of the cases, especially after the age of 65 years1121952). Besides trauma, there were numerous risk factors such as alcohol abuse, seizures, cerebrospinal fluid shunts, and coagulopathies including therapeutic anticoagulant1451).
In 17th century, CSH was a stroke. It became an inflammation in 19th century and finally a traumatic lesion in 20th century. Trauma is the most commonly alluded as a cause, however, it cannot occur when there is no enough subdural space even after a severe head injury. If there is sufficient subdural space, CSH may occur without trauma such as intracranial hypotension. Causation of CSH is an important issue in the accident insurance. The author tried to investigate trends in the causality of CSH.
MATERIALS AND METHODS
A computerized search of the National Library of Medicine (PubMed) database of the up-to-date literature (published from 2010 to 2014) was undertaken. The medical subject headings "chronic subdural hematoma" combined with "causality" yielded 197 citations (excluded non-English language and non-human citations). The abstracts of relevant citations were reviewed and 41 articles were selected. The selected papers have been categorized into one of five categories by the causalities proposed by the authors (Table 1). By a review of literature, the author suggested a different view on the causation of CSH.
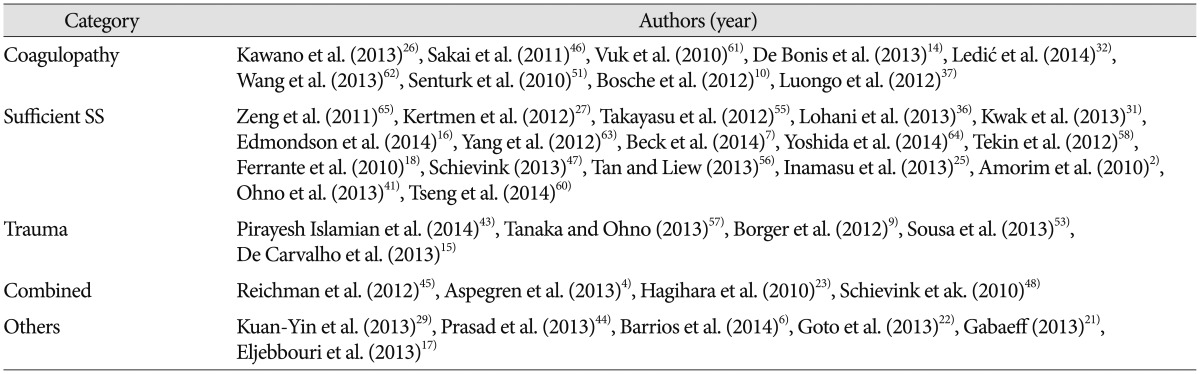
Causality of chronic subdural hematomas in selected papers (2010–2014)
RESULTS
As the cause of CSH, sufficient subdural space was alluded in 19 papers, coagulopathy in 13 papers, and trauma in 8 papers, including the combined categories. Sufficient subdural space included arachnoid cyst, cerebrospinal fluid leak, lumbar drainage, spinal anesthesia, intracranial hypotension, hydrocephalus, excerebral atrophy, and the old age. Coagulopathy included factor X deficiency, factor XIII deficiency, von Willebrand's disease, afibrinogenemia, anticoagulant therapy, and end stage renal disease. Trauma included head-banging, dancing, and any tears in the arachnoid membrane following contusion of the brain or slight bleeding from a bridging vein. Combined category included trauma with coagulopathy or sufficient subdural space with coagulopathy. Others included dural metastasis, lymphoma, infection, antiviral therapy, and birth related complications.
DISCUSSION
Sufficient subdural space was the most commonly alluded as the cause of CSH. The number of papers did not have a value by itself, since papers did not have equal frequency or importance. However, it may represent relative importance or apportionment of certain factors. Recent papers may not represent the whole aspects of the causation. They may have a tendency to publish atypical cases. However, we can explore this curious lesion using the more updated knowledge.
Traditional model of causation, so-called the classic epidemiologic triangle of host, agent, and environment was not suitable for CSH. To evaluate relative importance in multiple causation, web of causation model with directed acyclic graph (Fig. 1) is more suitable. Development of CSH starts from the separation of the dural border cell (DBC) layer, which can occur either by trauma or low intracranial pressure. Severe trauma cannot produce a CSH even in a patient with coagulopathy, when the subdural space is not enough. Trauma cannot be the causality of CSH in this situation. Furthermore, CSH may occur without trauma. Causation implies that there is a true mechanism that leads from exposure to disease. Trauma or bleeding tendency is frequently associated with CSH and they may precipitate development of CSH, however, it cannot lead CSH, if there is no prerequisite. The key determinant for development of CSH is a sufficient subdural space, in other words, cerebral atrophy. The most common and universal cause of cerebral atrophy is the aging. If we classify a disease according to the key determinant, cerebral atrophy is responsible for the CSH instead of trauma.

Schematic representation of the web of causation model for causation of chronic subdural hematoma. Development of CSH starts from the separation of the dural border cell (DBC) layer. Trauma or bleeding tendency may precipitate hematoma formation, however, it cannot produce chronic subdural hematoma, when there is no potential subdural space. The real lines mean direct causal relationships, while the dotted lines represent precipitations. Adopted from Lee KS et al.34), with permission from Br J Neurosurg.
Trauma was so frequently observed that CSH might be a traumatic lesion. The majority of CSHs are suspected by an undiagnosed trivial head injury. This assumption is hard to explain why CSH is rare in the young with severe head injury, while the majority of CSH occur in the old even without trauma33). In patients without trauma history, we presumed that they forgot the trauma, since the CSH is common in the aged and alcoholics. However, there are numerous cases of CSHs without trauma3781011152428303940424748495962), which made trauma as an associated factor instead of the cause.
Bleeding tendency clearly has a significant association with an increased risk of CSH14). Because of the continuing rise of life expectancy and the increasing use of anticoagulants, the incidence of CSH is expected to rise45142035). Anticoagulant and antiplatelet therapy became an important risk factor for development of CSH. However, bleeding tendency cannot lead CSH by itself.
Although about two-thirds (57–78.7%) of CSHs were in persons older than 65 years553), CSH does not occur in all aged person. Since aging and cerebral atrophy are universal, atrophy alone is not enough to explain the causality of CSH. The author suspect the cranial size and morphology as an important predisposing factor. Cerebral atrophy produce negative pressure within the cranium. This negative pressure is constant on each side of the cranium, according to Boyle's law, which the pressure of gas tried to hold at a constant temperature change by inverse with the volume of the gas. As the degree of atrophy is constant, the decreased length of brain diameter on the large hemisphere is longer than on the small hemisphere (Fig. 2). So, the distance from the skull to the cerebral cortex in the shrunken hemisphere is longer on the side of large hemisphere. The bridging vein is more stretched on the large hemisphere, so it may be tore by a trivial injury. If the distance exceeds the length of the arachnoid trabeculae, separation of the DBC layer will occur at the large hemisphere, which will create so-called the subdural space. For example, overall 10% reduction result 2 cm in the left, 1.5 cm in the right in the male cranium. While in the female cranium, 9% reduction (the degree of atrophy is less severe than male) of shorter diameter result about 1.5 cm in the left side. This anatomical difference of the cranium influences the left and male prevalence of CSH. Actual separation of the DBC layer will depends on the force pulling the arachnoid trabeculae, which is the sum of the cranial morphology and the degree of cerebral atrophy.
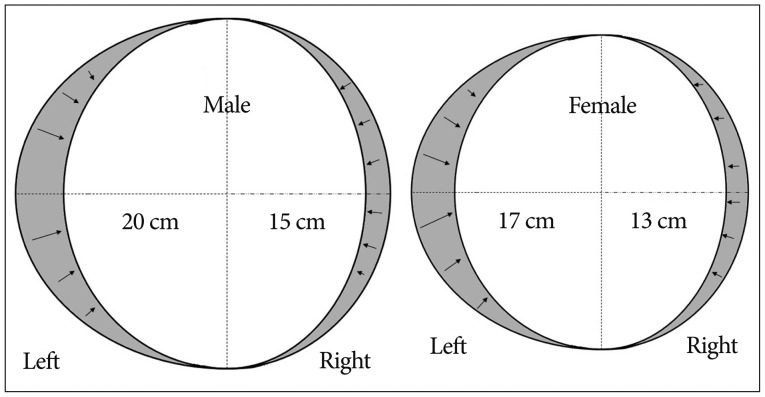
Schematic explanation for the difference in the incidence of chronic subdural hematoma. Anatomical difference of the cranium may influence the left and male prevalence of chronic subdural hematoma. The length and degree of atrophy in this figure are not actual data.
CONCLUSION
The origin of a CSH is multiple. It can be developed spontaneously, or changed from a subdural hygroma or an acute subdural hematoma. A more important prerequisite is sufficient potential subdural space that is aging, degeneration of the brain. CSH was a stroke in 17th century13), an inflammation in 19th century, and it became a traumatic lesion in 20th century38). Virchow recognized that hematoma durae matris sometimes was traumatic, but he believed that this lesion was most often caused by chronic inflammation (pachymeningitis chronica hemorrhagica) of the dura1354). Modifying Virchow's description, CSH is sometimes traumatic, but most often caused by degeneration of the brain. Now, it would be reasonable that in the aged persons, degeneration of brain might play the most important role in development of CSH.