INTRODUCTION
Cranioplasty complications are well documented and include infection, bone resorption, intracerebral hemorrhage, and infarction2,34,612). This report details a case of unexpected, severe postoperative cerebral edema following autologous cranioplasty. There are few reported cases of cerebral edema after cranioplasty5,1114). We discuss the potential pathological mechanisms of this complication.
CASE REPORT
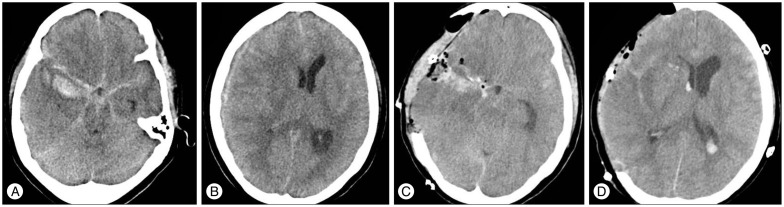
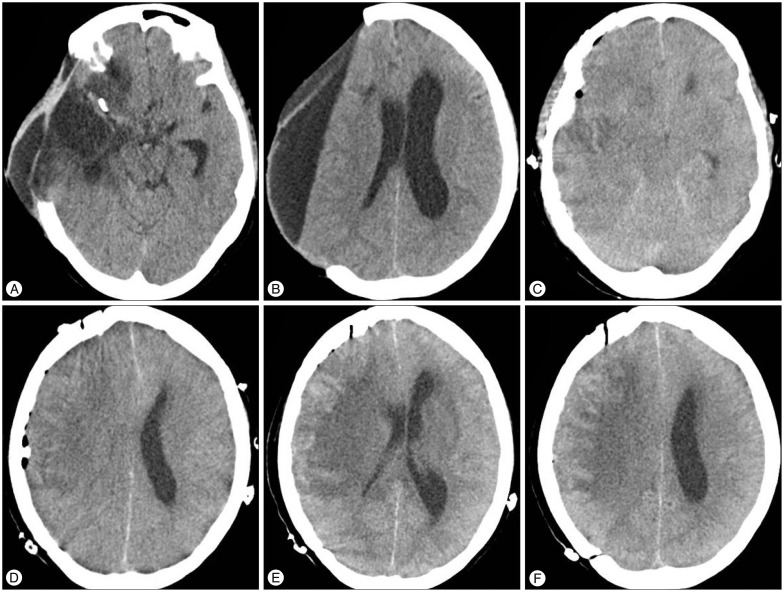
A 50-year-old female was admitted to our department with sudden-onset stuporous consciousness. A brain computed tomography (CT) scan revealed a subarachnoid hemorrhage with a right temporal lobe intracranial hemorrhage and a right subdural hematoma. Following the CT, angiography demonstrated an aneurysmal sac at the right posterior communicating artery (Fig. 1). Emergency decompressive craniectomy (DC) and aneurysmal neck clipping were performed. Following recovery there was some sinking of the scalp flap, and the decision was made to proceed with an autologous cranioplasty 61 days after the initial hemorrhage. There were no complications during the cranioplasty procedure, and there was no evidence of cardiovascular instability or cerebral swelling. Epidural and subdural drains were placed and connected to a suction system during skin closure. Following skin closure the drains were connected to a drainage bag to avoid subgaleal and epidural blood accumulation. However, the patient had a seizure in the recovery room. Emergency brain CT revealed widespread cerebral edema (Fig. 2). The patient extended her extremities in response to painful stimuli with no evidence of awareness. Therefore, the decision was made to clamp the drain catheters. The increased intracranial pressure (ICP) and cerebral edema were controlled with osmotic diuretics, corticosteroids, and antiepileptic drugs. The edema slowly subsided, but new low-density areas were noted on follow-up brain CT 1 week after the cranioplasty (Fig. 2).
DISCUSSION
Patients who survive DC need to undergo a second procedure, a cranioplasty. Complications following cranioplasty, including epidural or subdural hematoma, wound healing disturbance, subdural hematoma, cerebrospinal fluid fistula, infection, and bone graft resorption, are a significant cause of post-operative morbidity2,34,612). There are only five reported cases of unexpected cerebral edema after cranioplasty5,1114). Honeybul5)reported three cases of sudden death following massive post-operative cerebral swelling after autologous cranioplasty. All three patients had a bifrontal DC for intractably raised ICP following severe neurotrauma, and developed hydrocephalus necessitating shunt insertion. The author speculated that some degree of autoregulatory impairment and change in brain compliance due to the development of hydrocephalus and subsequent insertion of a ventriculoperitoneal (V-P) shunt may have contributed to the outcome. Santana-Cabrera et al.11) reported a similar case of massive post-operative cerebral edema following cranioplasty. Zebian and Critchley14) reported the case of a patient with an aneurysmal subarachnoid hemorrhage who underwent unilateral DC. During the cranioplasty there was a negative pressure shift causing the brain to expand rapidly to fill the defect within the skull; this shift may have been further exacerbated by the drain being placed on full suction. Of these reported cases, four were traumatic brain injury patients and one had cerebral edema following aneurysmal neck clipping. Bifrontal craniectomy was performed in four cases and left-sided unilateral craniectomy in one, while our patient underwent a right-side unilateral craniectomy. In addition, four of the previous cases underwent a V-P shunt operation prior to cranioplasty due to hydrocephalus, but our patient did not have hydrocephalus.
In the presented case, several factors contributed to the development of severe swelling following cranioplasty. The exact pathophysiological mechanism behind severe cerebral edema and sudden death following cranioplasty is poorly understood. Potential contributing factors include some degree of autoregulatory impairment, change in brain compliance due to the development of hydrocephalus, and the acute lowering of ICP. The underlying cause must be related to a failure in the autoregulatory process. The brain, which is subjected to atmospheric pressure prior to cranioplasty, appears to shift toward negative pressure, causing a rapid expansion of the brain to fill the defect within the skull.
Another point to consider is that the acute lowering of ICP may lead to intracranial hemorrhage in various scenarios. Roth et al.10) reported that continuous suctioning of the subgaleal and epidural space may induce a negative ICP that is sufficient to cause epidural hematomas and hemodynamic collapse. We speculated that placing the epidural and subgaleal drains on active suction in our patient may have caused an acute decrease in ICP leading to subsequent rapid expansion of the brain, which impaired autoregulation and led to reperfusion injury.
A few studies have reported neurological improvement following cranioplasty in craniectomy patients, and they indicated that the mechanism of recovery involves a significant increase in cerebral blood flow and cerebral energy metabolism7,813). Sometimes the brain is unable to endure sudden hyperperfusion after cranioplasty due to complications, such as diminished autoregulation, cerebral blood flow, and cerebral metabolism1,9). Therefore, physicians should remember that reperfusion injuries can occur following cranioplasty in patients with large skull defects.