INTRODUCTION
Penetrating cerebral injuries caused by foreign bodies other than bullets are relatively rare due to the substantial mechanical protection provided by the skull. In clinical practice, such injuries are mostly due to industrial accidents and criminal assaults2,8). Several descriptions of foreign bodies such as wood pencils or metal penetrating the cranium have appeared in the literature5,6). However, suicide attempts and self-inflicted nail gun injuries are rarely reported. A good neurological outcome can be expected if the free ends of the nails can be seen in the operative field and if the brainstem and major vessels are spared12). Here we report on a difficult case of deep-seated intracranial nail gun injury in which the free end of the nail was not seen.
CASE REPORT
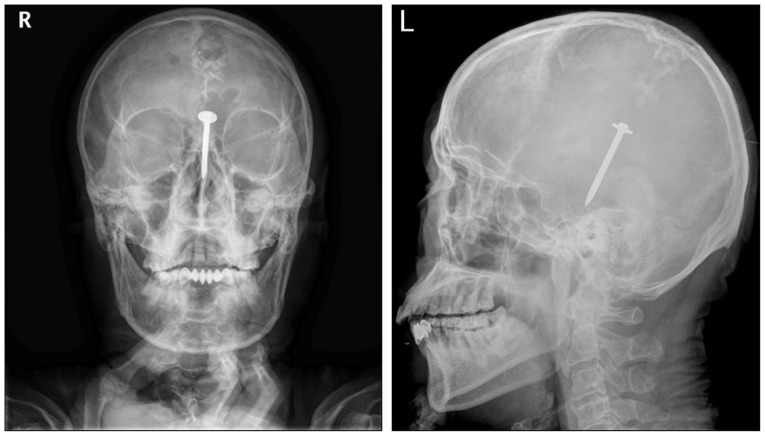
A 43-year-old man was referred to the emergency room due to altered mental status subsequent to a self-inflicted nail gun wound. During a quarrel with a co-worker, he attempted suicide by shooting himself with a nailing gun at his workplace. On physical examination, he was found to have an open laceration about 2√Ч1 cm in the left parietal region. On neurological examination, he was found to be drowsy with a Glasgow coma scale of 14 (E4 V4 M4). He showed right side hemiparesis (Grade II/Grade I). Plain skull radiographs revealed a 5-cm, linear, nail-shaped foreign body piercing the brain (Fig. 1).
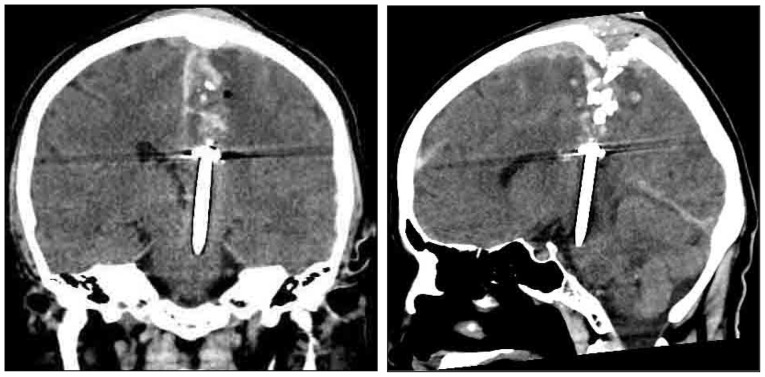
A computed tomography (CT) scan of the brain showed the presence of a metallic foreign body in the left parietal lobe. It reached almost to the pons, and multiple fracture fragments were also seen impacted into the parietal lobe (Fig. 2).
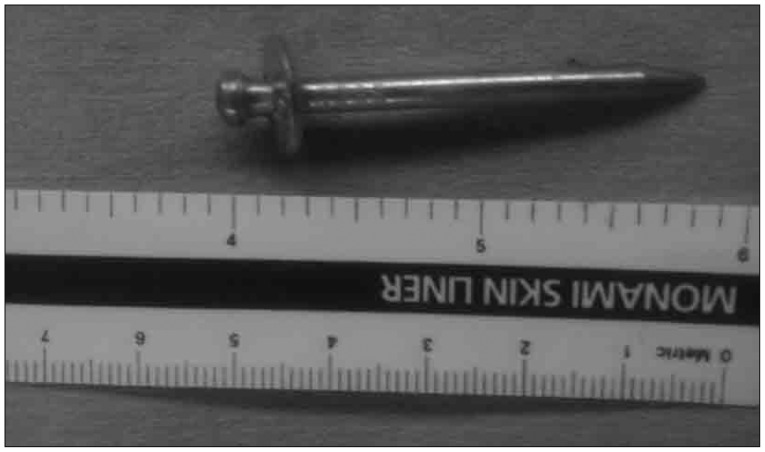
Treatment with a combination of ceftriaxone, chloramphenicol, and metronidazole was initiated and tetanus immunization was administered. The patient was operated immediately and a local scalp incision was made at the nail entry site. After a small circumferential craniectomy, the nail was cautiously removed under intraoperative C-arm guidance to prevent further vascular insult or neurological aggravation (Fig. 3). After washing the wound with antibiotics, it was closed in layers over a drain.
The postoperative period was uneventful and the patient exhibited no further neurological aggravation, evidence of infection, or symptoms of raised intracranial pressure. However, in spite of aggressive rehabilitative treatment for 3 months, his right side hemiparesis was not improved and he could not ambulate by himself.
DISCUSSION
Although gunshot injury is rare in Korea due to gun control, penetrating cranial injuries still occur, mostly from shotguns10). Other causes are infrequent and include criminal assaults and industrial accidents9). A few cases of deliberate, self-inflicted, penetrating brain injury from nail guns have been reported12,13). In most of these cases, patients survive with a good neurological outcome if the brainstem and major cerebral vessels have been spared and the offending nail is seen during physical examination. However, in our case, the free end of the nail was not seen and only the penetration site could be observed. As a result, we were obliged to remove the foreign body using blind technique.
Neuroimaging is vital for surgical decision-making in any penetrating head injury, offering guidance as to the best surgical approach, the size and site of the craniotomy, and the route of extraction of the foreign body, as well as informing the decision to choose non-surgical management. Simple radiographs are helpful for intracranial localization of metallic foreign bodies1,2,5). In the case of non-metallic bodies, cranium defects or the foreign body itself can occasionally be seen14). CT scanning of the brain is now the primary modality used in the neuroradiologic evaluation of patients with penetrating head injury. This is because CT scanning is quick and provides improved identification of in-driven bone and missile fragments, characterization of the missile trajectory, evaluation of the extent of brain injury, and detection of intracranial hematomas and mass effects11). In contrast, magnetic resonance imaging has limitations that restrict its use in practice. The strength of the magnetic field poses a danger when any ferromagnetic metals are present as foreign bodies. For the same reason, we could not use a three-dimensional navigation system in our patient. It is recommended that documenting vascular damage should be performed using cerebral angiography when the foreign body is located just beneath the major arterial or venous systems1).
In spite of the development of antibiotics, infectious complications are frequently seen in the penetrating head wound patients. Prompt surgical exploration is mandatory to reduce the mortality and complication rate. Despite antibiotic treatment, the morbidity rate is 33% in cases receiving prompt surgical treatment and rises to 53% in cases where surgery is delayed9). Small sized foreign bodies located deep in the brain can be left in place7,10,12). If the foreign body is not in close proximity to major arteries or veins and has extracranial components, a blind removal without craniotomy can be performed. However, deterioration and death have been described after removal in such cases3,4). Surgery should be performed for removal of a contaminated foreign body, repair of vascular or dural damage, or drainage of intracranial masses6,7). Bony fragments should also be excised to prevent complications. Removed foreign bodies should be cultured for aerobic, anaerobic, or fungal pathogens. In our case, all cultures were negative. Complications of attempts to treat this kind of injury include meningitis, cerebral abscess, hematomas, cerebral aneurysm, hydrocephalus, and focal neurological deficits7).