INTRODUCTION
Chordomas are pathologically benign tumors that originate from the notochord remnant which are typically midline and extradural lesion. Because of their location, ventral to the brain stem and invasive nature with vital neurovascular structures, skull base chordomas are difficult to treat, especially for gross total resection (GTR), hence the reason for recurrence. An aggressive surgical approach to attempt en-bloc resection and subsequent postoperative radiation therapy is recommended as the current therapeutic algorithm [13]. The surgical resection has a definitive role in the management of skull base chordomas. More extensive tumor removal has been associated with better prognosis [23,28]. Furthermore, selection of the surgical approach is also a significant factor for achieving radical resection. Most otorhinolaryngologists and neurosurgeons traditionally use the midline and lateral approaches in order to gain access to the skull base chordomas. The anterior midline approaches consist of extended subfrontal, transmaxillary, transmandibular, transsphenoidal, endonasal endoscopic, transoral, and transcervical approaches [3,6-8,20,27]. Transcranial lateral approaches (TLA) include frontotemporal transcavernous, orbitozygomatic, anterior transpetrosal, preauricular infratemporal, and extreme lateral transcondylar approaches [17,19,21,24,25]. All surgical approaches should be selected with the goal of GTR and minimal morbidity and mortality at the same time. However, when the tumors extend to more than one contiguous anatomical areas of skull base, radical removal may be difficult to achieve with a single approach, two or more surgical procedures are required [1].
The purpose of this study is to analyze the surgical outcomes of transnasal midline approaches (TMA) and TLA for the treatment of skull base chordomas over the last 10 years in our institute, and to summarize the appropriate surgical approach according to the growth pattern of tumors in order to obtain the best surgical outcomes.
MATERIALS AND METHODS
Patients
This retrospective study was in accordance with the ethical standards and approved by the Institutional Review Board (IRB) of Tianjin Huanhu Hospital (IRB No. 2022-002). We retrospectively reviewed 48 patients with histopathologically diagnosed skull base chordoma in our institution between January 2010 and September 2020. Data for all patients are obtained from patientsŌĆÖ medical records, radiological imaging data, and telephone interviews if necessary. All patients were assessed with Karnofsky Performance Scale (KPS) scores on admission, at discharge and 6 months after surgery.
Imaging assessment
All patients underwent a preoperative workup including magnetic resonance imaging (MRI), computed tomography (CT) and CT angiography to evaluate the characteristics of the tumor. The primary characteristics are listed as follows : 1) location and size in three dimensions, their volumes are calculated by A├ŚB├ŚC where A, B, and C are the maximum diameters of the chordoma in axial, coronal, and sagittal; 2) the extent of tumor invasion into surrounding tissues including the relationship between tumor and internal carotid artery (ICA), vertebral artery (VA), basilar artery (BA) and brainstem. Vascular involvement is defined as displaced, steno-occlusion or encased by tumor; and 3) the extent of bony infiltration and vascular involvement. The postoperative gadlinium enhanced MRI within 3 days was obtained to assess for any tumor residual. Extent of resection was categorized as GTR if there was no apparent residual tumor on postoperative MRI, and as subtotal resection (STR) for any radiographic residual (tumor removal greater than 90%), and as partial resection (PR) for most of the tumor residual (removal between 50% and 90% of the tumor).
Surgical procedure
The surgical approaches are divided into two types : TMA and TLA. The former included endonasal microscopic approach (EMA) in the early stage and endonasal endoscopic approach (EEA) at a later stage. The latter, depending on the location of the tumor, consists of frontotemporal approach, transcavernous approach, combined approach, extreme lateral transcondylar approach. The procedure of the EEA is as follows which performed by both neurosurgeons and otorhinolaryngologists. The basic indications for surgical approach selection is that the TMA was preferred for patients whose tumor was located in the midline ventral skull base with a small lateral extension or not. However, the TLA was preferred primarily because the tumors extend widely to the lateral skull base, such as invasion of the middle cranial fossa, petrous bone, infratemporal fossa, close relationship with important intracranial vessels or extensive intradural invasion and obvious brainstem compression. On the other hand, the decision was sometimes made based on the surgeonŌĆÖs familiarity with different skull base approaches.
The patient is placed in a supine position with the trunk elevated 10┬░ and the head turned 10┬░ toward the surgeon. Prepared a fat and/or fascia lata grafts in the anterolateral thigh or abdomen to repair bone and dural defects. A straight 4-mm endoscope for tumor removal and angled scopes for observation. Both nasal cavities were filled with adrenaline saline cottonoids to enlarge the space between turbinates and nasal septum to obtain decongestion of the nasal mucosa. The binostril four-hand technique was applied if necessary, especially in cases with cavernous sinus (CS) invasion and subdural extension. The right middle turbinate was resected and a vascularized nasoseptal flap was prepared and placed around nasopharynx, then the posterior segment of the nasal septum was removed. When the entire anterior wall of the sphenoid sinus was visible, bone punches or a microdrill was used to enlarge circumferentially. The anterior wall of the sphenoid sinus should be widely removed before reaching the sella. The sphenoid sinus floor was drilled down to the clivus recess, a wide sphenoidotomy and posterior etmoidectomy was performed to form a corridor between the maxillary sinus and the sphenoid sinus. At this time, some important anatomical landmark need to be identified, including optic nerve, optocarotid recess (OCR), cavernous segment and paraclival segment of ICA. The epidural portion of tumors can be identified and removed after the eroded bone was drilled. The cases with subdural extension that adjacent to the BA and brainstem should be resected carefully with four-hand technique. At the end of the procedure, the skull base defect was reconstructed using a multilayer graft harvested by fat, fascia lata, and vascularized nasoseptal flap. Finally, fibrin glue was used at the edges of the bone in order to fix the whole reconstruction.
Statistical analysis
IBM SPSS Statistics ver. 25 (IBM, Corp., Armonk, NY, USA) was used for statistical analysis. The chi-square test or FisherŌĆÖs exact test was utilized to evaluate the categorical data. The differences in medians between two variables were evaluated with Mann-Whitney U test. Kaplan-Meier analyses was used to analyze cumulative survival rates and cumulative recurrence free survival/progression free survival (RFS/PFS). All of p-values are 2-sided and 2-tailed and p<0.05 was considered statistically significant.
RESULTS
Demographic and clinical characteristics
Table 1 summarized the patientsŌĆÖ demographic information and clinical symptoms of the two groups. Among the 48 patients, there were 22 males and 14 females in the TMA group; four males and eight females in the TLA group. No statistical difference was reached in gender. The median age was 58.0 (10-71) and 39.5 (20-61), respectively. Patients in TMA group were older than that in TLA, and reached a statistical difference (p=0.014). In TMA group, symptoms leading to diagnosis were headache in 15 cases (41.7%), dysopia in 12 cases (33.3%), abducens nerve palsy in four cases (11.1%), facial numbness in one case (2.8%), dysphagia in two cases (5.6%), incidental found in two cases (5.6%); in TLA group, headache in four cases (33.3%), dysopia in three cases (25%), abducens nerve palsy in one case (8.3%), facial numbness in one case (8.3%), limbs weakness in two cases (16.7%) and one case with hypacusis (8.3%). There was no statistical difference in all symptoms between the two groups.
Comparison in surgical outcomes between the two approaches
Table 2 displayed the detailed comparisons of the two approaches; the tumor location and extension based on imaging data were also listed. The tumor extension was primarily focus on the relationship between tumor and CS, ICA, VA, BA, dura matter and brainstem. There was no statistical significance in tumor location and extension between the two groups. Among the 36 patients in the TMA group, 18 underwent EMA and 18 performed by EEA (primary surgery in 28 cases and recurrent surgery in eight cases); while among the 12 patients in the TLA group, nine cases with primary surgery and three cases with recurrent surgery. The median tumor volume was 27.1 cm3 (2.7-159.1 cm3) in TMA group and 46.1 cm3 (15.1-232.0 cm3) in TLA group. The tumor volume in the TLA group was larger than that in the TMA group with no statistically significant (p=0.063).
In terms of the extent of resection, the overall number of GTR was 12, STR was 30 and PR was 6, among which 10 cases reached GTR, 21 cases of STR and five cases of PR in the TMA group; in TLA group, there were two cases of GTR, nine cases of STR, and one case of PR. The GTR rate was 27.8% vs. 16.7% (p=0.700). However, there are some differences in GTR rates under different conditions, as shown in Table 3. For the primary surgery, the GTR rate was 29.7%, and for the surgery after tumor recurrence, the GTR rate was only 9.1% (p=0.322). In the midline approaches, the GTR rate was increased to 38.9% via EEA compared with 16.7% followed by EMA (p=0.264).
Complications
As seen from Table 2. In the TMA group, cerebrospinal fluid (CSF) leakage was the most common complication, accounting for 36.1% (13 cases). Of the 13 cases, two of them leaded to intracranial infection and improved after antibiotic treatment. Lumbar drainage was performed in seven cases and a surgical repair in one case due to a persistent leakage. The others included two deaths during the operation, mainly caused by intraoperative CS hemorrhage and brainstem failure because of delayed intracerebral hemorrhage respectively, cranial nerve (CN) palsy in two cases and two cases of hypopituitarism. On the other hand, in the TLA group, there were no deaths during the surgery, only one patient had CSF leak and ceased after the lumbar drainage in 2 weeks, CN palsy in three cases, hypopituitarism in two cases, and one epilepsy and one epidural hematoma that required surgical removal. The comparison of all complications did not reach statistical significance. The mean length of postoperative hospital stay was longer in TLA group than that in TMA group (19.5 vs. 9.0 days, p=0.006).
Life status and follow up
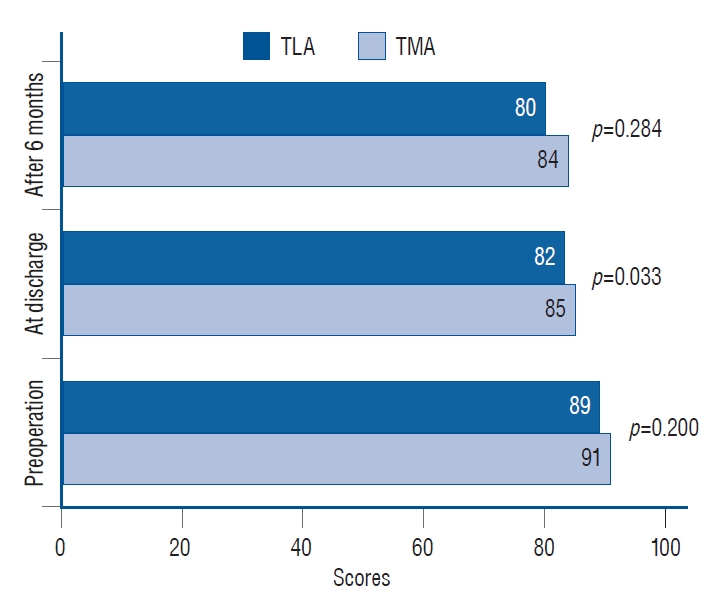
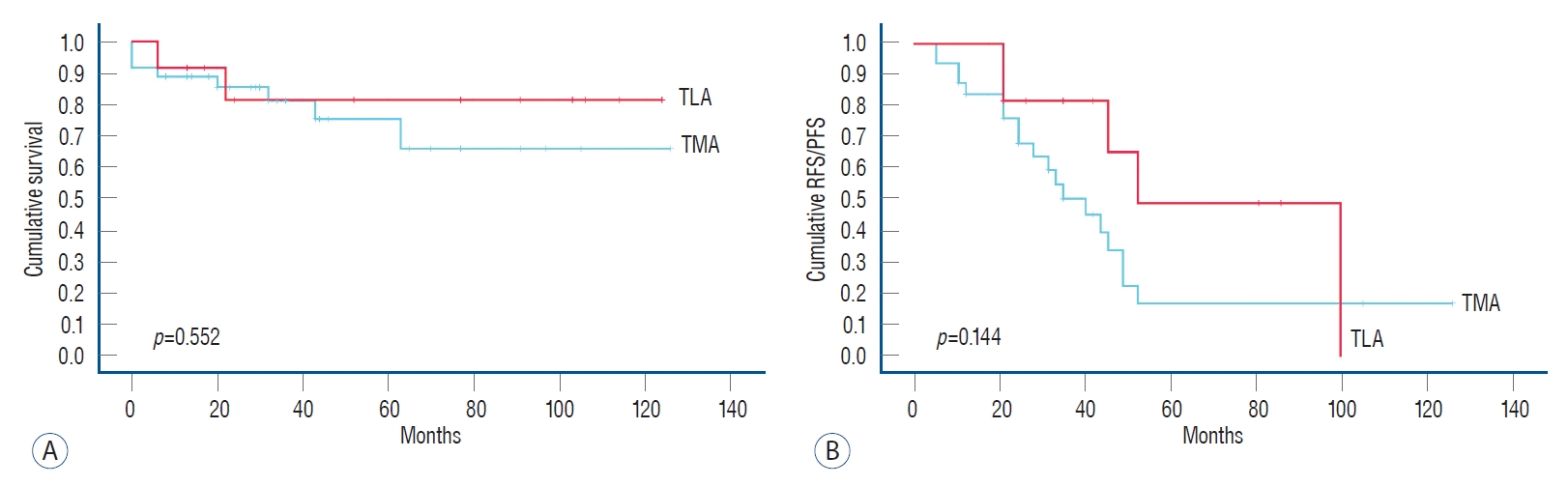
The KPS scores in each group during different periods were shown in Fig. 1. The mean KPS score can more intuitively reflect the life status, which was slightly higher in the TMA group than that of TLA group before surgery, at discharge and 6 months later after discharge, and the KPS score at discharge was statistically significant. The median follow-up period of the two groups was 35.0 months (6-126 months) and 64.5 months (6-124 months), respectively (p=0.296) (Table 4). During the follow-up period, 19 patients in TMA group and six patients in TLA group were found to tumor recurrence, the number of deaths added to six in TMA and two in TLA, seven of whom died from disease progression with no further treatment and one patient died after two more surgeries in another hospital. The median overall survival (OS) was 37.0 months (8-129 months) in the TMA group and 82.5 months (7-192 months) in the TLA group (p=0.050), and the median RFS/PFS was 15.0 months (3-72 months) and 24.0 months (12-57 months), respectively (p=0.094). Fig. 2 shows the cumulative survival rate (p=0.552) and cumulative RFS/PFS (p=0.144) of the two groups, and there were no statistical differences.
Illustrative cases
Case 1
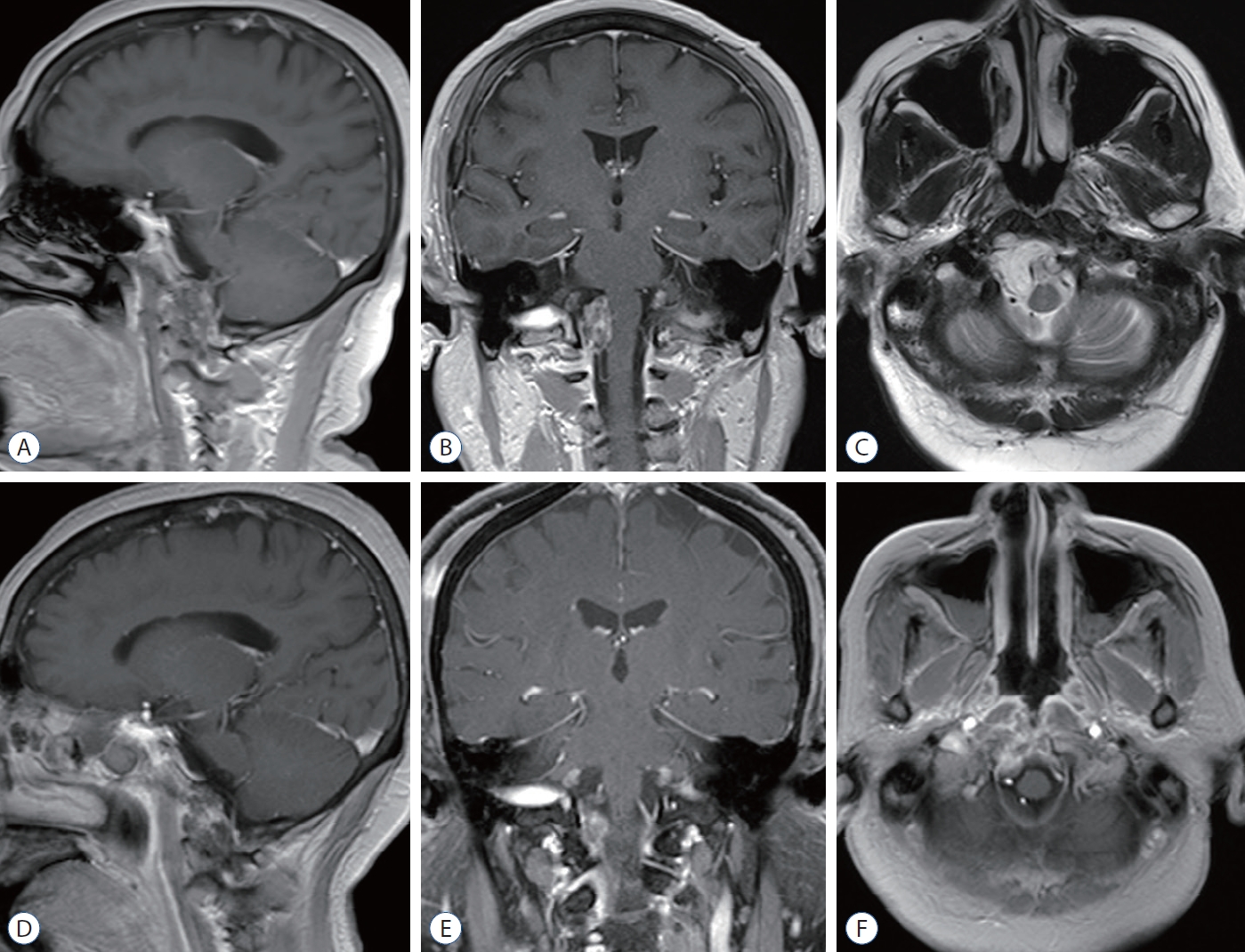
This case is presented to illustrate the EMA to remove skull base chordoma. A 29-year-old woman clinically presented with dysopia in both eyes for half a month and mild headache. Physical examination revealed binocular dysopia and bilateral visual field defects. Preoperative MRI scans showed a large and destructive mass in the sellar-spheoid-clivus area with CS and carotid artery involvement bilaterally (Fig. 3A-C). Her preoperative KPS score was 90. The lesion was removed by EMA with STR achieved (Fig. 3D-F). The symptom was somewhat restored immediately after surgery, considering that most of the tumor had been removed and complete optic nerve decompression was performed. Postoperatively, there was no CSF leak but slight hypopituitarism. The KPS score at discharge was 90 with no postoperative radiotherapy administered. The visual impairment has not completely recovered in the follow-up period.
Case 2
This case is presented to illustrate the EEA for treating skull base chordoma. A 65-year-old woman presented with intermittent headache for a half year and XIIth CN palsy, KPS score was 90 on admission. A preoperative MRI scan revealed an inferior clival chordoma with right medulla compression (Fig. 4A-C). She underwent a GTR by EEA (Fig. 4D-F). CSF leak occurred during the operation, and the subcutaneous fascia lata was harvested for plugging. Lumbar drainage was performed postoperatively, which was removed 5 days later. The KPS score at discharge was also 90 and remained XIIth CN palsy. No radiotherapy was administered because the tumor was completely resected.
Case 3
This case is presented to illustrate a case where the tumor progressed again after eight previous surgeries. This is the ninth operation via combined TLA. A 31-year-old man initially presented with IXth and Vth CN palsy, headache, and limbs weakness in 2013. After eight previous operations in other institutes, the clinical manifestation of this time (July 2019) was right limb weakness. The preoperative KPS was 80. On MRI scans, a destructive tumor was revealed extending from the upper-clivus to the craniocervical junction (CVJ) (Fig. 5A-C); the medulla was compressed and involved the left temporal and infratemporal fossa upward. This tumor was mostly removed by combining an extreme lateral transcondylar approach and infratemporal fossa approach for palliative purposes (Fig. 5D-F) with residual tumor in lower-clivus. No CSF leak occurred but the IXth, Xth and XIth CNs were injured. He was discharged from hospital with a 50 KPS score, indicating that the part of life can be self-care, but often need someone to take care of. Postoperative radiotherapy was not received in consideration of his life status and KPS score remains unchanged during the follow up.
DISCUSSION
Chordomas are rare, slow-growing, locally destructive midline tumors. Although pathologically considered to a benign neoplasm, chordomas have a rate of recurrence, their invasive growth pattern is often more typical of a malignancy. Headaches, dysopia and CNs palsy are the most clinical presentations and neurological signs. Surgical resection is one of the pivotal factors affecting the prognosis. Many publications have supported that radical resection is generally considered the best treatment [1,5,22,23,28]. For all this, taking the difficulty of accomplishing a GTR and the potential high morbidity related to aggressive tumor removal into account, safe cytoreduction with radiotherapy or staged surgical procedures seems to be another acceptable option, especially suitable for cases that are difficult to remove in a single surgery. Meanwhile, when considering to perform a staged surgery, based on the location and growth pattern of the tumor, it is crucial to select an appropriate surgical approach in the first operation to remove as much tumor as possible in preparation for the later second operation.
EMA
In view of most skull base chordomas have a center in the vicinity of the midline (Fig. 6), the transsphenoidal route often provides the most direct corridor and minimally invasive approach for lesion resection. As a matter of fact, when the endoscopy had not widely used in the treatment of skull base chordomas, EMA was used infrequently. Several literatures had reported a series of results through this approach. Maira et al. [15] reported a series of 12 clival chordomas, GTR was achieved in nine cases (75%). In a report of 18 patients with clival chordomas treated with extended microsurgical transsphenoidal approach by Couldwell et al. [6], GTR was achieved in 12 (66.7%). Fatemi et al. [9] reported 14 cases of clival chodomas with microsurgical transsphenoidal, GTR was achieved in 43%. Meanwhile, they pointed out that the use of the endoscope was associated with gross total or near-total tumor removal. In our series of 18 EMA cases, 16.7% with GTR and 66.7% with STR. The reasons why using EMA in the early stage are because of the fact that their tumor epicenter in the clivus or sellar with relatively few cases extending laterally, no open surgery and brain retraction are required, and the lack of experience in the use of endoscopy in the treatment of skull base chordoma. Given the limited lateral exposure, they were not sufficient for complete removal under most circumstances.
EEA
With the advent of endoscopic technology, it has been increasingly used to treat midline skull base lesions. The approach that averts brain retraction, large vessel and nerve manipulation was developed initially for intrasellar lesions and had been proved to obtain a good outcome. Recent advances in endoscopic facilities combined with neuronavigation and good cooperation with otolaryngologists have expanded the scope of endoscopic skull base surgery, clival chordomas are one of them. Furthermore, proficient mastery of the binostril approach as well as the four-hand technique makes the procedure more flexible under endoscopy. Recently, an increasing number of publications reported the EEA for skull base chordomas [2,10,12,14,30]. The GTR rate ranged from 33% to 86% [16], of which for primary tumors this can be as high as 80%, while that of recurrent tumors reduced to less than 50% [2,14]. In contrast to microsurgery, the endoscopy enables a panoramic view rather than a narrow microscopic view. The access to entire ventral skull base is available by EEA. The rational of this approach is that the neurovascular and brainstem are always posterior or lateral to the tumor. Fig. 6 reveals the midline areas within the shadow, connecting the median wall of orbit, lateral wall of the CS, internal auditory canal, jugular tuberculum, hypoglossal nerve hole and occipital condyle. EEA should be the first choice for lesions removal in this area. However, if the tumor extends laterally to this area, it does not mean that the EEA is a contraindication, but it is possible to increase the risk of damaging the neurovascular during the surgery that requires an experienced neurosurgeon or otolaryngologist to perform the procedure. For instance, when the tumor extends laterally to the optic nerve and lateral wall of the CS, even with carotid artery encasement, careful dissection and protection of the cavernous segment of the ICA is essential, as the rupture of ICA at this situation is often fatal, such as in one of our dead cases. This process would probably across the OCR, which would also go against KassamŌĆÖs philosophy : when possible, do not across the plant of CN [27]. With great care not to traumatize the lateral wall of CS as CNs (III, IV, V, and VI) situated at its inner aspect. If the anterior clinoid process has become an obstacle in the surgical field, endoscopic removal is also limited which may cause damage to the ophthalmic artery or/and CN III. Lateral extension of the chordoma at the level of the upper clivus and dorsum sellar requires a pituitary gland transposition superiorly with preservation of the pituitary stalk, which may affect the integrity and function of the pituitary gland, and not recommended by Gui et al. [12]. Lateral extension of the tumor at the level of the lower clivus even to the CVJ, the lateral extend is limited by hypoglossal nerve. The endonasal transpterygoid and transcondylar approaches provide access to the petrous apex, infrapetrous area, lateral and lower of the tumor. Maxillotomy and eustachian tube resection is necessary and it is an important landmark for the parapharyngeal ICA. When more than half of the occipital condyle was resected, occipitocervical fusion may be required which is not appropriate for this manipulation with endoscopy. In addition, the tumor size is also one of the reasons for limiting GTR with EEA when tumors with a diameter >4.0 cm or a volume >80 cm3 [10,18]. As the results of our series showed, the tumor diameter in the TLA group was significantly larger, which may be one of the reasons for the lower GTR rate than TMA or EEA.
TLA
Even though the EEA has many advantages and considerable GTR rates, TLAs are unable to be replaced completely up to now. Generally, the EEA and the lateral approach should complement each other, rather than substitute one for another. In a series of lateral approaches reported in the literatures, the GTR fluctuated. Such as reported by Colli and Al-Mefty [4], the total resection was 45.3% in 53 cases with skull base chordomas. Tzortzidis et al. [28] reported the GTR rate was 71.6% of their 74 patients. Gay et al. [11] achieved GTR in 47% of their 46 skull base chordoma patients. The merit of microscopic-assisted lateral approach is to make up for the insufficiency of EEA, especially for lateralized to the paramedian area or tightly involved the ICA, CS or have intradural extension with brainstem, vertebral and BA involved [4,23,28]. Furthermore, TLA is more suitable for extremely delicate manipulations than EEA, and allow safer dissection between the tumor and BA and brainstem [23]. The following TLAs are the most frequently used for skull base chordomas resection, alone or in combination : 1) Frontoorbitozygomatic approach. It is used for upper clivus lesions and extending laterally into the ICA, middle fossa, petrous apex, and provides excellent intradural access to the CS and intradural structures. However, the disadvantage of this approach is the limited visualization and does not address any bony infiltration, which may require a second approach to facilitate resection such as frontotemporal and/or transcavernous approach. 2) Subtemporal-infratemporal approach/Extended middle fossa approach. It provides a shorter access to middle skull base, petrous apex, upper clivus. It is an excellent approach to treat the lesions of infratemporal fossa and temporal fossa. When combined with the transpetrosal approach, clival chordoma that extends laterally to the petrous bone can be reached. And 3) extreme lateral transcondylar approach. It is used for chordomas involving the lower clivus, foramen magnum, occipital condyle, and extending laterally to the CVJ [24]. This approach facilitates the control of the VA and performed occipitocervical fixation if necessary, which is difficult to achieved by EEA.
Complications
CSF leak and CNs palsy are the most frequent postoperative complications [4,23,28]. CSF leak usually occurred in EEA owing to the dura was eroded by tumor or by the surgical approach occasionally and the persistent leak can cause predispose to intracranial infection and pneumocephalus. In most cases, multilayer skull base reconstruction with fat, fascia lata, and vascularized nasoseptal flap to plug the leakage and/or with lumbar drainage can significantly reduce the incidence of postoperative CSF leak. Excessive opening of the dura outside the tumor area should be avoided and only the eroded dura was opened to reduce the risk of CSF leak. On the other hand, working through spaces between CNs, the TLA may increase the likelihood of functional impairment (three of 12 cases in our series).
Tumor recurrence and radiotherapy
Regardless of the treatment modality, local recurrence of skull base chordoma is still common and affected by many factors, such as age, tumor location and size, the extent of surgical resection, postoperative radiotherapy, and tumor pathology and histological subtypes. Nevertheless, an aggressive surgical resection has been supposed to have a better prognosis [23,28]. In the meantime, advances in radiation technology have led to some consensus that radiation therapy in combination with surgery provides an additional advantage, consequently, adjuvant radiotherapy is recommended after surgery, even for inoperable patients [26,29]. In our study, the differences in median OS, median RFS, and median PFS may be due to the difference in follow-up time between the two groups.
There are some limitations in our research : this was a retrospective study, not all the surgeries were performed by the same neurosurgeon, and the concepts and the selection of surgical approach they are familiar with were different. Moreover, there were relatively few cases in the TLA group, which may lead to no statistical significance to some extent and the statistical differences in age between the two groups. Each patientsŌĆÖ data needs to be reevaluated after their 5 and 10 years during the follow-up.
CONCLUSION
Despite the management of skull base chordomas has changed from microscopic to endoscopic surgery gradually, a direct comparison between the two approaches is difficult, because there is no absolute boundary and both are essential for modern skull base surgeons. With the development of various surgical techniques, the combination of microscope-assisted lateral approach and EEA may further improve the GTR rate, which requires more researches on large number of patients. However, lacking of consensus on the optimal treatment for skull base chordomas makes treatment strategies varied from each center. A multidisciplinary collaboration of neurosurgeons, otorhinolaryngologists, and neuroradiologists is conducive to a comprehensive assessment of skull base chordomas.