INTRODUCTION
Child maltreatment is a major global public health challenge that involves various types of abuse and neglect, and it is one of the crucial risk factors of pediatric and adolescent psychopathology having severe consequences [8,9]. According to the federal definition of the Child Abuse Prevention and Treatment Act, child abuse and neglect is defined as any act, or failure to act, by a parent or caregiver (teacher, coach, and anyone who has an educational or caregiving role) that leads to physical or emotional harm, sexual exploitation or abuse, or death; or an act, or failure to act, which results in imminent risk of injury [9]. In children, the consequences of abuse and neglect can vary widely. A lack of understanding of serious lifetime consequences has hindered prevention policies and programs. Maltreated children are likely to develop psychiatric disorders such as major depression, anxiety disorder, posttraumatic stress disorder (PTSD), attention deficit hyperactivity disorder (ADHD), substance abuse, personality disorders, and psychosis over the course of their lifetime [35,38]. Therefore, it is important for clinicians to understand the etiology and risk factors of maltreatment in order to prevent and reduce victimization from abuse and neglect in children.
EPIDEMIOLOGY
Child maltreatment is a relatively common event, but identifying the real numbers of maltreated children is challenging owing to large variability. In a 2014 study by the US Department of Health and Human Services, 702000 victims of childhood abuse and neglect were estimated nationally; among them, approximately 75% of victims were neglected and 17% were physically abused. Moreover, 1580 children died of abuse and neglect at a rate of 2.1 per 100000 children in the national population [9]. Emotional maltreatment is difficult to estimate; however, conservative studies have estimated an occurrence of emotional maltreatment of approximately 8-12%. Sexual abuse estimation varies widely across countries. In 2002, World Health Organization reported that 73000000 boys and 150000000 girls less than 18 years of age were exposed to sexual abuse. Europe, America, and Asia had rates of 9.2%, 10.1%, and 23.9%, respectively, and Africa had the highest prevalence rate of 34.5% [9]. In Korea, according to a school-based report on the prevalence and risk factors of psychiatric disorders in children and adolescents in 2018, 37.8% of participants experienced some type of trauma, and psychiatric disorders were likely to occur with a 2-8-fold increased risk in traumatic participants [31]. For example, participants who have been diagnosed with PTSD and ADHD have a 2.3- and 3.6-fold higher risk of experiencing early childhood trauma than participants with no PTSD or ADHD, respectively [31].
According to a 2019 autopsy report from the National Forensic Service in Korea, 19 children died of abuse and neglect in 2014, accounting for a rate of 0.2 per 100000 in the national population. In addition, out of 341 autopsied children, 84 children (24.6%) died from maltreatment with clear evidence, 13 children (3.8%) died from possible maltreatment with clear documentation but insufficient evidence, and 51 children (15%) were strongly suspected to have been maltreated but there was a lack of evidence and information [15]. Among children and adolescents who died of maltreatment, 35.8% were infants, and 17.6% were children between 1 and 5 years of age. As the age increased, the death rate from maltreatment decreased, and this trend is matched with the patterns in the United States, France, the Netherlands, Australia, Canada, Germany, Italy, and Japan. The relationship between victims and perpetrators and the characteristics of perpetrators were also analyzed in the same autopsy report. It was shown that mostly the biological parents were involved with maltreatment; 57.1% of mothers and 29.1% of fathers, and 38.5% of biological mothers were less than 26 years old. These characteristics were similar to those of previous studies conducted by the Department of Education of England. Approximately 51.9% of perpetrators were unemployed, 24.3% were struggling with psychiatric illness, and 40.5% had financial difficulties [15].
TYPES OF MALTREATMENT
The types of maltreatment include active and passive maltreatment [35]. Active maltreatment comprises emotional abuse, physical abuse, and sexual abuse [35]. Verbal aggression, emotional manipulation, and witnessing domestic violence are examples of emotional abuse [35]. Physical abuse is a punishment that causes any kind of bodily harm, such as bruises, burns, fractures, and head trauma by acts of hitting, kicking, beating, shaking, burning, poisoning, and strangling [9,29]. Head injury may cause subdural hemorrhage, cerebral edema, hypoxic-ischemic injury, and retinal hemorrhages [29]. Sexual abuse is stipulated when an older child or adult forces a child to touch the perpetrator’s body, touches a child’s body, or forces a child to engage in any kind of activity with sexual contents [35,38].
Passive maltreatment is composed of emotional and physical neglect [35]. Neglect refers to when a caregiver does not provide care to meet a child’s basic needs. Emotional neglect is failure to meet a child’s basic emotional needs or being emotionally unresponsive to the child’s developmental level [35,38]. There are two types of physical neglect : failure to provide supervision and lack of supervision. The former is a failure to provide a minimum degree of care for a child’s basic physical needs, such as food, clothing, shelter, medical care, and hygiene [35,38]. The latter includes not providing adequate supervision to a child and not providing safe environments for a child [38].
RISK FACTORS
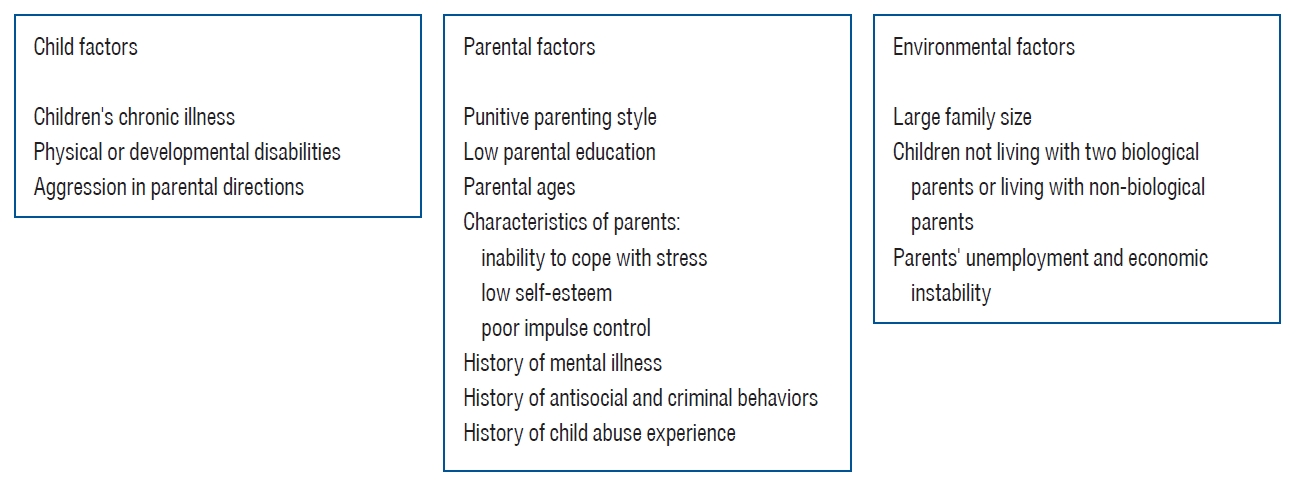
Analyzing risk factors is crucial for improving insight into the etiology of child maltreatment and preventing the recurrence of child abuse and neglect from a clinical viewpoint. Child maltreatment results from a complicated interaction between children, parents, caregivers, and environmental factors (Fig. 1). Child abuse and neglect could occur in children of all ages and diverse social and ethnic backgrounds, and multiple risk factors are involved in the occurrence of child maltreatment [28]. In addition, particular factors significantly influence maltreatment vulnerability. The conditions and characteristics that make it more difficult for parents to care for their children may affect the punitive parenting style. Examples include children’s chronic illness, physical or developmental disabilities, and aggression in parental directions. In particular, crying is a common trigger for abusive head trauma, and toilet training difficulties may result in immersion burns in response to encopresis or enuresis [28]. In a meta-analytic review regarding child abuse and neglect, 24 risk domains were reviewed and compared. Among them, large family size, children not living with two biological parents, low parental education, parents’ history of abuse, and parental age factors were the most significant domains that may affect child maltreatment [19]. In general, the strongest predictors of child maltreatment can be found in parental characteristics, such as inability to cope with stress, low self-esteem, poor impulse control, history of mental illness, and history of antisocial behaviors. Parental history of child abuse is also a significant risk factor, and it seems that children raised by parents who experienced abuse or neglect in their childhood are at risk of being a victim of child maltreatment [19]. Absence of a family support system places the child at an increased risk for maltreatment, and parents’ unemployment and economic instability are possibly associated factors. Children living with non-biological parents are at a significantly high risk of physical abuse, in addition to experiencing negative emotional, behavioral, and cognitive consequences from exposure to domestic violence [20,28]. It was shown that the most significant effects were found for parental and familial risk factors, and these risk factors should primarily be assessed when intervening and preventing child abuse and neglect. Lastly, since parental history of antisocial and criminal behaviors and psychiatric problems are among the relatively severe factors, it is important to keep track of the status of parents and families during case management in a social context [9,19].
ASSOCIATED PSYCHOPATHOLOGY
Maltreated children are more prone to depression, anxiety disorder, PTSD, behavioral problems, suicidal attempts, and substance use problems than non-maltreated children [5].
Major depressive disorder
Depression is a common consequence of childhood maltreatment. In the USA, the 12-month prevalence rate of depression is approximately 7%, while the depression rate of maltreated individuals is estimated to be approximately 24.7% [5]. Previous studies have shown that experiencing any form of maltreatment is associated with more than a 2-fold increase in the risk of depression in adulthood and with the development of chronic and recurrent depression [13,35]. It was suggested that the risk of depression increases in a graded, dose-dependent manner with the number of maltreatment experiences of children. In addition, depression has a much earlier onset age (between ages 5 and 10) in maltreated children than in non-maltreated youth [5]. Maltreatment increases the risk of depressive disorder in both men and women, although some studies have shown that physically abused females have a greater risk for depression than physically abused males [25]. Another clinical significance between maltreated and non-maltreated children is that depression emerges earlier and has a more sustained course in maltreated children. These children have more severe and unstable mood, neurocognitive symptoms, and more comorbidities, such as anxiety disorder and substance abuse. Psychotic symptoms are also more common, as are self-harm and suicide attempts [35]. Exposure to one or more maltreatment experiences accounted for 67% of suicide attempts [6]. Considering the types of maltreatment, it has been shown that all types of maltreatment are associated with significantly higher rates of depression and a greater risk of meeting the criteria for major depressive disorder. However, emotional abuse and emotional neglect have the strongest association with depression, whereas sexual and physical abuse and neglect have a weaker association with depression. In addition, the effect of emotional abuse on depression is greater in children and adolescents than in adults [13]. It means that a more silent form of maltreatment (emotional abuse and emotional neglect) is most strongly associated with depression. Compared to physical and sexual abuse, emotional neglect and abuse seem to be uniquely associated with anhedonic symptoms of depression and vulnerability to developing a negative cognitive style, which may increase the risk of depression [13]. This finding is helpful in approaching maltreated children with depressive disorder by building insights concerning the etiology of depression and setting treatment targets.
The treatment of depression in maltreated children is similar to that in any patient with depression, but some important factors should be considered. During the initial evaluations, assessment of child maltreatment and other stressors, family support, and familial conflicts should be conducted because these factors can contribute to the persistence of depression [5]. Depressive maltreated children also differ in treatment response. In depression outcome studies, childhood maltreatment showed poor treatment outcomes in patients with depression [22]. Therefore, medications, psychotherapy, or interpersonal therapy, including learning cognitive and behavioral strategies to manage ongoing stressors, should be combined to prevent recurrence and manage severe symptoms such as suicidality.
Anxiety disorder
Anxiety disorders are one of the most common psychiatric disorders in children. Approximately 7.1% of 3-17-year-old children were diagnosed with anxiety disorder [10], and it increased from 5.5% in 2007 to 6.4% in 2011-2012 among children aged 6-17 years [1]. However, there are few studies on how childhood adversity affects symptoms and treatments associated with anxiety disorders. Maladaptive family functioning, including family violence, physical abuse, sexual abuse, and neglect, was significantly associated with increased odd ratios (ORs; 1.6, 1.6, 1.9, and 1.6, respectively) in anxiety disorder, and childhood adversity was estimated to be responsible for 32.4% of the population-attributable risk for anxiety disorders [11]. Childhood sexual abuse was associated with social anxiety disorder, panic disorder, generalized anxiety disorder, and PTSD, while physical abuse was only associated with PTSD and specific phobia in a study using data from the National Comorbidity Survey-Replication [4]. The severity of anxiety was related to emotional abuse, emotional neglect, and sexual abuse [33]. Patients with anxiety disorder and a history of childhood trauma have significantly higher rates of concurrent major depressive disorder and a much more chronic course than those without [12]. In addition, they experience more significant impairment in social functioning [17], greater symptom severity, and poorer quality of life [32].
PTSD
PTSD includes three core symptoms of re-experience, avoidance, and negative alterations in cognition and mood after experiencing traumatic events [3]. Direct exposure to sexual or physical abuse and witnessing violence against family members during childhood meet the criteria for trauma that can lead to PTSD. Lifetime prevalence of PTSD increased by 4.9 times in those who experienced childhood maltreatment compared to those who did not in a prospective cohort study [30]. PTSD patients with a history of childhood abuse displayed different characteristics from their counterparts. Exposure to multiple traumas in childhood was related to higher PTSD symptom complexity [2], increased comorbidity of depression and suicidal behavior [2], and severe dissociated symptoms [21].
Illicit drug use/substance abuse
The impact of childhood maltreatment on the development of substance abuse and illicit drug use has been well documented. Dube et al. [7] reported that childhood abuse, neglect, and household dysfunction increased the risk of early drug initiation and illicit drug use in the Adverse Childhood Experiences (ACE) Study. The likelihood of initiation of illicit drug during early adolescence was found to increase by 40%, and the ACE score was associated with an increased risk of having a drug problem, drug addiction, parenteral drug use, and illicit drug use in a dose-dependent manner [7]. In a recent meta-analysis, significant associations were observed between child physical abuse, emotional abuse and neglect, and substance use disorders (physical abuse : OR, 1.92; 95% confidence interval [CI], 1.67-2.20; emotional abuse : OR, 1.41; 95% CI, 1.11-1.79; and neglect : OR, 1.36; 95% CI, 1.21-1.54) [25]. A well-designed female twin study found that childhood sexual abuse was positively associated with alcohol and other drug dependence with ORs of 2.8 to 3.1, which were higher than the ORs of major depression, general anxiety disorder, and panic disorder (all approximately 1.9), and the ORs were higher for genital-related sexual abuse than non-genital abuse [14]. Patients with substance abuse disorder or illicit drug users with a history of maltreatment tended to have greater rates of psychological distress [18], greater risks for incarceration and suicide attempt [36], consistently higher scores on substance use frequency and substance problems [37], and poorer response to treatment [27].
TREATMENT
In general, there is no “special” treatment for childhood trauma in patients diagnosed with mood disorders, anxiety disorders, or substance use disorders. After thorough evaluation, drugs such as antidepressants, mood stabilizers, antipsychotics, and non-pharmaceutical interventions, including cognitive behavioral therapy (CBT), interpersonal psychotherapy, and psychoeducation, could be administered to the patients according to their psychiatric diagnosis and symptoms. However, patients with histories of abuse and neglect have been consistently shown to have a poorer treatment response than their non-maltreated counterparts with the same the Diagnostic and Statistical Manual of Mental Disorders-V-based psychiatric diagnosis [22,24]. Depressed patients with childhood maltreatment were reported to have a lower remission/response rate or longer time to remit following psychotherapy, pharmacotherapy, and combined treatment [22,23], suggesting that the standard first-line treatment options for depression may not be effective for these populations [34]. In contrast, some studies reported more beneficial effects in patients with childhood adversity. Adults with chronic depression and early life stress had a more favorable response to the Cognitive Behavioral Analysis System of Psychotherapy than those without early life stress [24], and intravenous ketamine had a better outcome in participants with refractory depression and childhood maltreatment [26]. For sexually abused children with PTSD symptoms, trauma-focused CBT has shown the highest effectiveness, but the long-term evidence is insufficient [16,35]. Mentalization-based therapy may be effective in patients with insecure attachment patterns across a wide range of mental disorders such as major depressive disorder and personality disorder, and integrative therapies for combined substance dependence and trauma-related symptoms have been developed for maltreated substance abusers [35].
CONCLUSION
Childhood maltreatment is a complex global clinical issue that needs to be actively studied with more attention. Mental illness is among the most salient consequences of child abuse and neglect [38]. Abused and neglected children are more likely to experience psychiatric disorders such as major depressive disorder, anxiety disorder, PTSD, and substance use disorders, and early intervention for these mental illnesses is critical for better outcomes. Therefore, it is important for clinicians to understand the risk factors, etiology, and clinical presentations of childhood maltreatment, and to be aware of these issues when observing suspicious incidents.