INTRODUCTION
The biggest problem faced by local hospitals in rural and underserved areas is the difficulty in securing high-quality medical staff to treat acute and severe diseases. Due to the lack of neurosurgeons available for treating intracerebral hemorrhage (ICH), most critically ill patients with ICH at local hospitals in rural and underserved areas are transferred to regional emergency centers. ICH is a serious acute neurological illness due to the rupture of cerebral vessels. It occurs in approximately 20% of all stroke patients in Korea [8]. However, about 40% of ICH patients die within 30 days after the event, and only 20% of them can live independently 6 months after ICH development [2,8,18]. The number of adult ICH patients showed a relative decreasing trend from 18211 in 2008 to 16174 in 2016 [15]. However, despite improvements and infrastructure expansions for emergency patient transportation over the past 10 years in Korea, the number of annual deaths due to ICH remained unchanged from 2939 in 2012 to 2578 in 2020 [5]. Although there are no national data, a multicenter study revealed that the costs for ICH patients in the first year was 13090179 won, which is much higher than that of ischemic stroke patients (5460459 won) [21]. Considering indirect costs, such as the loss of labor due to disability, it is estimated that the actual social and economic loss is 10 times higher than the estimated direct cost. Mortality due to cardiovascular diseases, including ICH, exhibited regional disparity between metropolitan and non-metropolitan areas [10]. Therefore, it is necessary to develop a system to address medical inequality in treating ICH patients at the national level, not at the level of doctors or hospitals.
Since the coronavirus-19 (COVID-19) pandemic, non-face-to-face technologies and services, also called telemedicine, have been expanded to various fields of medicine. And telemedicine will be more available in various medical departments in Korea in the future than it is now. Currently, most telemedicine platforms are for patients with chronic or infectious diseases. Previous studies revealed that telemedicine was a safe and ideal expert support system during infectious outbreaks [7,20]. This technology makes high-quality medical procedures possible, limits potentially contagious interhospital transfers, saves critical resources, such as protective gear and rescue and emergency transport services, and offers safe home office work for clinicians [7,11,17,20]. COVID-19 has also led to changes in the laws, including data privacy protection and financial reimbursement, that previously made it difficult to implement telemedicine. Considering these changes in the medical and social environments, neurosurgeons should be especially interested in applying telemedicine technology to severe patients with severe intractable diseases.
An emergency transfer and cooperation system for critically ill patients has been well-established in Korea. However, the system has mainly focused on inter-hospital transfer. Neurosurgeons are not primarily involved in this transfer system. Thus, it is difficult to link the system to the rapid diagnosis of ICH and subsequent prompt treatment. In particular, only when a neurosurgeon is involved in the treatment of a patient with ICH from the beginning, can transfer to a suitable hospital, intensive care unit, and operating room be accomplished. Therefore, we believe neurosurgeons should collaborate to develop a new telemedicine platform for ICH patients who live in rural and underserved areas.
CONCEPT
Limitations and countermeasures for ICH in Gangwon-do
Gangwon-do is the second largest region in Korea after Gyeongsangbuk-do, and about 80% is comprised of mountains. Four university hospitals in Gangwon-do can perform emergency surgery for ICH patients at any time. The surgical management of ICH patients is rarely performed by neurosurgeons in general hospitals. Accordingly, it is practically difficult to diagnose and treat acute ICH occurring in patients in rural and underserved areas. To efficiently treat acute ICH patients in Gangwon-do, it is necessary to divide Gangwon-do into three regions, Chuncheon city, Wonju city, and Gangneung city, and to create a respond network between regional university hospitals and local hospitals in rural and underserved areas. In the establishment of such a network, a nonface-to-face cooperation platform that uses artificial intelligence (AI) is needed for effective management. A problematic issue in clinical practice is whether the fast and accurate reading of a computed tomography (CT) scan taken of a patient with a neurological abnormality is possible. Also, if ICH is diagnosed, it should be treated promptly without delay. Since no neurosurgeons who can manage ICH are available at local hospitals in rural and underserved areas, the development of a new telemedicine platform using AI for the automatic detection of ICH and remote collaboration technology with neurosurgeons at regional university hospitals is necessary.
Need for cloud-based telemedicine platform development
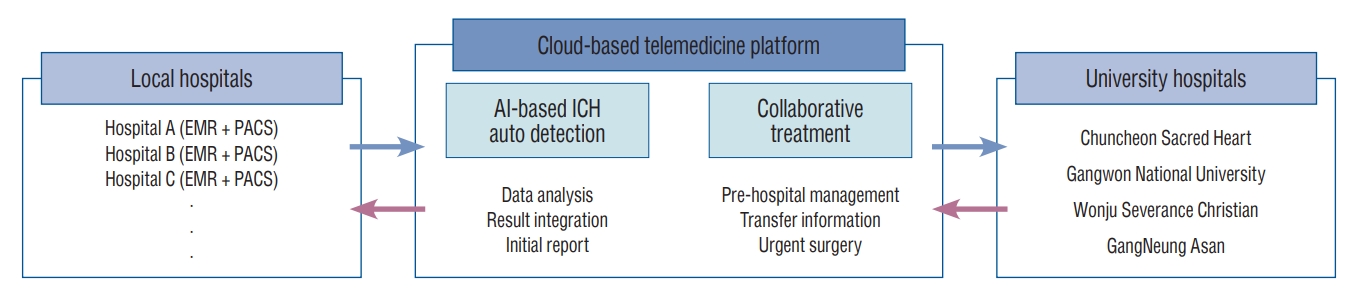
A non-face-to-face remote collaboration system simply using AI medical devices has the following disadvantages for use in real clinical practice. First, each picture archiving and communication system (PACS) at each local hospital should be individually equipped with AI software. The second problem is that when the number of participating hospitals increases in the future, it will be difficult to expand the cooperative individual network between local hospitals and university hospitals providing professional consultation. Third, if only the automatic detection of ICH is provided, the patientвҖҷs prognosis will not be improved. For neurological recovery, prompt and appropriate treatment, as well as early diagnosis, are required. However, this connection between automatic detection and ICH treatment is impossible without the cooperation of neurosurgeons. To overcome these limitations, a new dedicated cloud-based telemedicine platform for ICH should be developed. First of all, if the cloud server is equipped with an AI solution, there is no need to individually install AI software on the PACS in each local hospital. It is also advantageous for network expansion when the number of participating hospitals increases. Lastly, the most important thing is that the platform can allow neurosurgeons working in several university hospitals to participate in patient treatment early after an ICH (Fig. 1 and Supplementary Fig. 1).
PROTOCOL
We intend to proceed with telemedicine platform development in two phases. The first phase will be from April 2022 to December 2023, and the second phase will be from April 2024 to December 2025. We plan to develop a platform by dividing the work of neurosurgeons and information technology (IT) experts by setting the order of items through mutual feedback. The role of neurosurgeons in the first phase is as follows. First, neurosurgeons will standardize collaborative care for the telemedicine-assisted treatment of ICH patients and optimize it for clinical use. Second, a non-face-to-face collaboration system and AI dedicated to ICH should be evaluated in connection with the electronic medical record (EMR). In the second phase, neurosurgeons will evaluate the stability and effectiveness of the cloud-based telemedicine platform with participating hospitals including local hospitals in rural and underserved areas and university hospitals in Gangwon-do. Software capability and network stability via real-time collaboration between medical staff or hospitals will be evaluated and completed (Supplementary Fig. 2A). IT experts have the following goals during the first phase. First, it is the planning and design of a multilateral telemedicine collaboration platform. This work includes the use of video calls and secure messages via an EMR connection. Also, applications that provide the web browser-based uploading and downloading of medical information (e.g., radiological images, signal data, and text) and android-based mobile capability will be developed. The second is the interlocking of an AI-based automatic ICH reading system for use in a cloud environment. In the second phase, IT experts are expected to verify and improve the performance of the cloud-based telemedicine collaboration platform while treating ICH patients in the actual medical field. Problems identified through the testing of the cloud-based collaboration platform will be resolved. Finally, the function, performance, security, and safety of the telemedicine platform will be checked through an accredited certification authority. All descriptions were approved by the Institutional Animal Care and Use Committee of the participating university (approval No. 2022-11-003). This study was performed in accordance with the relevant guidelines.
DISCUSSION
ICH does not have a golden time, a time in which it must be diagnosed, and treatment must be delivered. It is an вҖңas-soon-as-possibleвҖқ disease that should be diagnosed and treated quickly. The rapid detection and treatment of ICH must be performed simultaneously to minimize neurological complications. However, the reality is that there are few doctors who can accurately interpret CT scans at local hospitals in rural and underserved areas. Even if such clinicians are available, if a CT scan is taken at night, ICH detection will inevitably be delayed. Thus, AI-based automatic detection software helps doctors who do not specialize in brain disorders to diagnose. However, the more important issue is whether treatment can be delivered promptly, immediately after ICH detection. Even in patients diagnosed with the same acute ICH, treatment methods (surgery vs. medical treatment) and the type of surgery vary depending on the amount of bleeding, the location of the occurrence, timing of ICH (acute, subacute, and chronic phase), and the presence of intraventricular hemorrhage and hydrocephalus. Also, when it comes to medical treatments, it is very difficult for non-neurosurgeons to decide how far to lower blood pressure, whether it is necessary to reverse anticoagulation effects, and select a drug to reduce cerebral edema [18]. About 20% to 40% of patients experience an increase in the ICH amount, and this hematoma expansion is a significant risk factor for poor neurological outcomes [16]. Hematoma expansion is most common within the first 6-24 hours and can occur up to 48 hours in coagulopathic patients [9,19]. Also, the prognosis of patients may differ depending on the type of ICH they experience. Patients with lobar ICH experienced more hematoma expansion and early neurological deterioration compared to those with deep-seated ICH [4,13]. Thus, the treatment of ICH patients at local hospitals in rural and underserved areas should be done based on professional consultation with neurosurgeons at a university hospital from the event onset. Through this project, we will establish an ICH treatment network in Gangwon-do. In this dedicated ICH telemedicine platform, neurosurgeons can actively participate in pre-hospital management. The ICH telemedicine platform we are going to develop is different from mobile stroke units (MSUs). Cooley et al. [6] reported that ICH patients with MSUs had faster onset-to-scene-arrival time than those without MSUs. Also, more ICH patients visited to a comprehensive or neurosurgical center, not a primary center, than those without MSUs. In their study, antihypertensive management was mostly performed, followed by airway management [6]. Patients in Korea have better access to medical care than those in Europe or Australia, so if a neurological abnormality occurs, a CT scan is performed at a nearby medical center. Accordingly, our goal is not simply to decide whether to prescribe drugs in a moving ambulance but to make ICH treatment efficient by linking diagnosis and treatment in rural and underserved areas. Further, our platform will be used in areas other than Gangwon-do, such as Jeju Island. Jeju Island also lacks professional clinicians. Currently, it is difficult to recruit neurosurgeons, even at the Jeju National University Hospital. In simple terms, a high salary can bring a neurosurgeon to a hospital in rural and underserved areas, but in practice, it is difficult to sustain the system. Thus, in reality, it is best to effectively utilize neurosurgeons at a university hospital for managing ICH patients in rural and underserved areas. We believe that our telemedicine platform, which is based on consultation with neurosurgeons at university hospitals, will effectively treat ICH patients anywhere in Korea.
AI used in the cloud-based telemedicine platform will provide automatic ICH detection using non-contrast CT images. The clinical efficacy of automatic ICH detection using various deep-learning algorithms has been increasingly reported [3,14,22]. Arbabshirani et al. [3] showed a convolutional neural network (CNN) algorithm with an area under the receiver operating curve (AUC-ROC) of 0.846 (0.837-0.856) for detecting ICH. Lee et al. [14] proposed an AI-based ICH detector without employing a CNN with an AUC of 0.859. Although the overall diagnostic accuracy rate of ICH was over 90.0%, the detection rates for specific ICH subtypes, such as subdural hemorrhage or subarachnoid hemorrhage, were 69.2% and 77.4%, respectively [22]. Thus, neurosurgeons need to double-check an ICH diagnosis rather than relying entirely on AI. In the future, through the updating of AI algorithms, we plan to further develop the system to automatically interpret the results of angiography images, in addition to non-contrast CT images [1,12].
Since our cloud-based telemedicine platform focuses on pre-hospital treatment, it needs to be linked to the management of ICH survivors. The prevention of ICH recurrence or ischemic strokes is also important for ICH survivors. Thus, IT devices, such as a mobile medical assistant, could be helpful for the efficient management of ICH survivors (Supplementary Fig. 2B). Through this, ICH survivors can actively participate in managing co-existing metabolic disorders, such as hypertension, diabetes mellitus, and atherosclerosis as well as receiving important information from the doctor at the same time. In addition, caregivers living outside of Gangwon-do will be able to access the patientвҖҷs treatment information, current status, and future plans. Therefore, there is a possibility of treating ICH patients more effectively when considering Gangwon-doвҖҷs entry into a super-aging population.
CONCLUSION
This article aimed to provide information on our research project to develop a cloud-based telemedicine platform for acute ICH patients in Gangwon-do. We believe that the cooperation of neurosurgeons in Gangwon-do will cause a paradigm shift in the pre-hospital treatment of ICH patients who live in rural and underserved areas.