INTRODUCTION
Stereotactic biopsy using the Leksell frame is a procedure performed under local anesthesia that enables rapid diagnosis with increased stability and proven effectiveness over decades. Theoretically, this diagnostic tool can be directed to any location in the brain, including brainstem tumors, as reported in the literature [1,5,7,10,13-16]. In the case of supratentorial tumors, the operator can obtain a wide field while the patient is comfortable in the supine position. However, conventional methods of infratentorial lesion biopsy have several limitations. Unlike supratentorial tumors, biopsies of infratentorial tumors, including those involving the brainstem, necessitate excessive neck flexion in the patient and lowering of the frame to the base of the skull for adequate surgical exposure. Consequently, patient discomfort and increased burden for the operator must be carefully considered during posterior fossa biopsies.
Therefore, a methodology adept at overcoming these restrictions and delivering reliable results was previous published [9]. The aim of this study is to provide detailed practical guidance and considerations for obtaining adequate tissue samples from deep-seated cerebellar lesions or lower brainstem lesions specifically those accessible via the cerebellar peduncle, drawing upon previous research and the author’s expertise.
MATERIALS AND METHODS
Operative technique : practical tips and considerations
The study protocol was approved by the Institutional Review Boards of Chonnam National University Hwasun Hospital (H2023-0140). All patients included in this study have given their written informed consent.
Tip 1. Leksell coordinate frame G fixation
1) to avoid the anterior screw from being implanted within the temporalis muscle, 2) to prevent any interference with the magnetic resonance (MR)-adapter, and 3) in close proximity to the tentorium, taking into account the magnetic field of MR imaging (MRI).
First, the insulated fixation posts must be fixed upside down (Fig. 1A). The anterior fixation screw, due to its downward angulation, may penetrate too deeply into the temporalis muscle. It may not achieve adequate fixation due to the presence of the temporalis muscle, and the thinness of the temporal bone requires heightened attention during fixation (Fig. 1B). Noteworthy that since the MR-adapter is mounted above the Leksell coordinate frame G. To optimize the MRI signals for infratentorial lesions, the Leksell coordinate from G should be positioned on the supratentorial side, close to the tentorium. When securing the posterior fixation screw, ensure that the inferior side of the insulated fixation post is set to the shortest length to avoid collision with the MR-adapter for MR imaging acquisition. Even a slight increase in length may lead to inaccuracies in mounting the adapter on the frame.
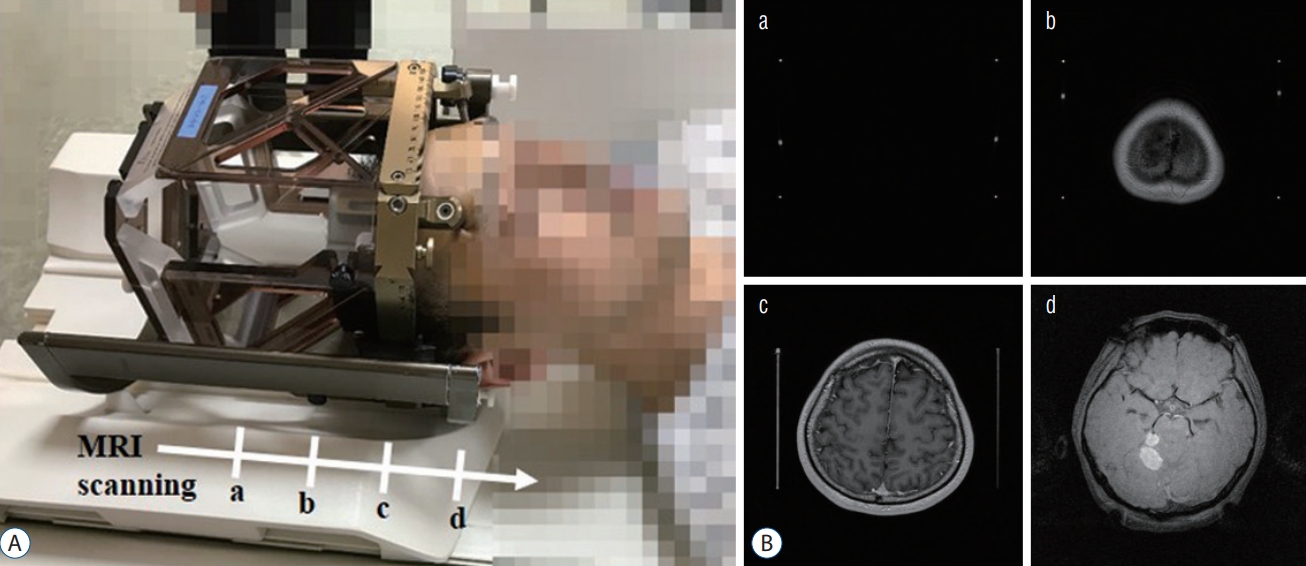
Tip 2. Mounting of indicator box and acquisition of magnetic resonance imaging
The MRI evaluation should encompass both the indicator box and the infratentorial region that deviated from it.
As shown in Fig. 2A, the MR-Indicator box is positioned on top of the head, the MR-adapter is secured, and the MRI scanning is conducted. Stereotactic MR images are acquired using a SIGNA EXCITE 1.5T MRI scanner (GE Healthcare, Chicago, IL, USA) equipped with a 275 mm inner diameter Quadrature Head Coil (GE Healthcare). The imaging isocenter is situated at the lower portion of the frame, precisely at the level represented in c of Fig. 2. The MRI evaluation should encompass both the indicator box and the infratentorial region that deviated from it (Fig. 2B). Noteworthy that the signal may be weak in the areas outside the indicator box due to the distance from the magnetic field. Before biopsy planning, confirm that the target location is identifiable on MRI scans.
Tip 3. Calculation of targets
A significant difference from the classic method is that the Leksell Vantage Z-scale on both sides is reversed and mounted. Therefore, it is necessary to convert the existing coordinate calculation method. The study by Horisawa et al. [9] explains the principle of correcting the Z value for this method. We refer to this report to make it simpler.
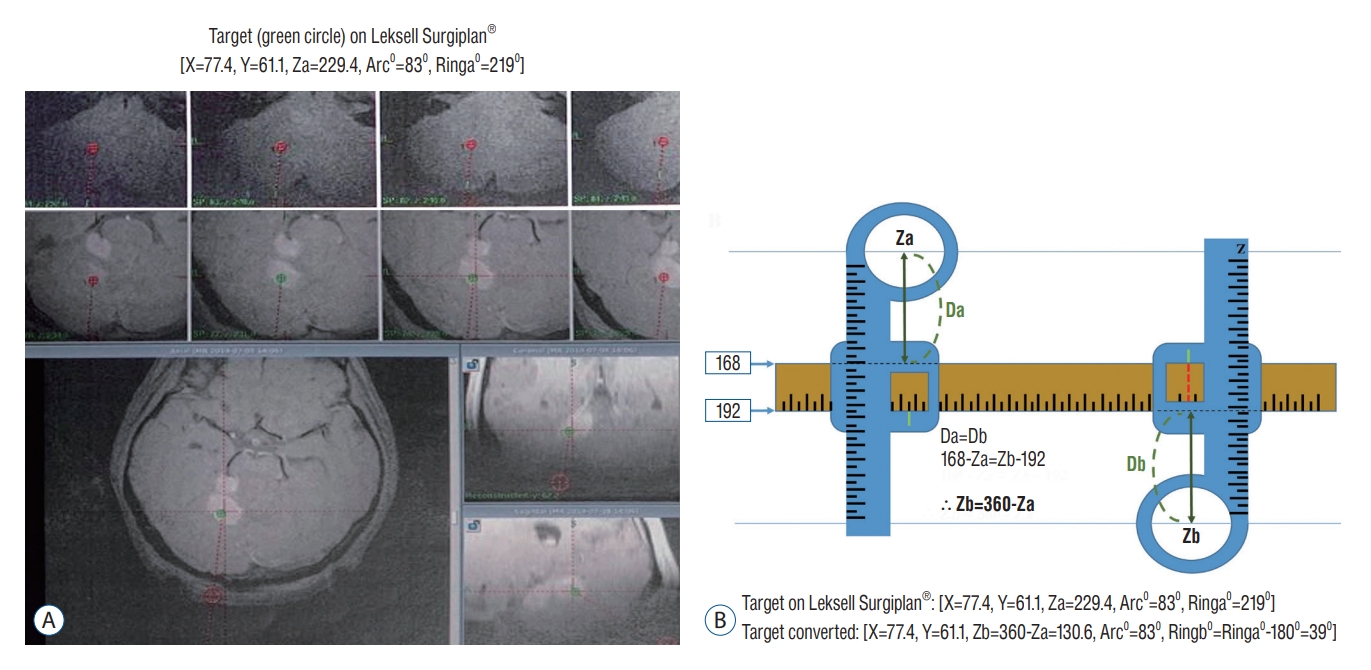
First, the [X, Y, Za, Arc0, Ringa0] coordinates of target points can be calculated using Leksell SurgiPlan® software (Elekta, Stockholm, Sweden), with arc 00 located on the patient’s right side (Fig. 3A). Fig. 3B explains the calibration. In the program, the upper and lower values of the Leksell vantage Y scale are fixed at absolute values of 168 and 192, respectively. Using this, even when the phase is inverted, the distance from the center of the Z scale ring to the Y scale is the same (Da=Db). This distance is always the same for any arbitrary target. Accordingly, the conversion expression of the Z coordinate (Za : Z coordinate on Leksell SurgiPlan®, Zb : Z coordinate calibration for operation target) Da=Db; 168-Za=Zb-192; Zb=360-Za can be obtained.
Using this conversion, we converted the coordinates obtained from the program to [X, Y, Zb=360-Za, Arc0, Ringb0=Ringa0-1800]. The calculated arc0 using Leksell SurgiPlan® remained the same, but the Ringb0 was calculated by subtracting 1800 from Ringa0.
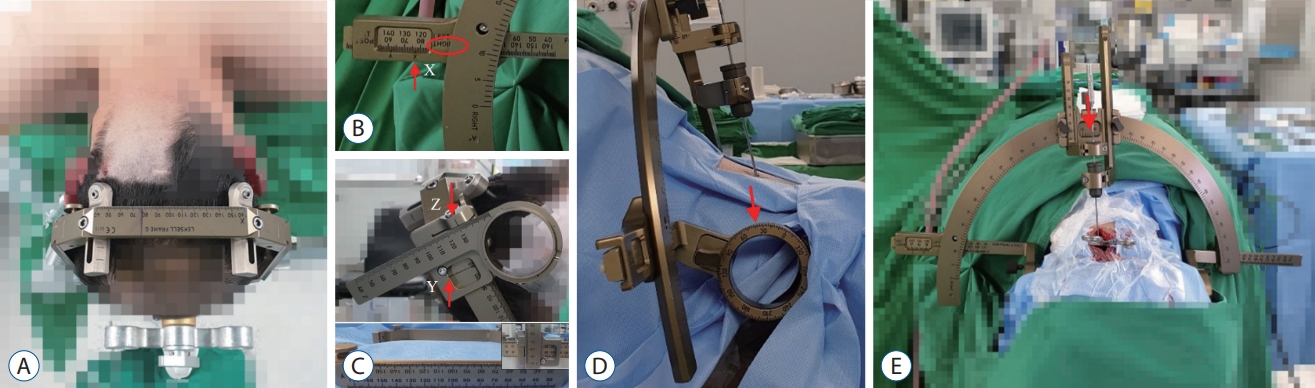
Tip 4. Surgical procedures with calculation targets
The operation was performed with the patient in the prone position under general anesthesia (Fig. 4A). There was no structural obstruction for access to the infratentorial lesion, and a wide surgical field was secured without excessive neck flexion in the patient. The converted coordinates were adjusted to the graduations of each scale (Fig. 4B and C). Noteworthy that since the coordinate slide is also installed inverted, the scale of the Y coordinate is hidden; therefore, it must be extended and drawn in advance before installation. The coordinate slide can be adjusted even if mounted upside down as long as the sticker scale is visible using an adhesive-laminated label printer tape (Brother®; Brother Industries, Nagoya, Japan). The sticker must be thin enough to avoid any interference with the movement of the coordinate slide. The Ringb0 was calculated by subtracting 1800 from Ringa0 (Fig. 4D). The calculated Arc0 using Leksell SurgiPlan® remained the same (Fig. 4E). The operator comfortably obtained the specimen in a stable position.
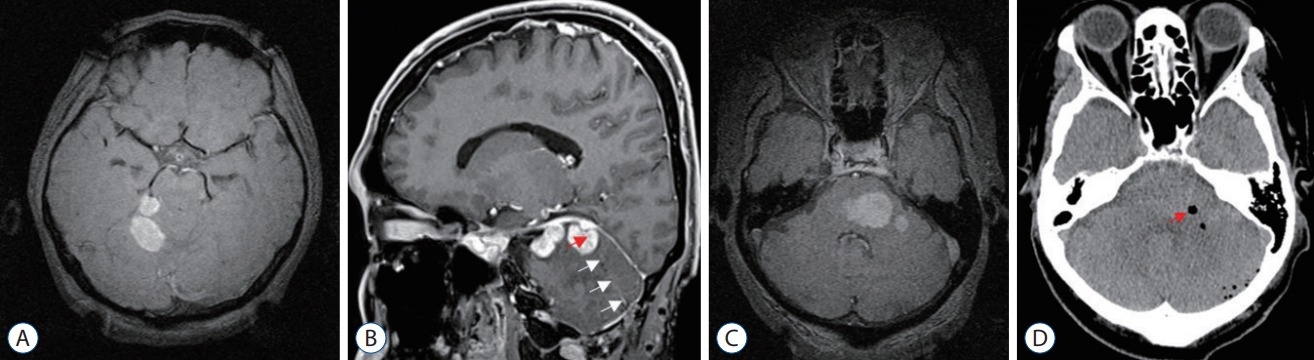
The frozen biopsy confirmed the targeted lesion. In case 1, the trajectory for deep cerebellar mass was verified on a brain MRI after surgery, and the biopsy needle reached the target as planned (Fig. 5A and B). In case 2, air was confirmed in the brain stem tumor where tissue was obtained on brain computed tomography (Fig. 5C and D). The tumors were diagnosed as diffuse large B-cell lymphomas.
RESULTS
Patient information is summarized in Table 1. In four cases with deep cerebellar (n=3) and brainstem (n=1) tumors, biopsies revealed two cases of diffuse large B-cell lymphoma, one metastatic brain tumor and one glioblastoma. In one patient following the position of the Leksell frame, the lesion was found beyond the effective range of the magnetic field during brain MRI. Therefore, the frame was subsequently readjusted downward to optimize alignment for imaging purposes. There was any other complication during the biopsies. We presented a comprehensive overview of practical tips and considerations based on case 1, for which a biopsy for deep cerebellar tumor was performed as the target.
DISCUSSION
The stereotactic brain biopsy using the Leksell system is widely used by neurosurgeons for its simplicity and reliability. This method can be quickly and safely performed under local anesthesia for supratentorial lesion biopsies but requires more preparation and effort for subtentorial lesions, including the brainstem.
In a previous study, it was reported that the supratentorial approach is preferred for lesions located in the cephalic portion of the brainstem, such as the midbrain. In contrast, the infratentorial transcerebellar approach is employed for lesions located in the caudal portion of the brainstem, including the medulla oblongata and cerebellar peduncle [10]. Generally, when using MRI guidance, approaches to the brainstem through the transfrontal lobe and transcerebellar trajectory often result in deviation. Giese et al [6]. reported an average deviation of 2.2-1.18 mm and an average distance of 85.9±4.7 mm when using transfrontal trajectory, while the suboccipital trajectory resulted in an average deviation of 1.81-0.7 mm and an average distance of 59.5±4.1 mm in cadaver studies. Therefore, a transcerebellar approach is preferable to ensure a precise and safe biopsy of infratentorial lesions. However, there are certain limitations in performing tissue biopsy using the Leksell system for the transcerebellar approach. Consequently, this study primarily focused on surgical indications for deep-seated cerebellar lesions or lower brainstem lesions specifically those accessible via the cerebellar peduncle.
When performing a biopsy of an infratentorial lesion using a transcerebellar approach, the structure of the Leksell system can pose limitations, which can be addressed by placing the Leksell coordinate frame G as low as possible and securing the surgical field by maximizing neck flexion. This approach has been described in several studies [1,5,7,10,13-16] with successful results, but there are cases where navigation-guided biopsies are necessary due to limitations. However, this traditional method can cause pain and discomfort to the patient (due to excessive neck flexion), discomfort for the surgeon, and limited surgical field access due to the posterior insulated fixation posts. These limitations are particularly burdensome during local anesthesia.
To overcome challenges, we carried out multiple biopsies following the techniques described by Horisawa et al. [9]. This study aims to provide practical guidance and considerations for securing adequate tissue samples, based on our detailed trial-and-error experiences and previous research. When performing surgery, there were several practical tips to consider. When placing a fixation post, it is important to consider the angle of the anterior screw, which screw to penetrate deeply into the temporalis muscle. During posterior screw fixation, there are two key points to consider. First, the portion of the fixation post below coordinate frame G should be minimized to mount the MR-adapter above the coordinate frame G. Second, to ensure the maximum MRI magnetic field from the adapter to the infratentorial lesion, it should be fixed in the lowest possible position while considering the surgical field (Figs. 1 and 2). If it is difficult to identify lesions in Leksell SurgiPlan® software, the coordinates of the target cannot be calculated; therefore, it must be checked before completing the MRI scan. One patient required frame repositioning to find the lesion.
In this study, while there could be concerns about MR distortion for lesions outside the magnetic field, we strategically positioned the imaging isocenter at the lower part of the frame, specifically at the level depicted in c of Fig. 2A. This was to minimize any potential magnetic resonance distortion issues even if the outside magnetic field might exhibit less strength at the site of the lesion. Additionally, since the lesion site is within 150 mm from the isocenter, we do not consider significant distortion a critical concern. As previously published data, there’s an observed increase in the distortion of 1.5 T and 3 T MRI images in proportion to the distance from the imaging isocenter within the radiofrequency coil [12]. For a region of interest with a radius of 100 mm centered at the isocenter, the mean distortion magnitude across all MRI scanners is 0.44±0.18 mm. Additionally, the maximum distortion fluctuates from 0.52 to 1.31 mm, contingent on the specific MRI scanner used. The distortion can extend up to 2 mm at a distance of 150 mm from the isocenter.
Coordinate conversion was simplified using the absolute value of the edge of the coordinate frame G recognized by SurgiPlan® software. Even if the phase of the coordinate Z-scale is changed, considering that the distance from the center of the ring to the coordinate frame G is the same, eventually leads to the same conclusion as reported by Horisawa et al. [9] report. This method in Fig. 3 is easier and simpler to understand. We successfully performed biopsies in four patients using this conversion formula. When fixing the coordinates of a target lesion, the coordinate slide is installed upside down, covering the scale of the Y coordinate, thus requiring the existing scale to be extended in advance for accurate drawing (Fig. 4C). To omit this work, we made a reusable sticker scale using an adhesive-laminated label printer tape (Brother®; Brother Industries) that maintains strong adhesive properties and does not deform even after sterilization with low-temperature ethylene oxide gas. This sticker was thin enough to avoid any interference with the movement of the coordinate slide.
Installing stable support to fix the Leksell system in a sitting position for the patient was challenging. The operator found it difficult to approach the patient from behind as they were seated with their heads bowed. Moreover, the operator was unfamiliar with adjusting the height and distance for the approach. Due to these difficulties, we determined it would be difficult to complete the surgery stably and efficiently within a short period. Therefore, we changed the patient’s position to prone under general anesthesia and waited for the confirmation of the frozen biopsy result for the specimen obtained during surgery. The concern of air embolism associated with the sitting position was eliminated [17]. The operation proceeded smoothly in the familiar prone position, and above all, the stable installation of the Leksell system on the bed, the wide surgical field, and the comfortable posture of the operator were significant advantages.
With advances in medical equipment technology, a navigation-guided or frame-less biopsy is widely used [2-4,8,11,18]. This method offers several advantages, such as real-time correction, error control in surgery, and the ability to simulate the procedure beforehand, regardless of time and place [2-4]. Such simulation allows for a more precise tract setting while avoiding critical structures. Instruments such as robot arms eliminate operator tremor, reduce errors, and minimize fatigue from repetitive tasks [4,11]. Biopsy through the transcerebellar track can also be performed with the patient in a lateral position [3,4]. However, the cost of preparing and managing the medical equipment and equipment control needs consideration. Contrarily, this method uses the existing Leksell system in the same process and time as traditional stereotactic biopsy, with the option for general anesthesia for patient and operator convenience. The current frame-less biopsy is both stable and precise, but we also consider the Leksell system to have excellent structural stability and accuracy. Furthermore, familiarity with the Leksell system can be a significant advantage. Combining our method with the current Leksell system ensures surgical comfort and stability without additional burden.
CONCLUSION
By utilizing established methodologies, we anticipate that added expertise can improve the consistency and manageability of stereotactic biopsies for infratentorial tumors. This can streamline surgical preparation, ensure adequate tissue samples, and reduce patient complications. Similarly, further knowledge can enhance the stability and comfort for the operator performing a biopsy of the posterior fossa, thereby minimizing potential difficulties and risks.